The role of 18F-fluorodeoxyglucose positron emission tomography / computed tomography imaging in the diagnosis of valve-in-valve endocarditis



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
The role of 18F-fluorodeoxyglucose positron emission tomography / computed tomography imaging in the diagnosis of valve-in-valve endocarditis
Infective endocarditis (IE) is a rare condition with an in‑hospital mortality of 17.1% and 1‑year mortality of up to 40%.1,2 It usually occurs in patients from high‑risk groups, such as those with prosthetic valves or with prosthetic material used for cardiac valve repair, those with previous IE, or those with untreated cyanotic congenital heart disease.3 The recurrence rate is between 2% and 6%.3 If IE occurs at least 6 months after the previous infection, it indicates a reinfection.3
In March 2022, a 79‑year‑old man was admitted to the hospital for a suspected IE reinfection. The patient had undergone coronary artery bypass grafting and a biological aortic valve implantation in 2018, followed by IE in 2019. The infection destroyed the aortic valve leaflets, which led to severe aortic valve failure. In 2021, the patient had undergone a valve‑in‑valve transcatheter aortic valve implantation (TAVI), followed by a percutaneous therapy for severe mitral regurgitation with the MitraClip system 7 months later. He also had chronic kidney disease and had undergone an appendectomy 2 months before the admission.
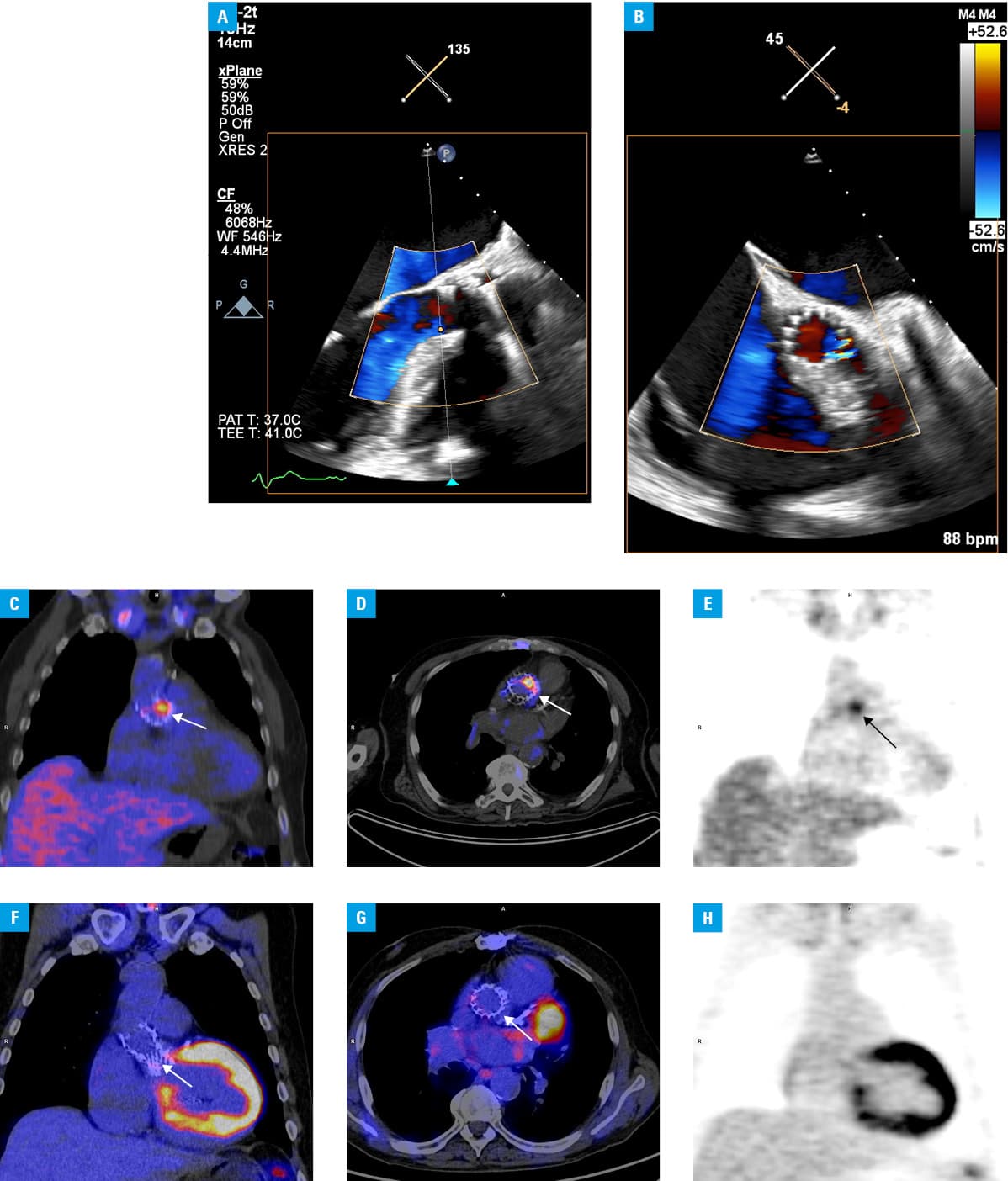
The patient presented with fever (up to 40 °C) and shivering but had no symptoms related to the respiratory or urinary system. Physical examination revealed a heart rate of 76 bpm, blood pressure of 90/50 mm Hg, a systolic‑diastolic heart murmur, crackles at the base of the lungs, and no peripheral edema. The level of C‑reactive protein was significantly elevated (192 mg/l; reference range <10 mg/l). Blood culture was positive for Staphylococcus hominis and Escherichia coli. According to the antibiogram, antibiotic therapy with ceftriaxone, vancomycin, and amikacin was implemented. Transthoracic and transesophageal echocardiography was performed, and neither showed any features of IE (Figure 1A and 1B). However, there was still a high probability and suspicion of IE as the patient belonged to a high‑risk group (previous IE, presence of prosthetic valve material). Hence, after implementation of a low‑carbohydrate / high‑fat diet and the administration of 2500 IU of heparin on the second day of antibiotic therapy, whole‑body 