Polypill in cardiovascular disease prevention: recent advances
Key words: polypill, primary cardiovascular prevention, secondary cardiovascular prevention, treatment adherence, treatment persistence



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Polypill in cardiovascular disease prevention: recent advances
Triple therapy with lipid‑lowering, antihypertensive, and antiplatelet agents reduces the risk of recurrent cardiovascular fatal and nonfatal events, cardiovascular mortality, and total mortality in secondary prevention. In real life, however, effective implementation of these optimal treatments both in primary and secondary prevention is low, and thus their contribution to cardiovascular prevention is much lower than it could be, based on research data. One of the main barriers to the adequate implementation of these strategies is low adherence to the elevated number of pills, as adherence is adversely affected by the complexity of the prescribed treatment regimen, and can be considerably improved by treatment simplification. This review updates the findings provided by recent epidemiological and clinical studies favoring a polypill‑based approach to cardiovascular prevention. The increased prevalence of patients with multiple cardiovascular risk factors and comorbidities provides the rationale for a therapeutic strategy based on a combination of drugs against different risk factors in a single pill. Pharmacologic studies have demonstrated that different cardiovascular drugs can be combined in a single pill with no loss of their individual efficacy, and this favors adherence to and persistence of treatment, as well as multiple risk factor control. Recently, a randomized clinical trial SECURE (Secondary Prevention of Cardiovascular Disease in the Elderly) has shown a significant, 30% reduction in cardiovascular events, and a 33% reduction in cardiovascular death in patients after myocardial infarction treated with a polypill, as compared with usual care, thus supporting the polypill use as an integral part of any cardiovascular prevention strategy.
Introduction
The concept of a cardiovascular polypill was originally proposed in 2001 by the World Health Organization and Welcome Trust expert group,1 suggesting that a one‑pill combination of 4 drugs, each with a documented ability to prevent cardiovascular disease (CVD) (a β-blocker, an angiotensin‑converting enzyme inhibitor [ACEI], a statin, and aspirin) might reduce the risk of future events in patients with previous CVD. Two years later, Wald and Law2 suggested that a polypill containing 6 agents with proven or potential cardiovascular prevention ability (3 antihypertensive drugs, a statin, aspirin, and folic acid) would reduce the incidence of cardiovascular events by over 80% in individuals over 55 years old, and that its wide implementation would be followed by an unthinkable and unprecedented improvement of both primary and secondary CVD prevention. Nevertheless, the scientific community did not accept this strategy of “vaccination approach” and discarded it as unproven and unrealistic. The main concerns included the unknown consequences of medicating the entire population, negative psychological effects of lifelong treatment in healthy individuals, inconvenience, and costs of possible adverse reactions to a high number of drugs, together with the risk of favoring unhealthy lifestyle habits resulting from the belief of being protected by the drugs taken.
However, based on the initial hypothesis of Wald and Law, many scientists proposed a more selective use of the polypill in individuals without CVD and high cardiovascular risk as a primary prevention strategy.3 Although lacking a definitive proof of efficacy, safety, and cost‑effectiveness of this strategy in all participants, several pilot studies4-6 demonstrated its feasibility and efficacy in subgroups of patients with multiple cardiovascular risk factors and advanced atherosclerotic disease.7 Overall, studies have shown that the use of the polypill significantly increases adherence to treatment.8,9 None of the previous studies had the power to detect significant differences in the rate of new cardiovascular events, but recent results of a meta‑analysis by the Polypill Trialists’ Collaboration7 confirm that the polypill containing an antihypertensive drug, a statin, and aspirin may be effective in the primary prevention of cardiovascular events.
In the last years, a large body of evidence has indicated that the control of cardiovascular risk factors either in the general population or in the patients at high risk, such as those with coronary artery disease (CAD), is very low and that poor adherence to cardioprotective treatment may be one of the most important factors contributing to this problem.10-16 The EUROASPIRE surveys in the patients hospitalized for CAD in 24 European countries have consistently shown that the guideline‑recommended targets for blood pressure and low‑density lipoprotein cholesterol (LDL‑C) are critically low.10 This is associated with insufficient implementation of the optimal medical treatment in these patients, particularly the suboptimal use of high‑intensity statin therapy and a combination of antihypertensive drugs to achieve recommended targets. Results of the ISCHEMIA study in Poland clearly show that this challenge may be overcome by the use of contemporary treatment methods and multispecialty team efforts.11 In addition, several studies have shown that complex treatment strategies, particularly those based on a high number of daily pills, adversely affect adherence, which is substantially improved by treatment simplification.17-21 As treatment simplification is probably the most important feature of a polypill regimen, this strategy appears to be the most adequate to improve the reported low efficacy of primary and secondary cardiovascular prevention at the population level.22-26
This review will update the findings provided by recent epidemiologic and clinical studies favoring a polypill‑based approach to cardiovascular prevention, the most recent evidence that this approach is effective in reducing cardiovascular morbidity and mortality in both primary and secondary cardiovascular prevention, the advantages associated with combining several drugs in a single Tablet, and the challenges and opportunities for wide implementation of a polypill strategy for cardiovascular protection in both low‑income and developed countries.
