Narrow-band imaging vs Lugol chromoendoscopy in screening for esophageal squamous cell neoplasia: a randomized trial
Key words: advanced imaging, chromoendoscopy, endoscopy, esophageal cancer, neoplasia



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Narrow-band imaging vs Lugol chromoendoscopy in screening for esophageal squamous cell neoplasia: a randomized trial
Introduction: To date, there has been no established optimal method for endoscopic detection of esophageal squamous cell neoplasia in high‑risk individuals.
Objectives: We aimed to compare the performance of narrow‑band imaging (NBI) and Lugol chromoendoscopy in screening for esophageal neoplasia among patients with a history of treatment for head and neck squamous cell cancer (HNSCC).
Patients and methods: We randomly assigned 300 patients who had completed curative treatment for HNSCC at least 1 year prior to the inclusion to undergo either NBI or Lugol endoscopy (2:1 ratio). Following white‑light examination of the esophagus, the assigned imaging study was performed, and biopsies were taken from any suspicious lesions identified using NBI or Lugol chromoendoscopy. The primary end point was positive predictive value (PPV) of the biopsied lesion for a diagnosis of esophageal neoplasia (high‑grade intraepithelial neoplasia [HG‑IEN] or invasive esophageal squamous cell carcinoma [ESCC]). The secondary end points included the number of biopsied lesions, duration of esophagus examination, and endoscopy tolerance.
Results: In 294 patients included in the final analysis (NBI, n = 204; Lugol chromoendoscopy, n = 90), we diagnosed 3 ESCCs (1.02%) and 2 HG‑IENs (0.68%). The PPV of NBI and Lugol chromoendoscopy in per‑lesion analysis was 7.69% (95% CI, 0.94%–25.1%) and 8.11% (95% CI, 1.7%–21.9%), respectively (P >0.99). NBI outperformed Lugol chromoendoscopy in terms of the rate of patients requiring biopsy (12.75% vs 41.11%; P = 0.003), duration of esophagus examination (3.5 min vs 5.15 min; P <0.001), and endoscopy tolerance assessed on the visual analog scale (25 mm vs 36.5 mm; P = 0.002).
Conclusions: With a PPV comparable to that of Lugol chromoendoscopy, but a lower number of biopsies required, shorter examination time, and better patient tolerance, NBI could be considered the primary screening method for ESCC in patients with HNSCC.
What's new?
An optimal method for endoscopic detection of esophageal squamous cell neoplasia in high‑risk individuals has not been established yet. To our best knowledge, this is the first controlled study that compared Lugol chromoendoscopy and narrow‑band imaging (NBI) in a large number of patients with a history of curative treatment for head and neck cancers. Additionally, it was conducted in the Western population, whereas most of the previous reports originate from areas with high incidence of esophageal squamous cell neoplasia (mostly Asia). We demonstrated similar diagnostic accuracy of both imaging methods; however, NBI outperformed Lugol chromoendoscopy in screening for esophageal squamous cell neoplasia due to the lower number of biopsies required, shorter esophagus examination time, and better patient tolerance. These results indicate that NBI should be considered the primary advanced imaging modality in screening for esophageal squamous cell carcinoma among patients at high risk for developing the disease.
Introduction
Patients with head and neck squamous cell cancer (HNSCC) are at an increased risk of developing synchronous and metachronous esophageal squamous cell carcinoma (ESCC) given the exposure to risk factors common for these types of cancer, such as excessive alcohol intake and smoking.1 Depending on the geographic region and the primary location of HNSCC, the risk of developing ESCC ranges from 3.2% to 14.9%,2-4 with a significantly higher incidence in patients with hypopharyngeal and oropharyngeal cancers than in individuals with cancers originating from the oral cavity, or those with laryngeal or nasopharyngeal cancers.4-6 Metachronous ESCC is one of the major factors contributing to poor prognosis and treatment failure in patients with HNSCC. Early detection and treatment of ESCC are crucial to improve survival of those patients; however, they remain challenging due to the subtle appearance of small, superficial lesions on routine white‑light endoscopy. To improve the detection, advanced imaging methods, such as conventional and virtual chromoendoscopy, are recommended.7,8 Lugol chromoendoscopy is an established method of early squamous neoplasia detection; however, it is a demanding and time‑consuming technique, and it comes with adverse effects, such as nausea, laryngitis, chest pain, and allergic reaction to iodine.9,10 Narrow‑band imaging (NBI) utilizes blue and green light wavelengths to enhance visualization of the mucosal surface and vascular microarchitecture.11,12 This increasingly available method is simple, fast, and free of adverse effects.
