Feasibility of hybrid telerehabilitation as a component of the Managed Care after Acute Myocardial Infarction (MC-AMI) program in a 12-month follow-up: experience from a single center
Key words: comprehensive care program, hybrid telerehabilitation, myocardial infarction



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Feasibility of hybrid telerehabilitation as a component of the Managed Care after Acute Myocardial Infarction (MC-AMI) program in a 12-month follow-up: experience from a single center
Introduction: Managed Care after Myocardial Infarction (MC‑AMI [KOS‑Zawał]), a comprehensive care program dedicated to patients after myocardial infarction, was implemented in Poland in 2017. Hybrid cardiac telerehabilitation (HTR) is a unique component of MC‑AMI.
Objectives: We evaluated the feasibility of HTR as a component of MC‑AMI and assessed its safety and acceptance by patients. One‑year all‑cause mortality among the patients participating and not participating in MC‑AMI was analyzed.
Patients and methods: The MC‑AMI group included 114 patients who underwent a 5‑week HTR program comprising telemonitored Nordic walking training sessions, and who completed the entire 12‑month MC‑AMI program. The influence of HTR on the physical capacity was assessed by comparing the stress test results before and after HTR. After HTR, the patients completed a satisfaction survey to assess their acceptance of the program. The non–MC‑AMI group was formed using propensity score matching to compare 1‑year all‑cause mortality between the patients participating and not participating in MC‑AMI.
Results: HTR significantly improved the functional capacity assessed in the stress test and was well‑received by the patients. In the study group, nonfatal non–ST‑segment elevation myocardial infarction, elective coronary percutaneous intervention, and cardiovascular hospitalization occurred in 0.9%, 2.6% and 6.1% of the patients, respectively. There were no deaths among the MC‑AMI participants, whereas in the non–MC‑AMI group, 1‑year all‑cause mortality was 3.5%. The log‑rank test comparing the survival probabilities of matched groups, estimated by the Kaplan–Meier method, showed heterogeneity of the curves (P = 0.04).
Conclusions: HTR as a component of MC‑AMI was a feasible, safe, and well‑accepted form of cardiac rehabilitation. Participation in MC‑AMI including HTR was associated with a significantly lower risk of 1‑year all‑cause mortality, as compared with not taking part in the rehabilitation program.
What's new?
In the last several years, the dynamic development of technology has enabled the inclusion of telemedicine in the organization of outpatient cardiologic care. One of the examples is hybrid telerehabilitation (HTR), which proposes the use of remote monitoring components (eg, telecare, electrocardiography telemonitoring) with telesupervised exercise training. Thanks to innovative solutions, HTR has become a unique, home‑based form of cardiac rehabilitation that overcomes the barriers to rehabilitation, thus eliminating health care inequalities and, at the same time, providing guideline‑consistent monitoring of physical training. Our study demonstrated the beneficial effects of HTR and confirmed its feasibility, safety, and acceptance by the patients. The results of the current study provided arguments for a wider implementation of HTR in routine clinical practice (such as in the Managed Care after Acute Myocardial Infarction program [KOS‑Zawał]), which can lead to an increased level of participation in cardiac rehabilitation and contribute to improved long‑term cardiovascular risk management and prognosis.
Introduction
According to World Health Organization data, ischemic heart disease, including myocardial infarction (MI), is currently the leading cause of death globally, regardless of the income group a country belongs to.1 Significant advances in the management of coronary artery disease (better and more timely access to acute care after MI, improved revascularization procedures, and drug treatment) in the last 2 decades have contributed to the reduction of in‑hospital mortality rates in the acute MI phase. The 30‑day mortality rate after MI has decreased substantially between 2007 and 2017. This indicator of acute care quality decreased by approximately 30% on average from 9.2% to 6.5% in the European Union countries (including Poland).2,3 Despite these advances, high mortality rate within 12 months after discharge remains a challenge. In Poland, 1‑year mortality (counted starting from the admission to the hospital) was 17.3%, and 1‑year postdischarge mortality was 9.8% in 2018.4 Several analyses pointed out the lack of lifestyle modifications, including in adequate physical activity, suboptimal control of cardiovascular risk factors, and limited access to specialized health care facilities, as the most important reasons for a poor prognosis in the 12‑month follow‑up after MI.5 The authors concluded that to improve the outcomes, emphasis should be placed on facilitating access to outpatient cardiac care, particularly cardiac rehabilitation, and on optimal management of modifiable risk factors.
Despite the guideline recommendations and proven benefits of secondary prevention reflected by mortality reduction, cardiac rehabilitation programs remain highly unavailable and underutilized.6-8 In Poland, according to the latest data, 35% of acute MI survivors participate in cardiac rehabilitation within 365 days following discharge, but only 19% do so within the first 30 days.4,9
For these reasons, at the end of 2017, after identifying the most important determinants of high post‑MI mortality rate (eg, poor control of risk factors, insufficient and delayed cardiac rehabilitation, suboptimal pharmacotherapy), the Polish Cardiac Society, the National Health Fund, and the Ministry of Health launched Managed Care after Acute Myocardial Infarction (MC‑AMI [KOS‑Zawał]), a novel, comprehensive, nationwide care program for MI survivors. This new program comprised individualized cardiac rehabilitation and secondary prevention for MI patients over 12 months after hospital discharge.10 The main goals of this program were to enhance the quality of cardiologic care as well as to improve survival rates and prognosis of patients after MI.