Rationale for the use of a polypill in the era of personalized medicine
It may seem counterintuitive that in the era of personalized and precision medicine, a cardiovascular polypill would be considered one of the most scalable strategies to restrain atherosclerotic cardiovascular disease (ASCVD) pandemic.6,27 However, the growing number of cardiovascular risk factors, especially in low- and middle‑income countries (LMIC), where accessibility of preventive cardiovascular therapy is scarce, calls for scalable, simple, and cost‑effective strategies to ensure adequate therapeutic treatment to prevent first or recurrent cardiovascular events.28-30
CVDs are now the leading cause of death worldwide. In 2019, they were responsible for more than 19 million deaths worldwide and the death toll is expected to reach 25 million by 2030. Although it continues its decades‑long rise in almost all countries, the problem affects particularly LMIC. Alarmingly, in some high‑income countries where it was previously declining, the age‑standardized rate of CVD has begun to rise.31 The health‑related, social, and economic costs of this growth require simple solutions to overcome this grave problem, and there is an urgent need to focus on implementing the already existing cost‑effective policies and interventions. Not only a healthier lifestyle including healthy diet, increased physical activity, and smoking cessation must be recommended and implemented, but also additional strategies to prevent CVDs are urgently needed. Pharmacologic treatment of high blood pressure (BP) and LDL‑C levels to achieve strict targets have shown to significantly reduce the frequency of cardiovascular events and CVD‑related mortality even in individuals at a low risk and without clinical CVD. In high‑risk populations without established vascular disease and in those with established vascular disease, a combination of low doses of aspirin, antihypertensive, and lipid‑lowering drugs has reduced the frequency of cardiovascular events and CVD‑related mortality.32,33 Therefore, the cardiovascular polypill containing an antihypertensive drug, a statin, and aspirin represents one of the most promising strategies, which should be implemented as an integrated public health approach to promote healthy lifestyle, control cardiovascular risk factors, and effectively implement cardiovascular therapies in high‑risk patients.34
Advantages of the clinical use of a polypill in cardiovascular prevention: accessibility, adherence, risk factor control, cost‑effectiveness, and patient preference
The negative impact of low adherence to prescribed CVD drugs on primary and secondary prevention prompted investigators to evaluate new strategies that should include new interventions in routine clinical practice and encouraged governments to develop new health policies. One of these strategies is treatment simplification by reducing the number of pills. It can be assumed that any strategy aimed at simplifying the treatment, such as the polypill, shall result in improved adherence. The initial polypill trials were designed to investigate pharmacodynamics and safety of the polypill as phase 2 studies, although with not enough statistical power to detect differences in clinical outcomes.35 The rationale for designing phase 2 studies was largely based on the understanding that the components of the polypill have been previously widely accepted, and their use is approved for primary and secondary prevention of atherosclerosis.
A Cochrane systematic review36 from 2017 summarized the evidence on the use of the polypill and included 13 polypill trials (9059 participants) from 32 countries, published up to 2016, that investigated the effect of different drug combinations in comparison with usual care, placebo, or an active comparator. The most recent reports (until 2022) have included new retrospective observation studies on the beneficial effects of the polypill on cardiovascular risk factors and prevention of hard events,37 2 randomized clinical trials on primary and secondary prevention29,38 and their meta‑analysis,7 and a prospective randomized clinical trial comparing the effect of a polypill‑based strategy on cardiovascular events and mortality in comparison with the usual care.39
The barriers that need to be overcome to globally implement the polypill‑based strategies include confirmation of their superiority vs the standard treatment in several aspects, such as the drug accessibility, the adherence to and persistence of the treatment, better control of all major risk factors, cost‑effectiveness, and the patient preference.
As far as accessibility and affordability are concerned, nearly 80% of all deaths due to CVDs take place in LMIC, where the access to any medication is a serious problem. Results from the PURE studies40,41 show that only 8% to 14% of patients have access to antiplatelet drugs, statins, and antihypertensive medication in secondary prevention, which is even more evident in rural areas. The superior adherence to the polypill, as compared with the standard treatment, has been consistently reported in clinical trials in different populations, which has made the polypill the single most efficient strategy to significantly improve adherence. Four trials have shown the effect of polypills on adherence as being 44% higher than that of the comparator (P <0.001).9,42-44 It is important to note that participants with low baseline adherence were those showing the greatest improvement in adherence to polypills, as compared with the participants with high baseline adherence levels. This finding supports the recommendation that polypills may be used to reduce differences manifested as lower baseline medication adherence rates in low‑income populations.45