The aim of this randomized trial was to compare the diagnostic performance of NBI and Lugol chromoendoscopy in screening for esophageal neoplasia in patients who had completed curative treatment for HNSCC.
Patients and methods
Study design
This parallel‑group, randomized study was conducted between December 2013 and November 2016 at the Maria Skłodowska‑Curie Institute – Oncology Center in Warsaw, Poland. Eligible patients with a history of curative treatment for HNSCC were randomly assigned at a 2:1 ratio to the NBI or Lugol chromoendoscopy group. The study was approved by the Ethics Committee of the Centre of Postgraduate Medical Education, Warsaw, Poland (65/PB/2013), and it was registered at ClinicalTrials.gov under the number NCT02435602.
Patients
We included adult patients with a performance status of 0 to 2 according to the Zubrod scale,13 who had previously underwent curative treatment for histologically confirmed squamous cell cancer of the larynx, oral cavity, oropharynx, or hypopharynx, and who had completed the treatment at least 1 year before the enrollment. We excluded the patients with a history of allergy to iodine and with clinical conditions precluding upper gastrointestinal endoscopy (ie, severe heart or lung disease).
None of the patients included in the study had undergone endoscopy screening (white‑light endoscopy, NBI, or Lugol chromoendoscopy) prior to the study inclusion.
All participants signed a written, informed consent to participate in the study and a separate informed consent for the endoscopy procedure.
Procedures
All patients enrolled in the study were asked to fill out a questionnaire concerning environmental risk factors (Supplementary material).
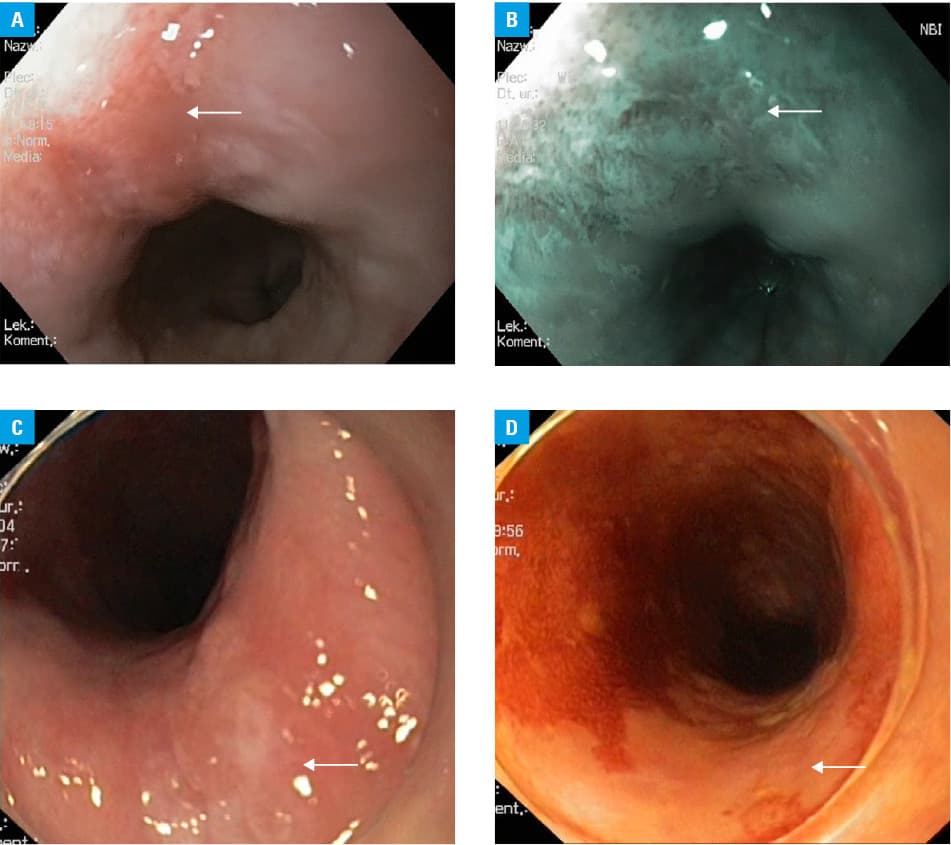
Endoscopy was performed by 4 experienced endoscopists, in accordance with a specifically prepared examination protocol. Before the study, all 4 endoscopists had participated in additional training, which comprised at least 10 examinations with NBI followed by Lugol chromoendoscopy. Approximately 30 minutes before the endoscopy, the patients were given a 50‑ml solution of 10% acetylocysteine for better mucosal visualization during the procedure. All patients underwent a high‑definition white‑light endoscopy examination (Olympus HQ180J) of the esophagus, stomach, and duodenum, followed by NBI or Lugol chromoendoscopy of the esophagus according to the randomization group (randomization code was disclosed before the endoscopy). The patients were offered local anesthesia (lignocaine spray) alone or in combination with conscious sedation (midazolam and fentanyl). In the NBI group, the esophagus was screened for demarcated brownish areas with an irregular vascular pattern (Figure 1A and 1B). In the Lugol chromoendoscopy group, the entire esophagus was stained with 10 to 20 ml of a 2% Lugol solution using a spray‑type catheter, and examined for the presence of any well‑demarcated Lugol‑voiding lesions with a diameter of 5 mm or larger, or any Lugol‑voiding lesions accompanied