Impact of smoking on outcomes in patients with ST-segment elevation myocardial infarction treated with primary percutaneous coronary intervention
Key words: mortality, smoking, ST-segment elevation myocardial infarction, tobacco



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Impact of smoking on outcomes in patients with ST-segment elevation myocardial infarction treated with primary percutaneous coronary intervention
Introduction: Smoking is a well‑established risk factor for cardiovascular diseases. However, in patients with ST‑segment elevation myocardial infarction (STEMI), smoking has been associated with better clinical outcomes; this phenomenon became known as the “smoker’s paradox.”
Objectives: The aim of this study was to evaluate the association between smoking and clinical outcomes in STEMI patients treated with primary percutaneous coronary intervention (PCI), using 3 large national registries.
Patients and methods: We retrospectively analyzed the data of 82 235 hospitalized STEMI patients treated with primary PCI. Among the analyzed population, 30 966 patients (37.96%) were smokers, and 51 269 (62.36%) were nonsmokers. We evaluated the baseline characteristics, pharmacotherapy, clinical outcomes, and readmission causes in a 36‑month follow‑up.
Results: The smokers were significantly younger (median [interquartile range] age, 58 [52–64] vs 68 [59–77] years; P <0.001) than the nonsmokers, and there were more men in this group. The patients who smoked were less likely to have traditional risk factors, as compared with the nonsmokers. In the unadjusted analysis, in‑hospital and 36‑month mortality and rehospitalization rates were lower in the smokers group. However, after adjustment for baseline characteristics that differed between the 2 groups, the multivariable analysis showed that tobacco use was one of the independent risk factors for 36‑month mortality (hazard ratio, 1.11; 95% CI, 1.06–1.18; P <0.001).
Conclusions: In the present large‑scale, registry‑based analysis, the observed lower 36‑month crude rates of adverse events among the smokers, as compared with the nonsmokers, might be partially explained by a significantly lower burden of traditional risk factors and younger age of the smokers. After accounting for age and other baseline differences, smoking was found to be one of the independent risk factors for 36‑month mortality.
What's new?
This is one of the largest studies examining the impact of smoking on outcomes in patients with ST‑segment elevation myocardial infarction (STEMI) treated with primary percutaneous coronary intervention. It adds greatly to a growing body of evidence refuting the existence of the “smoker’s paradox,” encompassing the complexity of the phenomenon. Our study showed that despite the observed lower 36‑month crude rates of adverse events among the smokers, after adjusting for baseline characteristic variables, tobacco use was found to be one of the independent risk factors for 36‑month mortality. The results of this study undermine the myth of beneficial effects of smoking on the prognosis in STEMI patients, and hopefully will contribute to tackling one of the biggest public health threats, that is, widespread tobacco use.
Introduction
The causality between smoking and cardiovascular disease (CVD) prevalence is considered to be unquestionable. Tobacco use is known to be the leading modifiable risk factor in patients with coronary artery disease (CAD).1,2 However, a favorable short‑term prognosis in smokers, as compared with nonsmokers, after ST‑segment elevation myocardial infarction (STEMI) has been described in multiple studies.3-6 This unanticipated phenomenon, known as the “smoker’s paradox,” has been attracting considerable interest due to its baffling nature ever since it has emerged into scientific discourse. Yet, there is still not enough literature comprehensively investigating the topic. The origin of this controversial and paradoxical association is still poorly understood. Numerous studies have attributed improved prognosis of smokers to their relatively younger age and, consequently, low‑risk baseline characteristics.7,8 Nevertheless, several papers reported a favorable prognosis in smokers even after adjustment for other comorbidities.3,9,10 Thus, it has been suggested that the underlying pathogenesis of STEMI in tobacco users differs from that observed in nonsmokers. It is hypothesized that smoking does not affect atherogenesis and plaque vulnerability as much as it promotes the imbalance in procoagulant vs anticoagulant activity.3,11,12 The conflicting evidence, counterintuitive results, as well as the scarcity of data makes further investigation necessary.
We therefore sought to evaluate the association between smoking and clinical outcomes in STEMI patients treated with primary percutaneous coronary intervention (PCI), using large national registries.