As far as the control of cardiovascular risk factors is concerned, 13 trials, with 7638 participants, reported the polypill effect on systolic BP (SBP), which was on average by 6.3 mm Hg lower in the polypill group than in the comparator group (P <0.001). A total of 11 trials, with 6565 participants, reported the effect of the polypill on total cholesterol, which was on average by 0.6 mmol/l lower in the polypill group (P <0.001).35 Due to the fact that most trials addressing changes in these cardiovascular risk factors had short‑term follow‑up, the differences in BP and cholesterol levels seen in the polypill and comparator groups were not maintained in the long‑term follow‑up to manifest differences in clinical events. A recent real‑life phase 4 study in 1193 patients in Mexico has shown a significant reduction of SBP from a mean baseline of 146.9 mm Hg to 128 mm Hg (P <0.001), and of diastolic BP (DBP) from 89.1 mm Hg to 80.4 mm Hg (P <0.001). LDL‑C levels were also significantly reduced from a mean baseline of 132.5 mg/dl to 107.6 mg/dl (P <0.001) after 1 year of treatment with the CNIC‑polypill.46
Although increasing the use of drugs results in a short‑term increase of costs, it then reduces the long‑term number of significant cardiovascular events, as well direct and indirect costs of hospitalization and treatment of the events. The net result is a reduction in health care costs in the long‑term. A systematic review47 found that when adherence is greater than 80%, the reduction in expenditure may be up to 18%. Several pharmacoeconomic models comparing the use of a polypill strategy with the usual care have been reported. Even in the least beneficial models, the polypill strategy has been shown to be cost‑effective due to its effects on the clinical outcomes resulting from improved adherence and control of the cardiovascular risk factors.48-50
Finally, various trials comparing different polypills with the usual care have reported on acceptability of the polypill concept by physicians and patients.45 Although subject to social desirability bias, whereby participants might report favorably to be seen in a better light, the overwhelming response was favorable toward the use of a polypill in routine clinical practice. Further studies surveyed the patients and physicians who were not involved in clinical trials with similar positive response to the polypill concept. The most commonly mentioned advantages were the ease and convenience of taking fewer pills, cost‑saving benefits, and improved safety due to simplified, and therefore less confusing pill regimens.51
What is new in primary prevention of cardiovascular disease
Although the beneficial effects of antihypertensive and lipid‑lowering drugs are well‑established,32,52 the use of low‑dose aspirin for primary prevention of CVD has been a matter of controversy.53 A recent systematic review and meta‑analysis54 of randomized clinical trials (RCTs) showed that the use of aspirin in patients without CVD was associated with a 38% risk reduction of cardiovascular events, and with a 0.47% higher risk of major bleedings.
This informed the European Society of Cardiology guidelines on diabetes, prediabetes, and CVD developed in collaboration with the European Association for the Study of Diabetes, which recommend the use of aspirin at low doses in diabetic patients even without prior CVD, thereby extending antiplatelet treatment to patients with a high cardiovascular risk also in primary prevention of CVD, if there are no contraindications.55 Similarly, the 2019 guidelines of the American College of Cardiology / American Heart Association on the primary prevention of CVD recommended using low‑dose aspirin for primary prevention of ASCVD in adults aged 40 to 70 years with high cardiovascular risk and no increased risk of bleeding. On the other hand, a therapy for patients older than 70 years, without increased bleeding risk must be individualized.56 Therefore, in individuals at high cardiovascular risk with no clinical evidence of a previous cardiovascular event and no significant risk of major bleeding, the polypill strategy including a low dose of aspirin can be considered.
The HOPE‑3 study57 explored the role of 3 drugs, renin‑angiotensin system (RAS) AT1 receptor blocker (ARB) candesartan, thiazide diuretic hydrochlorothiazide (HCTZ), and a 10‑mg dose of rosuvastatin into a single pill. The study recruited over 12 000 participants from many countries around the world, including men aged over 55 years and women over 65 years with at least 1 cardiovascular risk factor. The study had a 2 × 2 factorial design and the participants were randomly assigned to receive placebo or a low dose of a candesartan/HCTZ combination in the first arm. Then, in the second arm,58 they were randomly assigned to receive rosuvastatin 10 mg or placebo. The third arm compared the combination of the 2 antihypertensive drugs plus the statin with the double placebo.59 In the first arm, the patients who received only BP‑lowering treatment did not show a significant reduction in the composite primary outcome of cardiovascular death, nonfatal myocardial infarction (MI), or nonfatal stroke after a mean of 5.6 years vs placebo.57 In the second arm, the participants receiving only the statin showed a significantly (by 24%) lower risk of cardiovascular events than those receiving placebo.58 The third arm showed that the patients receiving the combination of the 2 antihypertensive drugs plus the statin had significantly (by 38%) lower rates of the primary outcome as compared with those taking placebo.59
A pragmatic cluster‑RCT conducted in Iran assessed the efficacy of a polypill with 4 components: aspirin, atorvastatin, HCTZ, and either enalapril or valsartan, vs minimal care consisting of a nonpharmacologic intervention in 6838 patients treated for primary or secondary CVD prevention. The primary outcome was the onset of major cardiovascular events (MACE) including hospitalization for acute coronary syndrome, fatal MI, sudden death, heart failure (HF), coronary artery revascularization procedures, and nonfatal and fatal stroke. After a 5‑year follow‑up, the 3421 individuals treated with the polypill had a lower risk of MACE than the 3417 patients offered minimal care, regardless of the history of CVD. The incidence of bleeding was similar in the 2 groups.38