with a pink sign (Figure 1C and 1D).14 The lesion size was assessed by visual comparison with the diameter of open biopsy forceps. Mucosal abnormalities were recorded with regard to their location, size, and the number of lesions within the esophagus. At least 2 biopsy specimens were obtained from each suspicious lesion for histologic assessment. The histologic diagnosis was established by an internationally recognized expert in gastrointestinal pathology (AM), who was blinded to the advanced imaging method used. Histology was classified into 5 categories: negative for neoplasia, indefinite for neoplasia, low‑grade intraepithelial neoplasia (LG‑IEN), high‑grade intraepithelial neoplasia (HG‑IEN), and invasive squamous cell carcinoma, according to the Vienna classification.15
Procedural times were recorded by an endoscopy assistant by measuring the total time of the esophagus examination with white‑light and advanced endoscopy imaging. All examinations were video‑recorded. After the examination, all patients assessed the tolerance of the procedure using the 100‑mm visual analog scale (VAS).
Outcomes
The primary outcome measure was the positive predictive value (PPV) of the detected and biopsied lesions for the diagnosis of esophageal neoplasia (HG‑IEN and ESCC).
Secondary outcome measures included the number of biopsied lesions, esophagus examination time, and endoscopy tolerance. All patients were followed using the National Cancer Registry database for a subsequent diagnosis of esophageal cancer up to December 31, 2017.
Randomization and masking
The eligible patients were randomized at a 2:1 ratio to either NBI or Lugol chromoendoscopy using a computer‑generated randomization list created by an independent statistician. The list was prepared using simple randomization stratified by the primary cancer site (laryngeal and oral cavity cancer vs oropharyngeal and hypopharyngeal cancer), and patients’ sex. Patient enrollment was performed in each case by the principal investigator, who was not involved in performing the endoscopy examinations. The randomization list was opened by the principal investigator immediately before the endoscopy procedure. Only the principal investigator and the endoscopist were aware of the allocation. The patients and the pathologist were not informed about the group assignment.
Statistical analysis
Data were presented as means and SDs or medians and interquartile ranges (IQRs) for continuous variables, and percentages for categorical variables. To calculate the 95% CIs, the binomial method was used.
Categorical variables were compared using the χ2 test or the Fisher exact test. Continuous variables were compared using the t test (when normally distributed) or the Mann–Whitney test (when the distribution was non‑normal). The distribution of each variable was assessed by plotting histograms. A P value below 0.05 was considered significant. All analyses were performed with the Stata software, version 13.1 (Stata Corporation, College Station, Texas, United States).