MC‑AMI was implemented in Poland on October 1, 2017. The program includes an acute intervention, complex revascularization, implantation of cardiovascular electronic devices (in case of indications), cardiac rehabilitation or hybrid telerehabilitation (HTR), and scheduled outpatient follow‑up.11 HTR is a unique component of the program, and it is worth noting that the guidelines of the European and American cardiologic scientific societies indicate HTR as a promising novel approach, pointing to its safety, effectiveness, and high patient adherence.12,13 The joint expert opinion of the Polish Cardiac Society and the Polish Academy of Sciences considers comprehensive HTR a procedure equivalent to inpatient or outpatient rehabilitation.14 The aim of this paper was to evaluate the feasibility, safety, and acceptance of HTR as a component of the novel care program after MI, and to assess the mortality and major adverse cardiovascular events (MACEs) over a 12‑month follow‑up.
Patients and methods
Patients
In our single‑center, retrospective analysis, the study group consisted of patients with MI admitted to the National Institute of Cardiology (Warsaw, Poland) between January 1, 2018, and July 31, 2021, who agreed to participate in the 12‑month MC‑AMI program. Cardiac rehabilitation was one of the core modules of the MC‑AMI program. Before discharge from the hospital, the patients were referred for cardiac rehabilitation (telerehabilitation or center‑based rehabilitation) according to indications and their preferences. Telerehabilitation was an alternative to center‑based rehabilitation. The participants who preferred HTR were referred to the Telecardiology Center for a screening visit (scheduled 7–14 days after discharge) to assess their eligibility for HTR.
Propensity score matching method
The control group consisted of patients diagnosed with MI, discharged from the Institute at the same time, and not participating in the MC‑AMI program. We did not include individuals with contraindications to HTR in the control group. Propensity score matching encompassing greedy nearest neighbor matching (1:1) without replacement, using well‑balanced variables listed in Table 1, was applied to form comparable groups of patients participating and not participating in the MC‑AMI program. The propensity score was calculated using the logistic regression.
Parameter | Patients participating in MC‑AMI (n = 114) | Matched patients not participating in MC‑AMI (n = 114) | P value |
All results for categorical variables are presented as numbers and percentages and for continuous variables as means (SD).
Abbreviations: ACS, acute coronary syndrome; AF, atrial fibrillation; CABG, coronary artery bypass grafting; CAR, coronary artery revascularization; CKD, chronic kidney disease; LVEF, left ventricular injection fraction; MC‑AMI, Managed Care after Acute Myocardial Infarction; MI, myocardial infarction; MINOCA, myocardial infarction with nonobstructive coronary arteries; NSTEMI, non–ST‑segment elevation myocardial infarction; PCI, percutaneous coronary intervention; STEMI, ST‑segment elevation myocardial infarction | |||
Male sex | 99 (86.8) | 98 (86) | >0.99 |
Age, y | 59.1 (9.5) | 59 (9.1) | 0.92 |
LVEF, % | 54.6 (7.4) | 54.5 (8.8) | 0.94 |
ACS on admission | |||
STEMI | 70 (61.4) | 65 (57) | 0.45 |
NSTEMI | 43 (37.7) | 49 (43) | |
MINOCA | 1 (0.9) | 0 | |
Medical history | |||
Hypertension | 77 (67.5) | 79 (69.3) | 0.77 |
Diabetes | 20 (17.5) | 19 (16.7) | 0.86 |
Hyperlipidemia | 96 (84.2) | 95 (83.3) | 0.85 |
Paroxysmal AF | 8 (7) | 8 (7) | 1 |
CKD | 0 | 0 | 1 |
Previous MI | 9 (7.9) | 6 (5.3) | 0.42 |
STEMI | 3 (2.6) | 2 (1.7) | >0.99 |
NSTEMI | 6 (5.3) | 4 (3.5) | 0.51 |
Previous CAR | 18 (15.8) | 19 (16.7) | 0.85 |
PCI | 15 (13.2) | 13 (11.4) | 0.68 |
CABG | 6 (5.3) | 6 (5.3) | 1 |
Each patient participating in MC‑AMI was matched with 1 patient not participating in the program but similar in terms of the other independent variables, which resulted in comparable risk prediction after MI between the groups.