Patients and methods
Data sources
This is a retrospective analysis of data derived from 3 large registries: the Polish Registry of Acute Coronary Syndromes (PL‑ACS), the Polish Nationwide Acute Myocardial Infarction Database (AMI‑PL), and the Silesian Cardiovascular (SILCARD) registry. PL‑ACS is a nationwide, multicenter, prospective, ongoing registry that, since 2003, has been collecting detailed data on acute coronary syndromes (ACSs), including patient characteristics, treatment modalities, and outcomes. The registry is managed in cooperation with the Ministry of Health and the National Health Fund. A detailed design of PL‑ACS has been presented previously.13 In essence, this analysis was performed in consecutive STEMI patients incorporated into the registry between the years 2006 and 2017, from 414 hospitals. Data on postdischarge mortality were obtained from the National Health Fund, which is the obligatory public health insurer in Poland and the sole payer. The AMI‑PL is a registry that contains administrative data on all cases of AMI between 2009 and 2014, including data on long‑term outcomes of all patients admitted to hospitals with AMI (codes I21–I22 according to the International Classification of Diseases and Related Health Problems, 10th Revision [ICD‑10]). The design of AMI‑PL has been described elsewhere.14 In brief, the registry incorporates the data of all AMI cases gathered by the national health care provider. Thus, it accumulates the records on medical procedures as well as the morbidity rates. The SILCARD database was created jointly by the Silesian Center for Heart Diseases in Zabrze and the Regional Department of National Health Fund in Katowice in order to carry out a comprehensive analysis of patients with CVDs in the Silesia Province. General information on the SILCARD database has been published earlier.15 Briefly, the database contains records from all hospitals (n = 310) in the Silesia Province, a large administrative region in Southern Poland with a population of 3.7 million adults. The Silesia Province hosts a well‑structured hospital network, including 2 tertiary cardiology centers, 3 cardiac surgery departments, and over 20 cardiac catheterization laboratories. The National Health Fund contributed all data to the registry, covering the period between 2006 and 2016. The SILCARD database enlists consecutive adult patients from the Silesia province hospitalized in the cardiology, cardiac surgery, vascular surgery, or diabetology units for any reason, or those hospitalized in the internal medicine or intensive care units with the primary diagnosis of CVD. CVD was defined as code R52 or J96, or any I code according to the ICD‑10. The consent of an ethics committee for this analysis was not required. Secondary end points were defined based on readmission causes according to the ICD‑10 codes reported to National Health Fund (Table 1.)
Disease | Code |
Abbreviations: CAD, coronary artery disease; HF, heart failure | |
CAD | I20, I21, I25 |
HF and cardiomyopathies | I42, I43, I50 |
Arrythmias | I44, I45, I47, I48, I49 |
Cerebrovascular disease | I60, I61, I62, I63, I64, I65, I66, I67, I68, I69 |
Hypertension | I10, I11, I12, I13, I14, I15 |
Valvular disease and infective endocarditis | I05, I06, I07, I08, I09, I35, I36, I37, I38, I39 |
Diseases of arteries, arterioles, and capillaries | I70, I71, I72, I73, I74, I75, I76, I77,I78, I79 |
Other | I26, I27, I28, I30, I31, I32, I40, I41, I51, I52, I80, I81, I82, I83, I84, I5, I86, I87, I88, I89, I90, I91, I92, I93, I94, I95, I96, I97, I98, I99 |
Study population
We retrospectively analyzed the data of 259 748 patients with AMI from the PL‑ACS, AMI‑PL, and SILCARD databases. This analysis included all patients hospitalized with a principal diagnosis of STEMI (according to the current guidelines of the European Society of Cardiology [ESC]) treated with primary PCI. Data of all individual patients and all hospitalizations were analyzed. The outcomes during a 36‑month follow‑up were available for all included patients.
We included only the individuals who underwent primary PCI. The patients who were younger than 18 years at the time of hospitalization were excluded from the analysis. The included patients were stratified into 2 groups based on their smoking status. We evaluated the baseline characteristics, pharmacotherapy, outcomes, that is, the incidence of MI, stroke, and mortality at 12 and 36 months, as well as readmission causes over the 36‑month follow‑up.
We defined the smokers as individuals who answered affirmatively to the question “Do you smoke cigarettes?”, thus reporting current tobacco smoking. The study flowchart is presented in Figure 1.