The sample size was calculated assuming the expected PPV of Lugol chromoendoscopy and NBI of 20% and 45%, respectively, based on the available data from Asian studies.16-18 No data from Western studies were available. To detect this difference at a significance level of 0.05 and with an 80% power, 53 lesions were needed in each study group. Assuming a 60% average frequency of detected lesions per patient in Lugol chromoendoscopy and 30% in NBI, and a 10% dropout rate, the required sample size was estimated to be 100 patients in the Lugol chromoendoscopy group and 200 patients in the NBI group.
Results
A total of 318 patients were assessed for eligibility. Of them, 18 individuals did not meet the inclusion criteria (Figure 2), so finally 300 patients were enrolled (between December 10, 2013 and November 22, 2016) and randomly assigned to the NBI group (n = 209) or the Lugol chromoendoscopy group (n = 91). A total of 6 patients were excluded from the analysis, leaving 204 and 90 individuals in the NBI and Lugol chromoendoscopy groups, respectively (Figure 2). The 2 groups did not differ in terms of sex, age, primary site of cancer, alcohol consumption, and smoking habits (baseline characteristics presented in Table 1). The median (IQR) time interval between the completion of treatment for HNSCC and surveillance procedures was 35.5 (18.2–56.5) months, and it was not different between the 2 groups (Lugol chromoendoscopy, 34.9 [18.8–61.3] months vs NBI, 35.7 [18.2–55.8] months; P = 0.84).