Inclusion and exclusion criteria for hybrid telerehabilitation
The clinical indications and contraindications to HTR did not differ from those applying to center‑based cardiac rehabilitation.6,14 The essential eligibility criteria for HTR were the patient’s consent, ability to exercise on their own, and adherence to remote cooperation with the monitoring team.14 Contraindications to HTR included all unstable medical conditions: unstable angina, uncontrolled hypertension, severe pulmonary hypertension, decompensated congestive heart failure, symptomatic or complex ventricular arrhythmias, valvular or congenital heart disease that required surgical treatment, anemia (hemoglobin <11 g/dl), febrile diseases or severe systemic diseases, any musculoskeletal or neurologic conditions that precluded physical exercise, disturbed balance, and increased the risk of falling, and severe psychiatric disorders or significant cognitive impairment.5,15,16
Description of the Managed Care after Acute Myocardial Infarction program
MC‑AMI consists of 4 modules: optimal strategy for complete revascularization, cardiac rehabilitation (in an outpatient clinic, hybrid home‑based and monitored, or inpatient rehabilitation in the hospital rehabilitation ward), electrotherapy (including implantable cardioverter‑defibrillator or cardiac resynchronization therapy) when appropriate, and outpatient care provided by a specialist within 12 months after MI. At the first screening visit (7–14 days after discharge), in addition to a clinical assessment, electrocardiography (ECG), and basic blood tests, the patients were referred for cardiac rehabilitation as a core component of MC‑AMI. Upon completion of the rehabilitation, at least 3 visits to a cardiologist were scheduled, 6 weeks, 4 months, and 9 months after MI, respectively. The number of consultations at the outpatient cardiology clinic during the 12‑month program was adjusted to the individual patient’s condition. The clinical assessment and echocardiography performed 6 weeks after discharge from the hospital identified the patients eligible for electrotherapy. The program also offered the possibility of a second‑stage percutaneous coronary intervention to perform functionally complete revascularization for eligible patients. The last summary follow‑up visit was scheduled at the end of the program.
Description of hybrid telerehabilitation
The detailed methodology of HTR was presented in several previous papers.15,17 HTR delivered all core components, such as obtaining clinical stabilization, cardiovascular risk reduction, disability reduction, psychosocial and vocational support, change in lifestyle behaviors, and self‑management. HTR was delivered by a medical team (cardiologists, physiotherapists, nurses, and psychologists) using advanced monitoring systems. Patient eligibility for HTR was assessed during the MC‑AMI screening visit. Before HTR, all patients underwent a medical check‑up, blood tests (complete blood count, potassium, sodium, creatinine, C‑reactive protein), and resting ECG. If necessary, echocardiography or 24‑hour Holter ECG recordings were also performed.
At baseline, each patient performed a symptom‑limited exercise treadmill stress test according to the Bruce or modified Bruce protocol to tailor HTR to the patient’s exercise capacity. Individual rehabilitative goals for each patient were established. The target training heart rate was between 50% and 70% of the heart rate reserve calculated using the Karvonen formula. After the completion of HTR, the exercise stress test (always following the same protocol for a particular individual before and after HTR) was repeated to assess the effectiveness of the rehabilitation. HTR consisted of 2 stages: an initial stage (1 week) conducted in an outpatient clinic and a basic stage (4 weeks) comprising telemonitored Nordic walking training sessions conducted at home, 5 times a week. During the initial stage, the patients were taught how to self‑evaluate their condition, measure their heart rate, blood pressure, and body mass, how to perform the exercise training and evaluate the level of perceived exertion according to the Borg scale, and finally, how to operate the telerehabilitation set. They also participated in 5 monitored educational training sessions.
Telemonitoring
Telemedicine offers the possibility to remotely supervise exercise training. The monitoring system used in our study included a wireless device for tele‑ECG–supervised exercise training, a data transmission set via a cellphone network, and a monitoring center capable of receiving and storing patient medical data. The device stored individually preprogrammed training sessions for each patient (with defined duration, breaks, and timing of the ECG recording), and was capable of recording ECG data from 3 precordial leads. We used the sequential ECG monitoring method for HTR supervising. The device recorded 4 ECGs (each lasting 16 s) during a single training session. The first ECG was obtained as part of the preliminary examination before the training, and the next 3 were recorded during the exercise training, each at the end of a prespecified training interval, during maximal effort. Additionally, in the case of an emergency event, the patient could upload an additional ECG (features of event‑Holter). We did not use real‑time monitoring. The system was used to monitor and control training at any place the patient wanted to exercise.
Exercise training
Each home‑based HTR training session consisted of 2 parts: a consent procedure and a proper training session. Before each training session, the patient answered a series of questions regarding their current physical condition, including fatigue, dyspnea, blood pressure, body mass, and medications taken. The patient then transmitted the resting ECG data to the monitoring center. The medical staff also analyzed the data sent from remote monitoring of cardiovascular implantable electronic devices, if available. If no contraindications were identified, the patient was allowed to start the training session. If the training session was completed uneventfully, the patient would transmit the ECG recording to the monitoring center immediately after the end of each training session.
Education
The ultimate goals of therapeutic education were to promote self‑care, healthy lifestyle behavior, and the responsibility of patients for their own treatment. During the initial stage of HTR, cardiologists conducted 3 educational sessions focused on the identification and reduction of risk factors, lifestyle changes, and optimization of treatment. The patients received recommendations regarding an adequate diet, smoking cessation, blood pressure control, and other risk factors. They were also instructed on the beneficial effect of physical activity as part of post‑MI management. The patients participated in workshops on first aid provision, including the principles of using an automated external defibrillator available in public spaces.
Psychological support
During the initial stage of HTR, the patients had 2 consultations with a psychologist, and there was a possibility of further psychosocial support. Help in dealing with psychosocial and professional problems of the patients was often the objective of the psychological support. In the case of psychiatric problems, such as anxiety or depression, relatively common after coronary events, a psychiatric consultation was sometimes recommended by the psychologist.