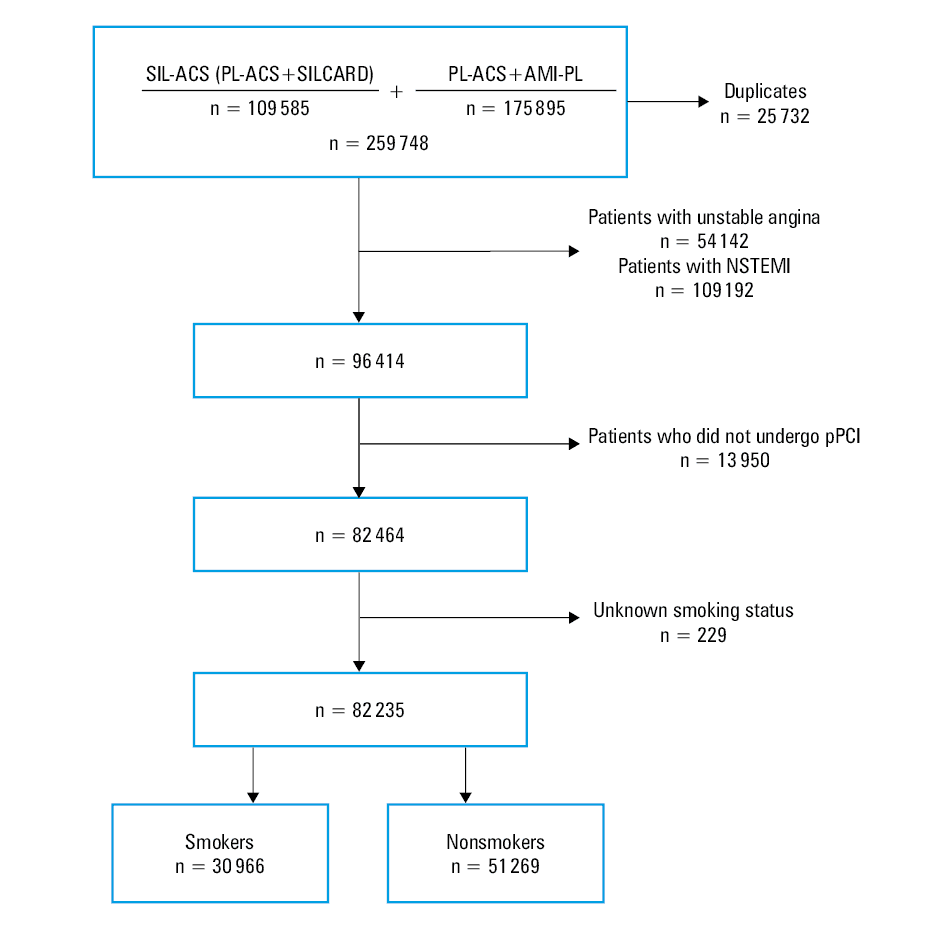
Abbreviations: AMI‑PL, Polish Nationwide Acute Myocardial Infarction Database; NSTEMI, non–ST‑segment elevation myocardial infarction; PL‑ACS, Polish Registry of Acute Coronary Syndromes; pPCI, primary percutaneous coronary intervention; SILCARD, Silesian Cardiovascular Registry
Statistical analysis
Qualitative variables were presented as percentages, and the comparative analysis was carried out using the χ2 test. The normality of distribution of the continuous variables was verified by visual inspection and the Shapiro–Wilk test, and these variables were reported as median with interquartile range (IQR) or mean with SD, and compared using the Mann–Whitney test or the t test, as appropriate. The long‑term outcomes and repeated hospitalizations over the 36‑month follow‑up were analyzed according to the first event of the given patient using the Kaplan–Meier method and compared by the log‑rank test. In order to adjust the 36‑month mortality for the differences in baseline characteristics, the Cox proportional hazards model was used. The baseline characteristics that differed between the groups with a P value below 0.05 were included in the multivariate analysis, and the final model was created by stepwise elimination (P <0.05 to remain in the model). The results were presented as hazard ratios (HRs) with 95% CIs. Statistica (version 13.1, TIBCO Software Inc., Palo Alto, California, United States) was used for calculations. The Kaplan–Meier curves were created using GraphPad Prism (version 9.4.0 for Windows, GraphPad Software, San Diego, California, United States). A 2‑tailed P value below 0.05 was considered significant.
Results
Baseline characteristics
We retrospectively analyzed the data of 82 235 patients hospitalized for STEMI (diagnosed according to the current ESC guidelines) and treated with primary PCI. Among the analyzed population, 30 966 patients (37.96%) were smokers and 51 269 individuals (62.36%) were nonsmokers. The patients in the smokers group were significantly younger (median [IQR] age, 58 [52–64] vs 68 [59–77] years; P <0.001) and more frequently male (76.94% vs 61.04%, respectively; P <0.001) than the nonsmoking patients. Angina was the most common presentation of STEMI in both groups. Type 2 diabetes prior to hospital admission was less prevalent in the smokers than in the nonsmokers (26.44% vs 39.52%; P <0.001). Hypercholesterolemia was also less frequent among the smokers (59.2% vs 60.16%; P <0.001). The median (IQR) left ventricular ejection fraction was 49% (40%–55%) in the patients who smoked and 46% (40%–53%) in those who did not (P <0.001). The smokers were less likely to be diagnosed with chronic kidney disease prior to admission than the nonsmokers (1.73% vs 5.55%, respectively; P <0.001). Sudden cardiac arrest as the initial manifestation of ACS was less prevalent in the smokers (1.93% vs 2.42%; P <0.001). Previous MI was also less frequent among the smokers (9.42% vs 13.15%; P <0.001). The smoking patients less frequently presented with heart failure (HF) (3.34% vs 6.25%; P<0.001), and were more likely than the nonsmokers to be classified as New York Heart Association class III or IV on admission. Sinus rhythm on admission was present in 95.49% of the smokers vs 91.77% of the nonsmokers (P <0.001). The baseline characteristics of the study population are summarized in Table 2.