Using a 2 × 2 × 2 factorial design, the recent International Polycap Study‑3 (TIPS‑3)29 evaluated the efficacy and safety of once‑daily polypill containing 40 mg of simvastatin, 100 mg of atenolol, 25 mg of HCTZ, and 10 mg of ramipril compared with matching placebo, and 75 mg of aspirin compared with matching placebo, and a combination of the polypill with aspirin compared with double placebo. The primary outcome was the incidence of MI, stroke, death from cardiovascular causes, resuscitated cardiac arrest, HF, or revascularization. A total of 5713 patients of a mean age of 64 years at intermediate or high cardiovascular risk, without CVD, were randomized and the mean follow‑up was 4.6 years. The primary outcome for the polypill comparison was the incidence of MACE plus HF, resuscitated cardiac arrest, and arterial revascularization, and it was present in 126 participants (4.4%) in the polypill group and in 157 individuals (5.5%) in the placebo group (hazard ratio [HR], 0.79; 95% CI, 0.63–1). The primary outcome for the polypill‑plus‑aspirin combination occurred in 59 participants (4.1%) in the combined‑treatment group and in 83 patients (5.8%) in the double placebo group (HR, 0.69; 95% CI, 0.5–0.97). A similar beneficial effect of the polypill strategy on death from cardiovascular causes, MI, or stroke occurred in 52 participants (3.6%) in the polypill‑plus‑aspirin group, and in 75 patients (5.3%) in the placebo group (HR, 0.68; 95% CI, 0.47–0.96).29
The reduction in SBP observed in the TIPS‑3 trial was larger than that observed in the PolyIran trial, in which no difference in DBP was detected at the study’s end.38 A combination treatment in the TIPS‑3 trial with a polypill containing a statin, 3 antihypertensive drugs, and aspirin lowered the incidence of cardiovascular events as compared with placebo in the participants without established CVD at intermediate or high cardiovascular risk.29
Finally, the individual participant data meta‑analysis7 of these 3 large RCTs (HOPE‑3, PolyIran, and TIPS‑3 trials), including 18 162 participants, compared the fixed‑dose combination treatment strategy including antihypertensive drugs plus statin, with or without aspirin, and a control strategy (placebo or usual care) in the primary prevention of CVD. The primary outcome was time to the first occurrence of a composite of cardiovascular death, MI, stroke, or arterial revascularization. During a median follow‑up of 5 years, the primary outcome occurred in 276 patients (3%) in the fixed‑dose combination strategy and 445 patients (4.9%) in the control group (HR, 0.62; 95% CI, 0.53–0.73; P <0.001). A significant reduction in the primary outcome and its components was observed for all fixed‑dose combination strategies, with and without aspirin, although strategies including aspirin showed greater reductions. The reductions were also observed for all separate components of the primary outcome, that is, MI (HR, 0.52; 95% CI, 0.38–0.7), revascularization (HR, 0.54; 95% CI, 0.36–0.8), stroke (HR, 0.59; 95% CI, 0.45–0.78), and cardiovascular death (HR, 0.65; 95% CI, 0.52–0.81). Therefore, the individualized results of these 3 trials and their meta‑analysis showed that the combination treatment strategies based on polypills containing low‑dose aspirin, antihypertensive drugs, and statin, substantially reduced MACE, MI, stroke, revascularization, and cardiovascular death in primary CVD prevention.7 These benefits were consistent irrespective of cardiometabolic risk factors, suggesting that the polypill strategy should be recommended to hypertensive patients with dyslipidemia in whom aspirin is indicated as a simplification strategy in primary prevention of CVD (Table 1).
Trial (sample size) | Population | Polypill composition | Outcomes |
Abbreviations: CVD, cardiovascular disease; HCTZ, hydrochlorothiazide; LDL‑C, low‑density lipoprotein cholesterol; MACE, major cardiovascular events | |||
Indian Polycap Study (TIPS)4 (n = 2053) | Men and women aged 40–80 y without CVD, with hypertension and high‑risk diabetes mellitus in India | Aspirin 100 mg, ramipril 5 mg, simvastatin 20 mg, HCTZ 12.5 mg, atenolol 50 mg | Feasibility, effect on risk factor levels, safety and tolerability |
Polypill for primary prevention of cardiovascular disease: a feasibility WHO study6 (n = 216) | Age >40 y without CVD and with estimated 10‑year total CVD risk score >20% in Sri Lanka | Aspirin 75 mg, simvastatin 10 mg, lisinopril 10 mg, HCTZ 12.5 mg (Red Heart Pill 2b) | Effect on estimated 10‑year total CVD risk score |
Improving Adherence using Combination Therapy (IMPACT)43 (n = 513) | Established CVD or 5‑year risk ≥15% | Aspirin 75 mg, simvastatin 40 mg, and lisinopril 10 mg with either atenolol 50 mg or HCTZ 12.5 mg | Effect on adherence and mean change in blood pressure and LDL‑C at 12 months |
Indian Polycap Trial (TIPS‑3)29 (n = 5713) | Primary prevention with estimated yearly CVD event rate >1% using the INTERHEART risk score in China and India | Simvastatin 40 mg, atenolol 100 mg, HCTZ 25 mg, and ramipril 10 mg | Death from cardiovascular causes, major cardiovascular events |
Heart Outcomes Prevention Evaluation (HOPE‑3)57-59 (n=12 500) | Primary prevention in men aged >55 y with at least 1 cardiovascular risk factor and women aged >60 y with at least 2 risk factors in 22 countries | Rosuvastatin 10 mg, candesartan 16 mg/HCTZ 12.5 mg (2 × 2 factorial design) | MACE, neurocognitive function, renal function |
PolyIran: pragmatic, cluster‑randomized trial38 (n = 6838) | Primary and secondary prevention of cardiovascular disease in a cohort of men and women aged 40–75 y in Iran | Atorvastatin 20 mg, HCTZ 12.5 mg, and either enalapril 5 mg or valsartan 40 mg, aspirin 81 mg | Major cardiovascular events, sudden death |