Assessment of patient acceptance of hybrid telerehabilitation
After completing HTR, the participants filled out a patient satisfaction questionnaire. We developed a 12‑question questionnaire to collect feedback from the patients to measure their acceptance of and satisfaction with HTR (Table 2).
Question | Answer, n (%) | ||
Abbreviations: ECG, electrocardiography; HRT, hybrid telerehabilitation | |||
Did you control the device yourself? | |||
Yes | 113 (99.1) | ||
No | 1 (0.9) | ||
How would you assess the difficulty of operating the device? | |||
Very easy | 68 (59.6) | ||
Easy | 46 (40.4) | ||
Difficult | 0 | ||
Very difficult | 0 | ||
Was it difficult to accurately place the electrodes on your skin? | |||
Yes | 2 (1.7) | ||
No | 112 (98.3) | ||
Did you observe any significant skin reaction to the electrodes? | |||
Yes | 8 (7) | ||
No | 106 (93) | ||
When using the equipment provided to communicate with the monitoring center, was the sound quality satisfactory? | |||
Yes | 108 (94.7) | ||
No | 6 (5.3) | ||
Did you find it difficult to coordinate the exercise with the instructions on the device? | |||
Yes | 0 | ||
Sometimes | 6 (5.3) | ||
No | 108 (94.7) | ||
Was it difficcult to the transmit the data (ECG, blood pressure)? | |||
Yes | 1 (0.9) | ||
Sometimes | 14 (12.3) | ||
No | 99 (86.8) | ||
Did you ever miss a telerehabilitation session due to technical problems? If so, how many times? | |||
Yes | 15 (13.2) | ||
Number of missed sessions, mean (SD); median (min–max) | 1.9 (1.2); 1 (1–5) | ||
When did you use the telemedicine equipment? | |||
Only during exercise | 109 (85.6) | ||
During exercise and when feeling unwell | 5 (4.4) | ||
Did HTR motivate you to exercise? | |||
Yes | 111 (97.4) | ||
Sometimes | 2 (1.7) | ||
No | 1 (0.9) | ||
Did you feel safer during HTR than when you exercised at home without supervision? | |||
Yes | 101 (88.6) | ||
No | 13 (11.4) | ||
Did HTR increase the following aspects of your daily activity? | |||
Physical exercise | Yes | 106 (93) | |
No | 8 (7) | ||
Mental | Yes | 107 (93.9) | |
No | 7 (6.1) | ||
Social | Yes | 80 (70.2) | |
No | 34 (29.8) | ||
Professional | Yes | 40 (35.1) | |
No | 74 (64.9) | ||
Sexual | Yes | 39 (34.2) | |
No | 75 (65.8) | ||
Assessment of adherence to hybrid telerehabilitation and the Managed Care after Acute Myocardial Infarction program
Daily telephone contact with the monitoring center was chosen as part of the consent procedure to assess HRT adherence. It was required to obtain permission to attend the training session. Adherence to MC‑AMI was evaluated by assessing the patient’s participation in telerehabilitation and the number of mandatory specialist visits. The patients were considered adherent if they participated in telerehabilitation and underwent all mandatory visits included in the 12‑month MC‑AMI program.
Assessment of hybrid telerehabilitation safety
When assessing the safety of HTR, we took into account all serious cardiovascular events and complications (eg, angina symptoms, dyspnea, complex ventricular arrhythmia, serious atrioventricular blocks) that occurred during telemonitored exercise training sessions and up to 1 hour afterward.
Assessment of the effect of hybrid telerehabilitation on exercise capacity
Exercise capacity and cardiovascular response to exercise were assessed during the exercise stress test, in line with the guidelines.18 A symptom‑limited exercise stress test was performed according to the Bruce protocol before and after the HTR program. The stress test before the HTR program was treated as a baseline. In our study population, we analyzed maximal exercise capacity (as measured by the metabolic equivalents of task [METs]), exercise duration, heart rate at rest and at maximal effort, blood pressure during exercise, and double product (ie, the product of heart rate and systolic blood pressure at rest and at the maximal effort).
One‑year follow‑up assessment
Mortality (all‑cause and cardiovascular), MACEs (including recurrent MI, stroke, and repeat coronary revascularization intervention), and cardiovascular hospitalization data were collected during the 12‑month follow‑up of the MC‑AMI program. We also analyzed and compared 1‑year all‑cause mortality between the patients participating and not participating in the MC‑AMI program.
Statistical analysis
All results for categorical variables are presented as numbers and percentages, and for continuous variables as means (SD). The normality of the distribution of continuous data and their changes over time were verified using the Shapiro–Wilk test. The paired t test was used to evaluate the statistical significance of differences in changes over time. The validity of logistic regression was assessed using the Hosmer–Lemeshow goodness‑of‑fit test. The model was well calibrated (χ2 = 7.91; P = 0.44), and yielded a concordance index (C index) of 0.73 (95% CI, 0.68–0.78; P <0.001). For matched groups, logistic regression results were as follows: the Hosmer–Lemeshow goodness‑of‑fit test, χ2 = 8.23; P = 0.41; C‑index, 0.54 (95% CI, 0.47–0.62); P = 0.99. The 2 groups (MC‑AMI and matched non–MC‑AMI) were compared using the χ2 test or the Fisher exact test (when the number of expected events in cells was lower than 5) for categorical variables and the independent t test for continuous data. The Kaplan–Meyer curves were used to present the time to event (mortality) outcome, and the 2 groups were compared using the log‑rank test. P values below 0.05 were considered significant. Statistical analyses were performed using SAS software, version 9.4 (SAS Institute Inc., Cary, North Carolina, United States).