Variable | Smokers (n = 30 966) | Nonsmokers (n = 51 269) | P value | |||
Abbreviations: CABG, coronary artery bypass grafting; Cx, circumflex artery; DBP, diastolic blood pressure; ECG, electrocardiography; HR, heart rate; IQR, interquartile range; LAD, left anterior descending artery; LM, left main coronary artery; LVEF, left ventricular ejection fraction; MI, myocardial infarction; NYHA, New York Heart Association; PAD, peripheral artery disease; PCI, percutaneous coronary intervention; RCA, right coronary artery; SBP, systolic blood pressure; TIMI, Thrombolysis in Myocardial Infarction; others, see Table 1 | ||||||
Age, y, median (IQR) | 58 (52–64) | 68 (59–77) | <0.001 | |||
Male sex, % | 79.64 | 61.04 | <0.001 | |||
Type 2 diabetes, % | 26.44 | 39.52 | <0.001 | |||
Obesity, % | 17.77 | 20.89 | <0.001 | |||
Hypertension, % | 58.27 | 71.78 | <0.001 | |||
Hypercholesterolemia, % | 59.2 | 60.16 | 0.01 | |||
Chronic kidney disease, % | 1.73 | 5.55 | <0.001 | |||
Chronic obstructive pulmonary disease, % | 3.13 | 2.92 | 0.09 | |||
Previous CAD, % | 6.53 | 11.35 | <0.001 | |||
PAD, % | 3.83 | 3.46 | 0.01 | |||
Previous MI, % | 9.42 | 13.15 | <0.001 | |||
Previous PCI, % | 6.61 | 9.4 | <0.001 | |||
Previous CABG, % | 1.02 | 1.95 | <0.001 | |||
Previous stroke, % | 1.9 | 3.88 | <0.001 | |||
Dominant symptom | Angina, % | 95.04 | 93.08 | <0.001 | ||
Dyspnea, % | 1.14 | 1.72 | ||||
Syncope, % | 0.47 | 0.79 | ||||
Cardiac arrest, % | 1.93 | 2.42 | ||||
Parameters on admission | ||||||
SBP, mm Hg, mean (SD) | 124.4 (32.7) | 126 (33.6) | <0.001 | |||
DBP, mm Hg, mean (SD) | 88.2 (25.6) | 86.3 (25.9) | <0.001 | |||
HR, bpm, median (IQR) | 75 (66–88) | 76 (68–90) | <0.001 | |||
LVEF, %, median (IQR) | 49 (40–55) | 46 (40–53) | <0.001 | |||
Pulmonary edema, % | 3.94 | 5.77 | <0.001 | |||
Cardiogenic shock, % | 1.37 | 2.25 | <0.001 | |||
HF, % | 3.34 | 6.25 | <0.001 | |||
NYHA class, % | I | 66.59 | 56.25 | <0.001 | ||
II | 27.88 | 32.37 | ||||
III | 2.68 | 5.06 | ||||
IV | 2.85 | 6.31 | ||||
Rhythm on ECG on admission, % | Sinus rhythm | 95.49 | 91.77 | <0.001 | ||
Atrial fibrillation | 2.6 | 6.09 | ||||
Pacemaker rhythm | 0.09 | 0.35 | ||||
Other than sinus rhythm | 1.82 | 1.79 | ||||
Infarct‑related artery, % | LM | 1.07 | 1.37 | <0.001 | ||
LAD | 39.09 | 42.84 | ||||
Cx | 14.39 | 13.7 | ||||
RCA | 39.98 | 44.1 | ||||
Bypass | 0.74 | 1.26 | ||||
Undefined | 1.05 | 1.36 | ||||
Symptom‑to‑balloon, min, median (IQR) | 260 (155–560) | 294 (167–670) | <0.001 | |||
Baseline TIMI score, % | 0 | 54.26 | 54.78 | <0.001 | ||
1 | 12.15 | 13.65 | ||||
2 | 11.58 | 12.1 | ||||
3 | 22 | 19.47 | ||||
Final TIMI score, % | 0 | 10.92 | 10.21 | <0.001 | ||
1 | 3.34 | 3.76 | ||||
2 | 5.1 | 6.58 | ||||
3 | 80.64 | 79.44 | ||||
Medications at discharge
Aspirin and P2Y12 inhibitors were prescribed more frequently in the smokers than in the patients who did not smoke (93.3% vs 89.11%; P <0.001 and 87.25% vs 84.08%; P<0.001, respectively). The smokers received angiotensin‑converting enzyme inhibitors and β-blockers at discharge more often (79.19% vs 76.39%; P <0.001 and 83.71% vs 80.83; P <0.001, respectively), they were also more commonly prescribed with statins (89.46% vs 85.62%; P <0.001). In total, 1.13% of the smokers and 1.86% of the nonsmokers received oral anticoagulants (P <0.001). The summary of medications prescribed at discharge is presented in Table 3.