Polypill in primary prevention of CVD: an individual participant data meta‑analysis7 (n = 18 162) | Individual participant data meta‑analysis of 3 large randomized controlled trials (HOPE‑3, PolyIran, and TIPS‑3) on the effect of different polypills in primary prevention of CVD | Fixed‑dose combination treatment strategy with antihypertensive drugs plus statin, with or without aspirin | Death from cardiovascular causes, major cardiovascular events |
What is new in secondary prevention of cardiovascular disease
It is important to note that all research about the polypill was initially developed in the context of secondary cardiovascular prevention in patients with a history of MI for a number of reasons: 1) in patients with established CVD, the efficacy of pharmacological treatment of several cardiovascular risk factors (antihypertensive, antiplatelet, and lipid‑lowering treatments) has been unequivocally proven by RCTs,60-62 and a greater protective effect has usually been documented when these drugs are used in combination63; 2) secondary cardiovascular prevention is characterized by a more favorable number‑needed‑to‑treat ratio as compared with the primary prevention, with thus a more favorable cost‑benefit ratio; 3) despite its high economic burden for the health care system, the control of cardiovascular risk factors is still largely insufficient in patients with established CVD64 due to underprescription of drugs with documented protective effects, low treatment adherence and, in low‑income countries, limited accessibility to the health systems and medications, and the treatment costs too high for many patients.40,41
In the last 10 years, studies have shown that the polypill strategy can favorably affect cardiovascular prevention in patients with established CVD through their improved adherence. The Second Indian Polycap Study (TIPS‑2),5 the UMPIRE (Use of a Multidrug Pill In Reducing cardiovascular Events) trial,42 the IMPACT (Improving Adherence using Combination Therapy) trial,43 and the Kanyini GAP (Kanyini Guidelines Adherence with Polypill) open‑label trial44 showed a much greater adherence to the polypill‑based strategy than to the usual care with separate administration of appropriate drugs. Further evidence came from the research conducted in Spain at the Centro Nacional de Investigationes Cardiovasculares (CNIC). Preclinical and clinical studies with a polypill containing 100 mg of aspirin, 40 mg of simvastatin, and ramipril at various doses (2.5, 5, or 10 mg) confirmed its similar efficacy in comparison with individual administration of these 3 components.65,66 Subsequently, the polypill was tested in an RCT in the patients with a history of MI in whom separate administration of the 3 drugs was compared with the polypill strategy during 9 months. Both groups showed similar effects on BP and serum LDL‑C reduction, serious adverse events, and death. In line with the previous studies, adherence to treatment in the polypill group was significantly better than in the group in which the drugs were given separately (50.8% vs 41%; P = 0.019).9 Similar findings were reported for the second polypill also containing aspirin and ramipril at various doses, but in which simvastatin was replaced with atorvastatin (20–40 mg). It showed similar safety, tolerability, and bioequivalence of all its components with the drugs given separately.67 Based on all these data, the European Society of Hypertension published in 2017 a position statement on the clinical use of the polypill.68 Table 2 shows the clinical situations in which the use of the polypill is recommended.
Abbreviations: ACEI, angiotensin‑converting enzyme inhibitor; ARB, angiotensin AT1 receptor blocker; others, see Table 1 |
|
|
|
|
Recently, a retrospective observational NEPTUNO study37 using data from electronic health records, evaluated the efficacy of the CNIC‑polypill including aspirin, ramipril, and atorvastatin, on the incidence of recurrent MACE and control of cardiovascular risk factors in 6456 patients with established ASCVD, in comparison with 3 cohorts: 1) the same monocomponents taken separately (monocomponents); 2) equipotent drugs (equipotent); and 3) other drugs not included in the previous cohorts (other therapies). After a 2‑year follow‑up, the risk of MACE in the CNIC‑polypill cohort was lower than in all the other control groups (by 22% vs monocomponents; P = 0.017; by 25% vs equipotent drugs; P = 0.002; and by 27% vs other therapies; P = 0.001, respectively). The proportion of patients achieving strict BP control below 130/80 mm Hg increased more in the CNIC‑polypill cohort than in all control cohorts (+12.5% vs +6.3% in the monocomponent group; P <0.05; +12.5% vs +2.2% in the equipotent group; P <0.01; and +12.5% vs +2.4% in the other therapies; P <0.01). Similarly, the proportion of patients who achieved LDL‑C targets below 70 mg/dl increased more in the CNIC‑polypill cohort (+10.3% vs +4.9% in the monocomponent group; P <0.001; +10.3% vs +5.7% in the equipotent group; P <0.001; and +10.3% vs +4.9% in the other therapies; P <0.001). Finally, treatment persistence at the end of the study was also significantly higher in the patients receiving the CNIC‑polypill (72.1% vs 62.2%, 60%, and 54.2% for the monocomponent, equipotent, and other therapies group, respectively; P <0.001). This observational study is the first one showing that the use of the CNIC‑polypill is associated with a significant reduction in the incidence of recurrent MACE, together with a delayed time to event, in a large sample of real‑world patients with a history of ASCVD, as compared with 3 different active treatments (the same monocomponents in 3 Tablets, equipotent drugs given separately, and other therapies), reinforcing the usefulness of the polypill strategy for secondary cardiovascular prevention in clinical practice.