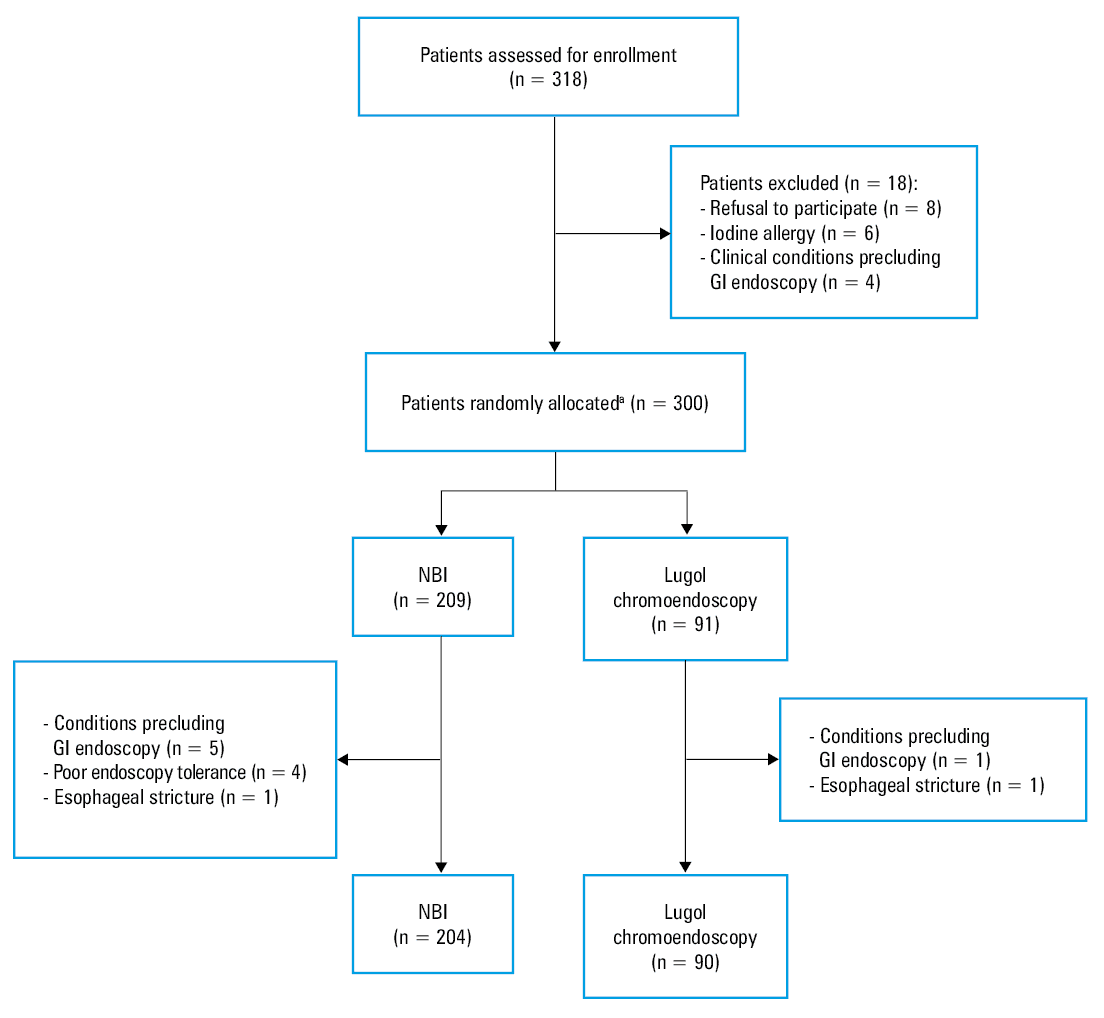
Abbreviations: GI, gastrointestinal; NBI, narrow‑band imaging
Characteristics | NBI (n = 204) | Lugol chromoendoscopy (n = 90) | P value | ||
Abbreviations: see Figure 2 | |||||
Sex, n (%) | Women | 48 (23.5) | 16 (17.8) | 0.27 | |
Men | 156 (76.5) | 74 (82.2) | |||
Age, y, mean (SD) | 62.5 (9.6) | 63.3 (9.9) | 0.51 | ||
Primary location of the head and neck cancer, n (%) | Oral cavity | 26 (12.75) | 10 (11.11) | 0.94 | |
Oropharynx | 71 (34.8) | 31 (34.44) | |||
Hypopharynx | 16 (7.84) | 6 (6.67) | |||
Larynx | 91 (44.61) | 43 (47.78) | |||
Consumption of alcohol, n (%) | 112 (54.9) | 51 (56.67) | 0.78 | ||
Smoking status, n (%) | Current smoker | 60 (29.41) | 16 (17.78) | 0.09 | |
Ex‑smoker | 102 (50) | 55 (61.11) | |||
Nonsmoker | 42 (20.59) | 19 (21.11) | |||
All patients decided to undergo the examination with local anesthesia only (which is a standard outpatient approach in Poland).
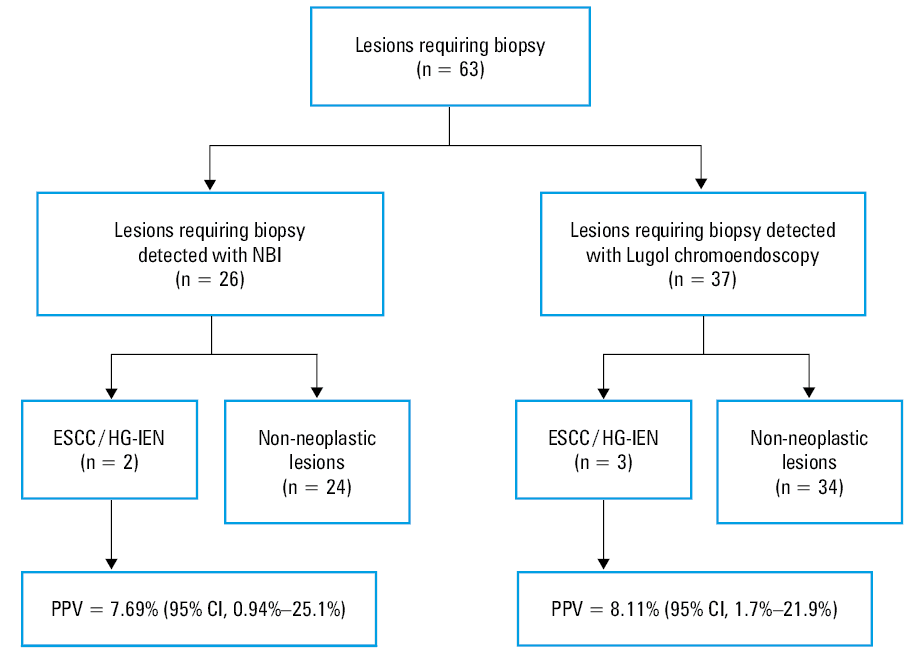
In 43 of 294 patients (14.6%), a total of 63 suspicious esophageal lesions requiring biopsy were detected. Of the 63 lesions identified, 5 (7.9%) were true positive (2 HG‑IEN, 3 ESCC). The median size of neoplastic and non‑neoplastic lesions was 12 mm and 6 mm, respectively (P = 0.052). Characteristics of the patients diagnosed with HG‑IEN and ESCC are presented in Table 2.