Variable | Smokers (n = 30 966) | Nonsmokers (n = 51 269) | P value |
Data are presented as percentages.
Abbreviations: ACE, angiotensin‑converting enzyme; LWMH, low‑molecular‑weight heparin | |||
Aspirin | 93.3 | 89.11 | <0.001 |
P2Y12 inhibitors | 87.25 | 84.08 | <0.001 |
ACE inhibitors | 79.19 | 76.39 | <0.001 |
β-Blockers | 83.71 | 80.83 | <0.001 |
Statins | 89.46 | 85.62 | <0.001 |
Nitrates | 10.97 | 11.01 | 0.86 |
LMWH | 3.35 | 3.74 | 0.004 |
Oral anticoagulants | 1.13 | 1.86 | <0.001 |
Clinical outcomes
In‑hospital mortality was lower in the smokers group than in the nonsmoking patients (2.59% vs 6.17%; P <0.001). Also, the rates of in‑hospital MI and stroke were significantly lower in the smokers group. Similarly, cardiogenic shock and pulmonary edema developed less frequently in the smokers, as compared with the nonsmokers (1.78% vs 3.17%; P <0.001 and 0.85% vs 1.34%; P <0.001). The incidence of in‑hospital cardiac arrest was lower in the smoking patients (2.98% vs 4.82%; P <0.001).
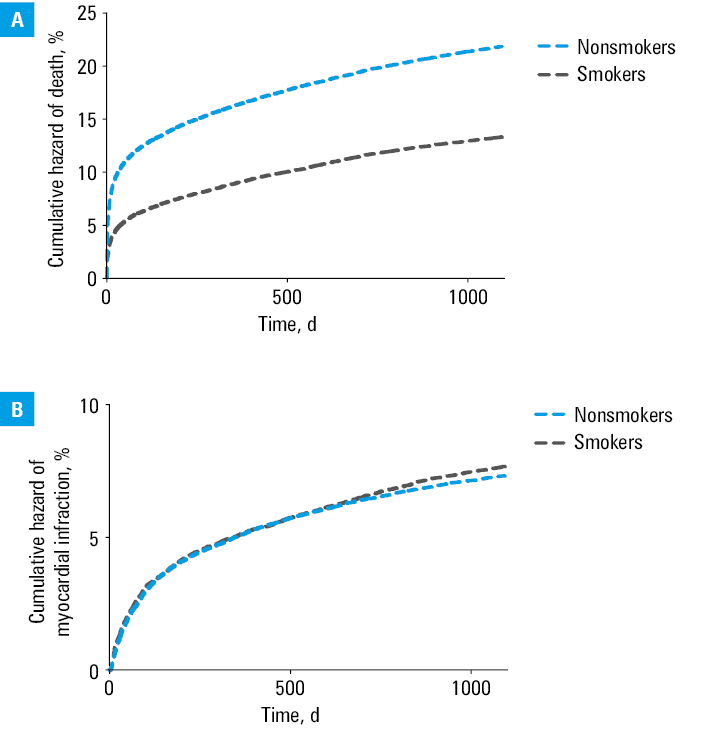
All‑cause mortality both at 12 and at 36 months was lower in the smokers group (7.91% vs 14.8%; P <0.001 and 13.25% vs 21.84%; P <0.001, respectively) (Figure 2A). There was no difference between the analyzed groups in MI rates at either time point (12 months, 5.15% vs 5.09%; P = 0.72; 36 months, 7.71% vs 7.36%; P = 0.07, in smokers vs nonsmokers, respectively). Revascularization rates were higher in the smokers group at both time points (12 months, 21.79% vs 21.11%; P = 0.03; 36 months, 25.08% vs 23.83%; P <0.001). Also, the stroke incidence was lower in the smokers group both at 12 and at 36 months (0.63% vs 1.25%; P <0.001 and 1.35% vs 2.33%, P <0.001, respectively). Patient outcomes are presented in Table 4. The Kaplan–Meier curves of cumulative incidence rates of death and MI in both analyzed groups are presented in Figure 2.