The results of the first and unique RCT assessing the effectiveness of the CNIC‑polypill on cardiovascular events and mortality in secondary cardiovascular prevention, the SECURE (Secondary Prevention of Cardiovascular Disease in the Elderly) trial,39 have been recently published. In this phase 3 RCT, 2499 patients with MI in the previous 6 months were randomized to a polypill‑based strategy or usual care. The polypill contained aspirin (100 mg), atorvastatin (20 or 40 mg), and ramipril (2.5, 5, or 10 mg). The primary outcome was a composite of cardiovascular death, nonfatal type 1 MI, nonfatal ischemic stroke, or urgent revascularization. The key secondary end point was a composite of cardiovascular death, nonfatal type 1 MI, or nonfatal ischemic stroke. The composite primary outcome was significantly (by 24%) reduced in the CNIC‑polypill group. Any of the components of the composite primary event occurred in 118 out of 1237 patients (9.5%) in the CNIC‑polypill group and in 156 out of 1229 patients (12.7%) in the usual care group (HR, 0.76; 95% CI, 0.60–0.96; P = 0.02). A significant reduction by 30% in the key composite secondary outcome was also observed in the CNIC‑polypill group. The secondary outcome event occurred in 101 patients (8.2%) in the CNIC‑polypill group and in 144 patients (11.7%) in the usual care group (HR, 0.70; 95% CI, 0.54–0.90; P = 0.005). Cardiovascular death rate was reduced by 33% in the CNIC‑polypill group. These results were consistent across all prespecified subgroups divided by age (<75 or ≥75 years), sex, absence of diabetes, type 2 diabetes, chronic kidney disease, and previous cardiovascular events. Patient‑reported medication adherence was by 17% higher in the CNIC‑polypill group than in the usual care group at 24 months, and adverse events were similar in both groups. The SECURE trial is the first RCT showing a significant reduction in the cardiovascular events and mortality with the safe use of a polypill‑based strategy that may be partly explained by increased adherence39 (Table 3).
Trial (sample size) | Population | Polypill composition | Outcomes |
Abbreviations: ASCVD, atherosclerotic cardiovascular disease; BP, blood pressure; FOCUS, Fixed‑dose combination drug for secondary cardiovascular prevention; MI, myocardial infarction; SBP, systolic blood pressure; UMPIRE, Use of a multidrug pill in reducing cardiovascular events; others see Table 1 | |||
Second Indian Polycap Study (TIPS‑2)5 (n = 518) | Previous vascular disease or diabetes mellitus from 27 centers in India | Simvastatin 20 mg, ramipril 5 mg, atenolol 50 mg, HCTZ 12.5 mg, and aspirin 100 mg, plus K+ | Effect of 2 polycaps vs 1 polycap on cardiovascular risk factors and tolerability |
UMPIRE randomized clinical trial42 (n = 2004) | Established CVD or high risk of CVD (5‑year CVD risk >15%) in India, the Netherlands, England, and Ireland | Aspirin 75 mg, atenolol 50 mg, simvastatin 40 mg, lisinopril 10 mg; or aspirin 75 mg, simvastatin 40 mg, lisinopril 10 mg, and HCTZ 12.5 mg | Adherence to medications and changes in SBP and LDL‑C. Secondary outcomes: MACE and cardiovascular death |
Improving Adherence using Combination Therapy (IMPACT)43 (n = 513) | Established CVD or estimated 5‑year CVD risk ≥15% in 54 primary care centers in New Zealand | Aspirin 75 mg, simvastatin 40 mg, and lisinopril 10 mg with either atenolol 50 mg or HCTZ 12.5 mg | Effect on adherence and mean change in BP and LDL‑C at 12 months |
Kanyini Guidelines Adherence with Polypill (Kanyini GAP)44 (n = 623) | Men and women aged ≥18 y with established CVD or estimated 5‑year CVD risk ≥15% from 33 primary care centers in Australia | Aspirin 75 mg, simvastatin 40 mg, and lisinopril 10 mg with either atenolol 50 mg or HCTZ 12.5 mg | Effect on adherence and mean change in BP and LDL‑C at 24 months |
FOCUS Trial in Secondary Prevention9 (phase 1, n = 2118; phase 2, n = 695) | MI survivors from Spain, Italy, Argentina, Brazil, and Paraguay | Aspirin 100 mg, simvastatin 40 mg, and ramipril 2.5, 5, or 10 mg | Adherence, feasibility, effect on CVD risk factor levels, safety, and tolerability |
NEPTUNO study37 (n = 6456) | Electronic health records from patients with established ASCVD in Spain | Aspirin 100 mg, atorvastatin 20 or 40 mg, and ramipril 2.5, 5, or 10 mg | Incidence of recurrent MACE |
Secondary Prevention of Cardiovascular Disease in the Elderly (SECURE) trial39 (n = 2499) | MI survivors within previous 6 months, aged ≥75 y or, ≥65 y with a major risk factor from 113 centers in Spain, Italy, France, Germany, Poland, Czech Republic, and Hungary | Aspirin 100 mg, atorvastatin 20 or 40 mg, ramipril 2.5, 5, or 10 mg | Composite of MACE (cardiovascular death, nonfatal ischemic stroke, nonfatal MI) at 36 months |
Considering the results of all the above mentioned studies, the use of a fixed‑dose cardiovascular polypill once daily to replace the multiple pill strategy of separate drugs, may be an integral part of a more efficient secondary prevention strategy. Simplification of treatment complexity and availability of the polypill allow for implementation of a widely applicable strategy to improve accessibility and adherence to treatment, leading to decreased risk of cardiovascular events and cardiovascular death.