18F‑fluorodeoxyglucose positron emission tomography / computed tomography (18F‑FDG PET/CT) was performed. Inflammatory activity was found in the aortic valve annulus and at the arterio‑superior part of the ascending aorta (Figure 1C–1E). No extracardiac foci were detected. Thus, after the PET/CT scan, the 2 main Duke criteria were met (2 positive blood cultures for IE and positive imaging results for IE), and the diagnosis of IE was confirmed. The patient received antibiotic therapy for 6 weeks. Five months later, a follow‑up 18F‑FDG PET/CT scan showed no evidence of infection in the aortic valve (Figure 1F–1H).
In further retrospective analysis, the appendectomy performed 2 months before the admission to the hospital was evaluated as a likely source of infection. E. coli is not a typical etiologic agent of IE—only a few such cases have been described in the literature. Native valves without degenerative valvulopathy appear to be more susceptible to E. coli than prosthetic valves.4
The incidence of IE as a complication of TAVI is estimated at 0.2% to 3.1%.5 However, the incidence of endocarditis after a valve‑in‑valve procedure is not yet known, as it is not the standard procedure after IE. Such a scenario has not been described in recent publications. The case presented here demonstrates that 18F‑FDG PET/CT can be a valuable tool in the diagnosis of valve‑in‑valve endocarditis, as the number of cases of this infection will likely grow due to the increasing availability of percutaneous procedures.
- Habib G, Erba PA, Iung B, et al. Clinical presentation, aetiology and outcome of infective endocarditis. Results of the ESC‑EORP EURO‑ENDO (European infective endocarditis) registry: a prospective cohort study. Eur Heart J. 2019; 40: 3222‑3232.
- Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology / American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2021; 77: 25‑197.
- Habib G, Lancellotti P, Antunes MJ, et al. 2015 ESC Guidelines for the management of infective endocarditis: the Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio‑Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J. 2015; 36: 3075‑3128. | Crossref
- Akuzawa N, Kurabayashi M. Native valve endocarditis due to Escherichia coli infection: a case report and review of the literature. BMC Cardiovasc Disord. 2018; 18: 195. | Crossref
- Harding D, Cahill TJ, Redwood SR, Prendergast BD. Infective endocarditis complicating transcatheter aortic valve implantation. Heart. 2020; 106: 493‑498. | Crossref
ARTICLE INFORMATION