Outcome | Smokers (n = 30 966) | Nonsmokers (n = 51 269) | P value |
Data are presented as number (perentage) of patients.
a Data available for 25 993 smokers and 44 365 nonsmokers
Abbreviations: CRT‑D, cardiac resynchronization therapy–defibrillator; ICD, implantable cardioverter–defibrillator; others, see Table 2 | |||
In‑hospital | |||
Death | 802 (2.59) | 3163 (6.17) | <0.001 |
Cardiac arrest | 923 (2.98) | 2471 (4.82) | <0.001 |
Cardiogenic shock | 551 (1.78) | 1625 (3.17) | <0.001 |
MI | 118 (0.38) | 256 (0.5) | 0.01 |
Stroke | 59 (0.19) | 179 (0.35) | <0.001 |
Pulmonary edema | 263 (0.85) | 687 (1.34) | <0.001 |
At 12 months | |||
Death | 2449 (7.91) | 7588 (14.8) | <0.001 |
MI | 1595 (5.15) | 2610 (5.09) | 0.72 |
Stroke | 195 (0.63) | 641 (1.25) | <0.001 |
Coronary angiography | 8599 (27.77) | 13 474 (26.28) | <0.001 |
PCI | 6748 (21.79) | 10 823 (21.11) | 0.03 |
CABG | 1267 (4.09) | 2051 (4) | 0.56 |
Cardiac ablation | 31 (0.1) | 41 (0.08) | 0.39 |
ICD/CRT‑D implantation | 486 (1.57) | 697 (1.36) | 0.03 |
At 36 monthsa | |||
Death | 3444 (13.25) | 9689 (21.84) | <0.001 |
Myocardial infarction | 2004 (7.71) | 3265 (7.36) | 0.07 |
Stroke | 351 (1.35) | 1034 (2.33) | <0.001 |
Coronary angiography | 8528 (32.81) | 13 487 (30.4) | <0.001 |
PCI | 6519 (25.08) | 10 572 (23.83) | 0.001 |
CABG | 1178 (4.53) | 1992 (4.49) | 0.8 |
Cardiac ablation | 39 (0.15) | 58 (0.13) | 0.46 |
ICD/CRT‑D implantation | 608 (2.34) | 905 (2.04) | 0.01 |
After correcting for the differences in baseline characteristics between the 2 groups, multivariable analysis demonstrated that tobacco use was one of the independent risk factors for 36‑month mortality (HR, 1.11; 95% CI, 1.06–1.18; P <0.001). The results of the multivariable analysis are summarized in Table 5.
Variable | HR | 95% CI | P value |
Abbreviations: IRA, infarct‑related artery; others, see Table 2 | |||
Age (per 1‑year increase) | 1.05 | 1.05–1.05 | <0.001 |
Male sex | 1.04 | 0.99–1.09 | 0.1 |
Type 2 diabetes | 1.25 | 1.2–1.32 | <0.001 |
Smoking | 1.11 | 1.06–1.18 | <0.001 |
IRA–LAD | 0.96 | 0.92–1.01 | 0.1 |
LVEF (per 1% increase) | 0.95 | 0.95–0.95 | <0.001 |
Angina symptoms | 0.6 | 0.56–0.64 | <0.001 |
Sinus rhythm on ECG | 0.77 | 0.73–0.82 | <0.001 |
Cardiogenic shock | 2.3 | 2.12–2.47 | <0.001 |
PAD | 1.63 | 1.5–1.78 | <0.001 |
Hospitalization due to cardiac arrest | 4.48 | 4.16–4.81 | <0.001 |
Time‑to‑balloon (per 10‑min increase) | 1.014 | 1.001–1.027 | 0.03 |
All‑cause readmission rates were also lower in the smokers than in the nonsmokers, both at 12 and at 36 months (12 months, 50.16% vs 52.21%; P <0.001; 36 months, 62.65% vs 64.09%; P <0.001, in smokers vs nonsmokers, respectively). The incidence of HF and cardiomyopathy was higher in the nonsmokers at both studied time points (12 months, 6.97% vs 11.04%; P <0.001; 36 months, 7.38% vs 11.48%; P <0.001, in smokers vs nonsmokers, respectively). Chronic coronary syndrome was the most common cause for cardiovascular readmission in both groups at both time points. All readmission causes are presented in Table 6.