Results
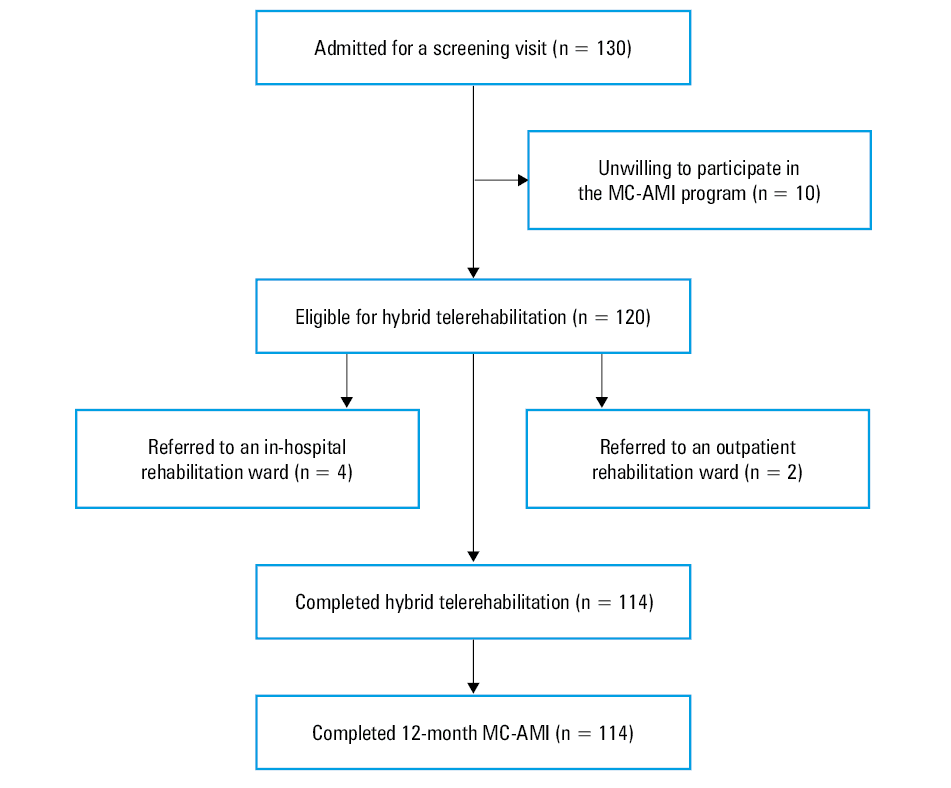
Between January 1, 2018 and July 31, 2021, a total of 130 consecutive patients with a diagnosis of MI, before discharge from the National Institute of Cardiology, gave their consent to participate in the 12‑month MC‑AMI program, with HTR as the chosen form of the cardiac rehabilitation. All the patients were referred to the Telecardiology Center for an HTR screening visit (Figure 1).
Abbreviations: see Table 1
Out of the 130 patients, 10 refused to participate in the MC‑AMI program due to personal obligations, and 6 were referred to the outpatient cardiac rehabilitation unit (2 patients due to their choice) or to the in‑hospital rehabilitation unit (4 patients with serious comorbidities and frailty). Finally, 114 patients (study group) participated in HTR and completed it. Each of them also completed the entire 12‑month MC‑AMI program. Using 1:1 propensity score matching, we formed a control group consisting of 114 out of 306 patients diagnosed with MI, discharged from the Institute in the same time frame, and not participating in MC‑AMI.
The demographics and clinical background of both groups are shown in Table 1.
Acceptance of hybrid telerehabilitation
All patients completed the acceptance questionnaire at the end of HTR. The program generally achieved very good rates. According to all participants, the telerehabilitation set was easy or very easy to use. Only 1 patient declared that they needed some help of the family to operate the telemonitoring device. Importantly, daily contact with the monitoring center and supervised training sessions motivated 97% of the patients to exercise. Eighty‑eight per cent of them evaluated the safety of HTR as better than training at home without supervision. The vast majority of the participants (>90%) declared that participation in HTR contributed to an increase in their daily physical and mental activity. Due to the temporary lack of coverage of the cellular network, 15 participants (13%) missed a few exercise sessions. However, all of them managed to complete all 20 training sessions. Detailed answers to individual questions are presented in Table 2.
Adherence to hybrid telerehabilitation and the Managed Care after Acute Myocardial Infarction program
The adherence to HTR was the highest possible. All 114 participants completed HTR by participating in all planned training sessions. However, 2 of them did not undergo the final exercise stress test; 1 patient because of anemia caused by acute rectal bleeding due to radiation proctitis, and 1 patient due to symptoms of heart failure exacerbation that developed after the end of HTR and did not require hospitalization. The same high level of adherence was achieved with respect to MC‑AMI, as all the patients completed the entire program.