Global implementation of a polypill strategy: challenges, barriers, and opportunities
The present rate of cardiovascular morbidity and mortality, together with the statistical projections of their devastating effects in the near future, particularly in LMIC, calls for an urgent reassumption of the polypill concept by stakeholders, to overcome the critical barriers to the implementation of major public health actions for all the CVD patients. The beneficial consequences of the polypill use for health systems are potentially relevant not only in low‑resource settings but also in all settings where adherence in primary or secondary prevention is low. The important gaps in the secondary cardiovascular prevention have been well documented and, despite the known benefits of effective and inexpensive pharmacotherapy, either for primary or secondary prevention of cardiovascular events and mortality, these treatments are underused in many LMIC, where the greatest burden of CVD occurs. There is an urgent need of a conceptual adaptation to the reality of noncommunicable diseases by stakeholders (the society, the associations of patients, scientific associations, pharmaceutical industry, insurance companies, and policy makers) to adopt and implement simple, cost‑effective strategies, such as the cardiovascular polypill for primary and secondary cardiovascular prevention. The wide use of a cardiovascular polypill in the context of public health strategies for either secondary prevention in patients with previous cardiovascular events, and for primary prevention in patients with advanced atherosclerosis and high cardiovascular risk, is a crucial strategy for the optimization of the best proven treatments.27,34,37,39,46,50,51,69
However, when a clinician decides to start a cardiovascular polypill or switch to it from previous treatment in order to simplify treatment for patients with hypertension, dyslipidemia, and advanced atherosclerotic disease or established cardiovascular event, a common problem is that the doses of the current antihypertensive drugs and statin used by the patient must be adapted to their hypertension grade and LDL‑C level, which may vary widely between different patients showing a similar global cardiovascular risk. Actually, this should not be a major problem, as the physician may choose from multiple versions of the CNIC‑polypill with different doses of the BP‑lowering and statin components, allowing for greater flexibility of its prescription and use.70
Based on the extensive data on the therapeutic interchangeability between RAS blockers, either ACEIs or ARBs, as well as between statins, switching between 6 different versions of the CNIC‑polypill with the same components, namely 100 mg of aspirin, 2 available doses of atorvastatin (20 mg or 40 mg), and 3 different doses of ramipril (2.5 mg, 5 mg, or 10 mg), is not a major problem. However, we must consider different real‑life, clinical situations, as patients may differ in the severity of BP and LDL‑C levels. Moreover, BP and LDL‑C targets to be achieved are different for primary or secondary cardiovascular prevention, and may require a stricter target depending on the associated cardiovascular risk factors and comorbidities.33 In each situation, the doses of the polypill components (ie, ramipril and / or atorvastatin) must be adapted and, in the patients whose BP or LDL‑C levels are not at target, the addition of further BP‑lowering drugs, for example, calcium channel blockers (CCBs) or diuretics, or lipid‑lowering drugs may be required.70