Variable | Smokers (n = 30 966) | Nonsmokers (n = 51 269) | P value |
Data are presented as percentages.
a Aortic aneurysm and dissection, other aneurysms and dissections, other peripheral vascular diseases, arterial embolism and thrombosis, other disorders of arteries and arterioles, diseases of capillaries
Abbreviations: see Table 1 | |||
Readmission at 12 months | |||
All‑cause readmission | 50.16 | 52.21 | <0.001 |
Cardiovascular readmission | 41.86 | 43.26 | <0.001 |
CAD | 82.02 | 74.67 | <0.001 |
HF and cardiomyopathies | 6.97 | 11.04 | <0.001 |
Arrythmias | 2.73 | 3.73 | <0.001 |
Cerebrovascular disease | 1.8 | 2.83 | <0.001 |
Hypertension | 1.68 | 2.26 | 0.001 |
Valvular disease and infective endocarditis | 0.4 | 0.72 | <0.001 |
Diseases of arteries, arterioles, and capillaries | 2.04 | 1.91 | 0.42 |
Other reasons | 2.36 | 2.84 | 0.01 |
Readmission at 36 months | |||
All‑cause readmission | 62.65 | 64.09 | <0.001 |
Cardiovascular readmission | 49.17 | 47.87 | <0.001 |
CAD | 79.15 | 71.51 | <0.001 |
HF and cardiomyopathies | 7.38 | 11.48 | <0.001 |
Arrythmias | 3.1 | 4.17 | <0.001 |
Cerebrovascular disease | 2.4 | 3.67 | <0.001 |
Hypertension | 2.06 | 2.68 | <0.001 |
Valvular disease and infective endocarditis | 0.46 | 0.76 | <0.001 |
Diseases of arteries, arterioles, and capillariesa | 2.74 | 2.37 | 0.02 |
Other reasons | 2.72 | 3.35 | <0.001 |
Discussion
In the present large‑scale, retrospective analysis of data derived from 3 extensive registries, we evaluated the impact of smoking on the outcomes of STEMI patients treated with primary PCI. The key finding was that despite relatively better outcomes at 36 months in the smokers group, after adjusting for baseline characteristic, smoking was found to be one of the independent risk factors for 36‑month mortality. Also, among the patients with STEMI, those who smoked were prone to develop MI earlier in life than those who refrained from smoking.
The smoker’s paradox is still considered a conundrum due to decades of conflicting research results. In our study, the smokers were significantly younger, and had a lower cardiovascular risk burden as well as a lower incidence of comorbidities on admission. These findings are in line with the results of numerous previously published papers. Differences in baseline characteristics between the smokers and the nonsmokers, along with confounding by other factors have been considered to account for the phenomenon.16,17 However, some researchers used multivariable analyses to investigate weather the survival benefit associated with smoking in STEMI patients really exists.8,18,19
As stated before, there are several plausible explanations of the smoker’s paradox, with residual confounding or systematic errors being only some of them. According to some hypotheses, there might be a more complex explanation than just the statistical bias. Different pathogenesis of STEMI in smokers and nonsmokers has been taken into consideration. Enhanced platelet response to clopidogrel therapy in smokers, as compared with nonsmoking patients, caused by cytochrome P450 activation could also be responsible for the phenomenon.20,21
It has been deliberated whether ischemic preconditioning, which would decrease the size of the infarct, or a decreased inflammatory response in smokers might be the cause of this paradoxical association.22-24 Also, the state of hypercoagulability related to tobacco use and a subsequent coagulation–fibrinolysis imbalance may influence the outcome.25-27 Adverse events during the initial hospitalization occurred predominantly more frequently in the nonsmoking patients. In‑hospital mortality, as well as the incidence of in‑hospital cardiac arrest, were lower in the smokers group. Cardiogenic shock and pulmonary edema also developed less frequently in tobacco smokers.
Our results tie well with previous studies, wherein smoking was associated with a relatively better prognosis after primary PCI in STEMI. Although the smokers had a better prognosis in the unadjusted analysis, after correction for differences in age and presenting characteristics, they often had an increased risk of reinfarction and the composite of death or HF hospitalization during the 12‑month follow‑up. They were also prone to develop post‑PCI major adverse cardiovascular events (MACEs) earlier than the nonsmokers.17,28
In our study, all‑cause mortality and readmission rates both at 12 and 36 months were lower in the smokers group. However, after adjustment for baseline covariates, smoking was found to be one of the independent risk factors for 36‑month mortality in the multivariable analysis, despite the counterintuitive results of some previous studies. The advantages of the presented analysis are the relatively long follow‑up of 36 months and the accurate assessment of readmission rates and their causes.