Safety of hybrid telerehabilitation
There were no deaths or other serious adverse events (eg, angina symptoms, dyspnea, exercise‑induced hypotension, complex ventricular arrhythmia, atrioventricular block) during the telemonitored Nordic walking sessions and up to 1 hour after the training. The patients also did not report any significant symptoms that would require discontinuation of the training session.
Effects of hybrid telerehabilitation on physical capacity
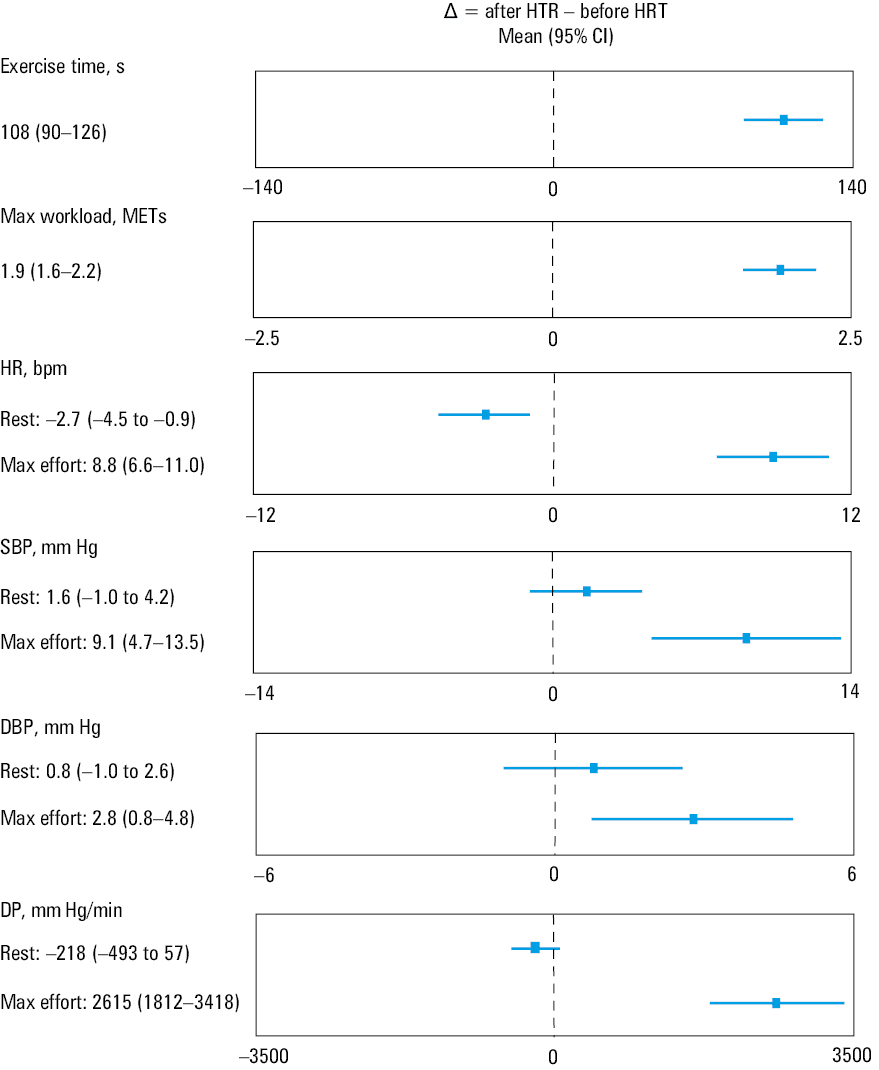
The analysis revealed significant changes in exercise stress test results before and after HTR (Figure 2). A significant increase in exercise duration and maximal exercise capacity were observed in the exercise stress test performed after HTR (Table 3). Furthermore, heart rate, blood pressure, and double product at maximal effort also increased significantly after rehabilitation, whereas the resting heart rate decreased significantly.
Abbreviations: see Table 3
Exercise test result | Before HTR | After HTR | P value |
All results for continuous variables are presented as means (SD).
Differences were considered significant at P <0.05.