Figure 1 summarizes the steps that clinicians may follow in the patients with indications for a triple combination of a RAS blocker, a statin, and a low dose of aspirin, to switch from the current baseline multiple pill treatment with statins and ACEIs or ARBs combined with other medications for comorbidities (ie, glucose‑lowering drugs, diuretics, CCBs, antialdosterone drugs or β-blockers for HF, or post‑MI) to the CNIC‑polypill based regimen for treatment simplification and reduction of the number of daily pills.70
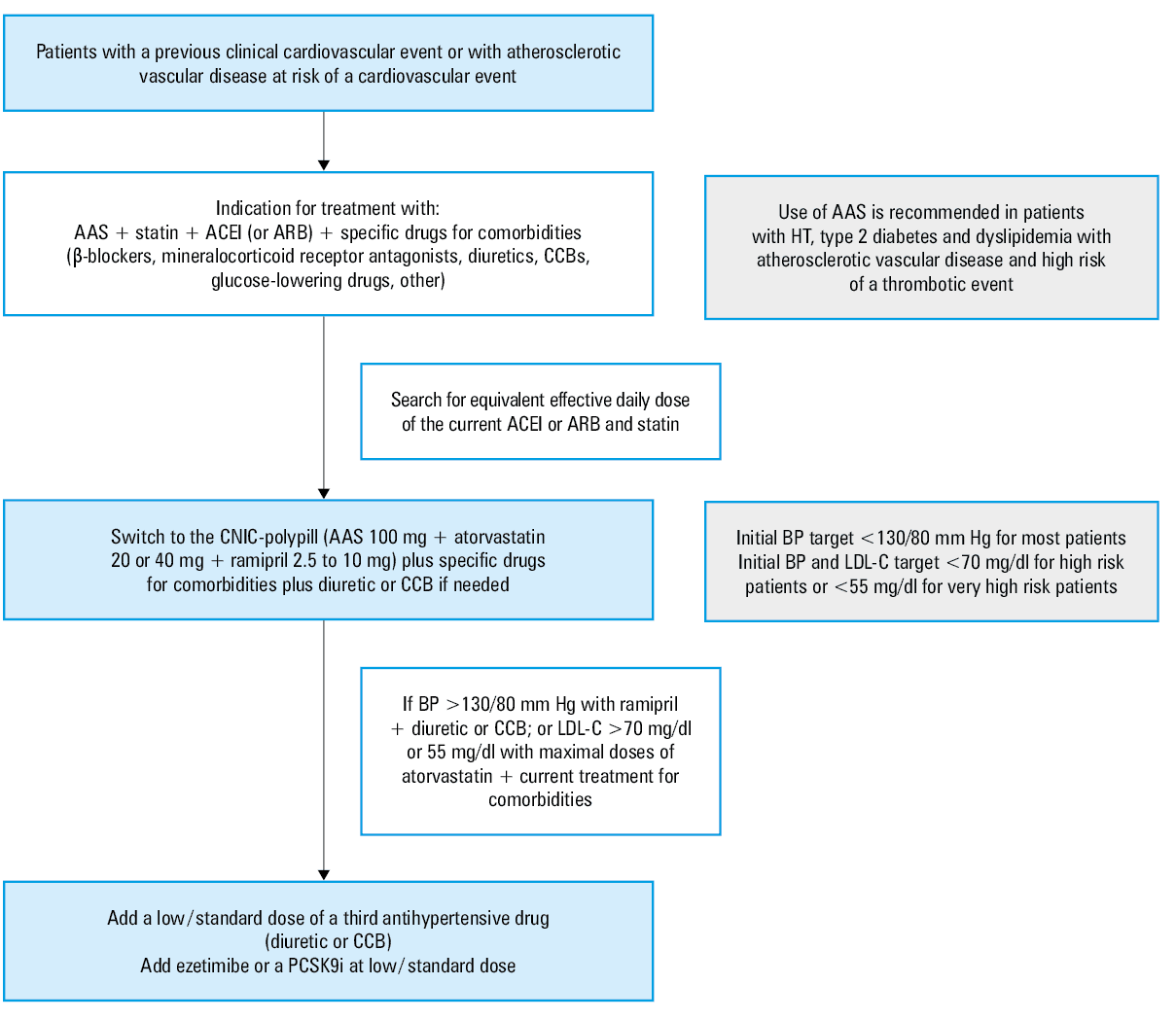
Abbreviations: AAS, aspirin; CCB, calcium channel blocker; HT, hypertension; PCSK9i, proprotein convertase subtilisin / kexin type 9 inhibitor; others see Tables 1 and 2
Summary and conclusions
CVDs are the leading cause of death worldwide, with a huge social impact, as well as growing burden for the global economy and health care systems. Many factors have been involved in the transition from the burden of transmissible chronic diseases to a nontransmissible chronic diseases such as CVDs: the effective vaccination programs and infectious diseases control, the change in dietary habits worldwide, the trend to sedentary lifestyle, industrialization with a shift from manual to sedentary labor, globalization, the surge in smoking habits and sugary beverage consumption in LMIC, and rapid urbanization, all have played a role.
The simultaneous increase in the prevalence of cardiovascular risk factors, together with a decline in mortality in high‑income countries in the past 2 decades, with improved survival after the first cardiovascular event, has led to a significant upsurge in the need for secondary cardiovascular prevention. The important role of nonadherence to cardioprotective drugs in increased frequency of cardiovascular outcomes and increased health care expenditure has become more clear.
The cardiovascular polypill has proven to be a key therapeutic strategy to improve medication adherence and treatment persistence in CVD prevention. There is clearly a need for a global polypill strategy in the current scenario of CVD based on improved accessibility, affordability, adherence, and cost‑effectiveness. The available data demonstrate that the cardiovascular polypill improves adherence to treatment and reduces morbidity and cardiovascular mortality in comparison with the usual care. Therefore, this medication should be an integral part of an effective strategy for primary and secondary cardiovascular prevention.
- WHO‑Wellcome Trust meeting on secondary prevention, World Health Organization & Wellcome Trust (London 2002). Secondary prevention of noncommunicable diseases in low‑and middle‑income countries through community‑based and health service interventions: World Health Organization‑Wellcome Trust meeting report, 1‑3 August 2001.
- Wald NJ, Law MR. A strategy to reduce cardiovascular disease by more than 80%. BMJ. 2003; 326: 1419. | Crossref
- Castellano JM, Sanz G, Ortiz AF, et al. A polypill strategy to improve global secondary cardiovascular prevention: from concept to reality. JACC. 2014; 64: 613‑621. | Crossref
- Indian Polycap Study (TIPS), Yusuf S, Pais P, et al. Effects of a polypill (Polycap) on risk factors in middle‑aged individuals without cardiovascular disease (TIPS): a phase II, double‑blind, randomised trial. Lancet. 2009; 373: 1341‑1351. | Crossref
- Yusuf S, Pais P, Sigamani A, et al. Comparison of risk factor reduction and tolerability of a full‑dose polypill (with potassium) versus low‑dose polypill (Polycap) in individuals at high risk of cardiovascular diseases. Circ Cardiovasc Qual Outcomes. 2012; 5: 463‑471. | Crossref
ARTICLE INFORMATION