Younger age is a factor that independently improves the overall prognosis and is a predictor of lower long- and short‑term mortality.29-33 In our study, the patients from the smokers group were on average 10 years younger than the nonsmokers. This fact is crucial for correct interpretation of the study results. Moreover, a history of MI is considered to be a well‑recognized risk factor for long‑term mortality among patients with ACS.34,35 In our population, the smokers had previous MI significantly less frequently than the nonsmokers (9.42% vs 13.15%; P <0.001). Patients with diabetes mellitus (DM) who present with STEMI, as compared with nondiabetic individuals, are also at an increased risk for adverse events, including HF, arrhythmia, bleeding, and death. Mostly due to an elevated risk for atherosclerosis in DM, the disease is also associated with higher short- and long‑term morbidity and mortality.36,37 In our study, the incidence of DM in the smokers was lower than in the nonsmoking group, which could also influence the overall results.
Tobacco consumption remains the leading cause of preventable death; nonetheless, it has been estimated that approximately 22.5% of adults smoke tobacco products worldwide.38 The intention behind our research was to elucidate the origin of the paradoxical association known as the smoker’s paradox, as well as to encompass the complexity of the phenomenon, especially because claims that smoking has a protective role against CVD can be pernicious to public health. It is therefore essential to unequivocally establish that tobacco smoking is not the variable that improves the outcome in STEMI patients. What is more, it predisposes to experiencing MI at a younger age. Promoting smoking cessation through population‑wide campaigns is the right approach to tackle the issue and reduce the smoking rates, along with morbidity and mortality that follow tobacco use.39,40
Limitations
The findings of this study have to be interpreted in light of some limitations. Firstly, the observational nature of this analysis is a restriction that arises from the study design. Furthermore, the follow‑up data were obtained from the National Health Fund; thus, we had no insight into the specific causes of death in the analyzed population. What is more, the smokers with STEMI might have had higher mortality rates prior to presentation to the hospital.41 Additionally, due to secondhand smoking and ambient air pollution, it is unfeasible to truly distinguish between smokers and nonsmokers. Finally, the smokers were treated as a homogenous group, whereas the tobacco consumption patterns surely differed among them, which also may have influenced the outcomes. Descriptive data on tobacco use were not available.
Conclusions
In the present large‑scale, registry‑based analysis, the observed lower 36‑month crude rates of adverse events among the smokers, as compared with the nonsmokers, might be partially explained mainly by younger age of the smokers. After accounting for age and other baseline differences (including known risk factors), smoking was found to be one of the independent risk factors for 36‑month mortality. This finding, as well as the observation that smokers tend to suffer from STEMI on average 10 years earlier in life than the nonsmokers, undermine the theory proposing salutary effects of smoking on atherosclerosis development and progression. To the best of our knowledge, this is the largest study examining the impact of smoking on outcomes in patients with STEMI treated with primary PCI in a European population.
- Gleerup HB, Dahm CC, Thim T, et al. Smoking is the dominating modifiable risk factor in younger patients with STEMI. Eur Heart J Acute Cardiovasc Care. 2020; 9: 70‑75. | Crossref
- Salehi N, Janjani P, Tadbiri H, et al. Effect of cigarette smoking on coronary arteries and pattern and severity of coronary artery disease: a review. J Int Med Res. 2021; 49: 1‑11. | Crossref
- Gupta T, Kolte D, Khera S, et al. Smoker’s paradox in patients with ST‑segment elevation myocardial infarction undergoing primary percutaneous coronary intervention. J Am Heart Assoc. 2016; 5: e003370. | Crossref
- Barbash GI, Reiner J, White HD, et al. Evaluation of paradoxic beneficial effects of smoking in patients receiving thrombolytic therapy for acute myocardial infarction: mechanism of the “smoker’s paradox” from the GUSTO‑I trial, with angiographic insights. Global Utilization of Streptokinase and Tissue‑Plasminogen Activator for Occluded Coronary Arteries. J Am Coll Cardiol. 1995; 26: 1222‑1229. | Crossref
- Barbash GI, White HD, Modan M, et al. Significance of smoking in patients receiving thrombolytic therapy for acute myocardial infarction. Experience gleaned from the International Tissue Plasminogen Activator / Streptokinase Mortality Trial. Circulation. 1993; 87: 53‑58. | Crossref
ARTICLE INFORMATION