Abbreviations: DBP, diastolic blood pressure; DP, double product; HR, heart rate; MET, metabolic equivalent; SBP, systolic blood pressure; others, see Table 2 | |||
Exercise time, s | 361 (112) | 469 (142) | <0.001 |
Maximal workload, METs | 7.8 (2) | 9.7 (2.6) | <0.001 |
HR at rest, bpm | 69.7 (11.5) | 67.0 (10.1) | 0.004 |
HR at max effort, bpm | 122.9 (16.2) | 131.7 (18.1) | <0.001 |
SBP at rest, mm Hg | 120.1 (15.8) | 121.7 (15.3) | 0.21 |
DBP at rest, mm Hg | 76.4 (10.2) | 77.1 (8.8) | 0.37 |
SBP at max effort, mm Hg | 164 (26.8) | 173.1 (26.1) | <0.001 |
DBP at max effort, mm Hg | 81.6 (11.9) | 84.4 (10.7) | 0.007 |
DP at rest | 8396 (1873) | 8178 (1684) | 0.11 |
DP at max effort | 20 339 (1984) | 22 954 (5413) | <0.001 |
One‑year follow‑up
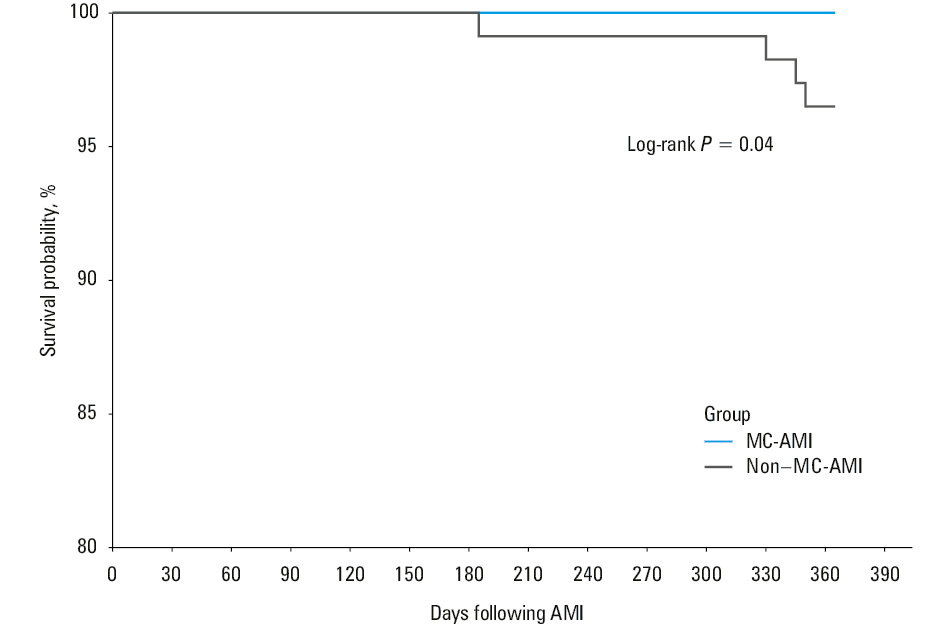
In the study group there were no deaths during the 12‑month follow‑up, and MACEs were rare. Only 1 patient (0.9%) experienced a recurrent nonfatal non–ST‑segment elevation MI 7 months after the first MI. Elective percutaneous coronary intervention was performed in 3 individuals (2.6%). Furthermore, 7 patients (6.1%) required hospitalization for cardiovascular reasons. The most common cause of hospital admission was chest pain (5 patients). All of them underwent coronary angiography, and in 1 case coronary vasospasm with negative troponin was diagnosed. The remaining patients did not need any coronary intervention. The other 2 patients needed hospitalization for elective cardioversion of persistent atrial fibrillation and elective interventional treatment of peripheral artery disease, respectively. The 1‑year all‑cause mortality among the MC‑AMI participant was 0% (0/114), whereas in the non–MC‑AMI group it was 3.5% (4/114). The log‑rank test comparing the survival probabilities of the matched groups, estimated by the Kaplan–Meier method, showed heterogeneity of the curves (P = 0.04) (Figure 3).
Abbreviations: see Table 1
Discussion
Despite its well‑established benefits, cardiac rehabilitation is still underused in patients who experienced MI. Attendance at ambulatory rehabilitation programs was reported as unsatisfactory and low.19 Telemedicine has become one of the methods that overcome barriers to accessing cardiac rehabilitation. Over the last decade, several studies have shown that HTR is a feasible, effective, and safe form of cardiac rehabilitation, with high adherence and good patient tolerance.15,20-22 Therefore, our center implemented HTR as an element of MC‑AMI.
Acceptance of and adherence to hybrid telerehabilitation
Our study showed that the adherence to HTR was high and most of the patients received it well. The level of adherence to telerehabilitation was reported at approximately 90% or more in several previous studies.15,20,22 There is no doubt that achieving good acceptance of HTR contributes to high adherence. The best measure of patient acceptance in our study was the claim that HTR stimulated and motivated the patients to exercise, which was made by over 90% of the participants. In all of the quoted studies,15,16,20,21,23 the patients did not mention any significant difficulties related to the operation of the telemonitoring devices, and considered them easy to use.
A few publications on HTR confirmed that adherence to this form of cardiac rehabilitation is superior to the adherence to center‑based rehabilitation.16,23 Tang et al24 revealed also that the preference of patients to participate in home‑based or outpatient clinic rehabilitation appears to be equivalent and provides similar health benefits.
Safety of hybrid telerehabilitation
The lack of serious adverse events during training sessions demonstrated the safety of HTR and confirmed the results of previous studies,3,15,22,23 including TELEREH–HF (Telerehabilitation in Heart Failure Patients),20 the largest randomized clinical trial introducing comprehensive HTR in heart failure patients. In 2 studies,15,16 the participants considered the safety of HTR to be higher than when training at home without supervision. As pointed out by Piotrowicz et al,22 despite the fact that telerehabilitation took place far from the medical center, the participants felt safe thanks to remote monitoring and supervision modalities. In their review, Batalik et al19 analyzed 12 studies on cardiac telerehabilitation, and found that no serious cardiovascular complications or deaths were recorded during the interventions described in any of the studies.
Undoubtedly, 3 crucial factors had a significant impact on the safety of HTR. The first factor was the appropriate qualification for telerehabilitation according to the guidelines that provide all indications and contraindications to this training. The second factor was the optimalization of exercise training modalities (eg, type, intensity, method) based on the clinical status and results of the exercise stress test. The last factor affecting HTR safety was the daily eligibility assessment before the training session (consent procedure).
Effects of hybrid telerehabilitation on physical capacity
The improvement in physical capacity observed in our study (significant increase in exercise duration and maximal exercise capacity on a treadmill after HTR) is consistent with data from other studies and confirms the effectiveness of HTR. In their review, Prabhu et al25 concluded that in most studies, both types of cardiac rehabilitation programs (center- and home‑based ones) are equally effective in improving individual functional capacity. The results of the TeleInterMed study15 indicated that the distance in the 6‑minute walk test, exercise duration, and physical capacity improve significantly in stable individuals after home‑based cardiac telerehabilitation. Szalewska et al21 also showed that HTR was effective in coronary artery disease patients with and without diabetes. The patients in both groups exhibited a significant increase in their maximal workload on the exercise stress test after HTR. Finally, the TELEREH‑HF study20 demonstrated a significant improvement in the the 6‑minute walking distance and peak oxygen consumption in the cardiopulmonary exercise test after HTR in the rehabilitation group, as compared with standard care.20
One‑year follow‑up
There were no deaths and only a small number of MACEs and cardiovascular hospitalizations during the 12‑month follow‑up in our study group. The 1‑year all‑cause mortality was significantly lower in the study group than in the patients not participating in MC‑AMI. These data confirmed the results obtained in other centers that run the MC‑AMI program or analyzed its results.26-30 In the 2 largest nation‑wide analyses of MC‑AMI effectiveness,26,27 participation in the program was related with improved prognosis. Jankowski et al26 reported that 1‑year all‑cause mortality was 4.4% among the participants (n = 10 404) and 9.5% among those who did not participate in the program (n = 77 335). A survival analysis performed by Kubielas et al27 revealed a significantly lower (P <0.001) probability of death in the MC‑AMI than in the non–MC‑AMI group.27 The authors concluded that AC‑AMI reduced the risk of death in the first year post‑MI by 29%. Wita et al28,29 revealed that participation in MC‑AMI was related to a reduction in the rate of MACEs by 45% in a 3‑month observation, and to a reduction in 1‑year mortality by 38%. The authors emphasized that among the components of MC‑AMI, cardiac rehabilitation (hazard ratio [HR], 0.34) and strict outpatient care (HR, 0.42) were the essential factors affecting the reduction in mortality. Gąsior et al30 also confirmed the improved prognosis of the population who participated in MC‑AMI. The authors showed that participation in MC‑AMI was associated with lower rates of stroke, heart failure hospitalizations, and all‑cause mortality over a 12‑month follow‑up. MC‑AMI was also an independent factor of 12‑month survival in MI survivors with pre‑existing heart failure.
As compared with standard care, MC‑AMI improved the prognosis by increasing the rate of patients undergoing cardiac rehabilitation, complete revascularization, and implantation of cardiovascular electronic devices.11
Study limitations
The results should be interpreted in the context of the study limitations. Firstly, the relatively small number of patients weakens the strength of our conclusions. We acknowledge that studies with a larger number of participants are needed to confirm the results of our current work. More evidence is required to confidently confirm that additional health benefits are observed in HTR patients.
Secondly, our study group included relatively young individuals (mean age, 59.1 years) with quite high left ventricular ejection fraction (LVEF; mean, 54.6%) and good physical capacity at baseline (mean, 7.9 MET in the exercise treadmill stress). Such baseline characteristics could have contributed to better prognosis during the follow‑up.
Conclusions
Our study demonstrated that HTR was a feasible and effective form of cardiac rehabilitation in the MC‑AMI program. A significant increase in exercise duration, maximal exercise capacity, and double product at the maximal effort was observed in the exercise stress test after HTR, as compared with the test performed at baseline. The intervention was well accepted by the patients, including the need for daily interaction and collaboration with the monitoring center. The level of adherence to HTR, as well as to MC‑AMI, was very high, and outcomes at the 12‑month follow‑up seem promising. Participation in MC‑AMI including HTR was associated with a significantly lower risk of 1‑year all‑cause mortality, as compared with individuals who did not take part in the program. It should be emphasized that our study group was relatively young, with preserved LVEF, and good physical capacity at baseline. Therefore, our conclusions could be applied to a highly selected, low‑risk population of patients with MI.
- Nowbar AN, Gitto M, Howard JP, et al. Mortality from ischemic heart disease. Circ Cardiovasc Qual Outcomes. 2019; 12: e005375. | Crossref
- OECD/European Union. Health at a Glance: Europe 2020: State of Health in the EU Cycle. Paris: OECD Publishing; 2020.
- Santos IS, Goulart AC, Brandão RM, et al. One‑year mortality after an acute coronary event and its clinical predictors: the ERICO study. Arq Bras Cardiol. 2015; 105: 53‑64. | Crossref
- Jankowski P, Topór‑Mądry R, Gąsior M, et al. Management and predictors of clinical events in 75 686 patients with acute myocardial infarction. Kardiol Pol. 2022; 80: 468‑475. | Crossref
- Piepoli MF, Hoes AW, Agewall S, et al. 2016 European guidelines on cardiovascular disease prevention in clinical practice: the Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts); Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J. 2016; 37: 2315‑2381.
ARTICLE INFORMATION