Sex | Age, y | Index localization of HNSCC | Time from the completion of HNSCC treatment, mo | Histologic diagnosis | Lesion size, mm | Chromoendoscopic method | Treatment | Follow‑up durationa, mo | Cigarette packs per year, n | Consumption of alcoholb |
a After endoscopic treatment
b Consumption of any alcohol in the past 12 months
Abbreviations: EMR, endoscopic mucosal resection; ESCC, esophageal squamous cell carcinoma; ESD, endoscopic submucosal dissection; HG‑IEN, high‑grade intraepithelial neoplasia; HNSCC, head and neck squamous cell cancer; M, male; others, see Figure 2 | ||||||||||
M | 46 | Hypopharynx | 12 | HG‑IEN | 12 | NBI | ESD | 46 | 0 | Yes |
M | 67 | Oropharynx | 26 | ESCC | 20 | Lugol chromoendoscopy | ESD | 38 | 47 | Yes |
M | 64 | Oropharynx | 15 | ESCC | 6 | Lugol chromoendoscopy | ESD | 7 | 16 | Yes |
M | 69 | Larynx | 37 | ESCC | 7 | NBI | EMR | 14 | 22.5 | No |
M | 63 | Larynx | 12 | HG‑IEN | 15 | Lugol chromoendoscopy | ESD | 6 | 90 | Yes |
In the NBI group, 26 lesions (12.75%) detected in 20 patients required biopsy. Of these, 2 were true positive (1 HG‑IEN, 1 ESCC). The non‑neoplastic lesions were LG‑IEN (1 lesion), esophagitis (20 lesions), and normal mucosa (3 lesions).
In the Lugol group, 37 lesions (41.11%) detected in 23 patients required biopsy. Of these, 3 were true positive (1 HG‑IEN, 2 ESCC). The non‑neoplastic lesions comprised LG‑IEN (1 lesion), esophagitis (26 lesions), and normal mucosa (7 lesions).
The PPV of NBI and Lugol chromoendoscopy in a per‑lesion analysis was 7.69% (95% CI, 0.94%–25.1%) and 8.11% (95% CI, 1.70%–21.9%), respectively, without a significant difference (Figure 3).
The PPV of NBI and Lugol chromoendoscopy in a per‑patient analysis was 10% (95% CI, 1.2%–31.7%) and 13% (95% CI, 2.8%–33.6%), respectively (P = 0.34).
There was no significant difference in the detection rate of neoplasia between the Lugol chromoendoscopy and NBI groups (3.3% and 0.96%, respectively; P = 0.17). The prevalence of lesions requiring biopsy was significantly higher in the Lugol chromoendoscopy group than in the NBI group (41.11% vs 12.75%, respectively; P = 0.003) (Table 3). The median (IQR) duration of esophageal examination was significantly longer for Lugol chromoendoscopy than that for NBI (5.15 [4.5–6.67] min vs 3.5 [2.83–4.67] min, respectively; P <0.001) (Table 3). The median (IQR) endoscopy tolerance (using VAS) was significantly better for NBI than for Lugol chromoendoscopy (25 [9.5–44] mm vs 36.5 [17‑53] mm, respectively; P = 0.002) (Table 3). Neoplastic lesions were detected in 4% of current smokers (3 out of 76), in 0.6% of ex‑smokers (1 out of 157) and in 1.6% of nonsmokers (1 out of 61) (P = 0.12). Neoplastic lesions were also detected in 2.5% of alcohol drinkers (4 out of 163) and in 0.8% of patients from the nonregular drinkers group (P = 0.39). There were no adverse events in either group.
Secondary outcomes | NBI (n = 204) | Lugol chromoendoscopy (n = 90) | P value |
Abbreviations: IQR, interquartile range; VAS, visual analog scale; others, see Figure 2 | |||
Lesions requiring biopsy per patient, n (%) | 26 (12.75) | 37 (41.11) | 0.003 |
Esophagus examination time, min, median (IQR) | 3.50 (2.83–4.67) | 5.15 (4.5–6.67) | <0.001 |
Endoscopy tolerance (VAS), mm, median (IQR) | 25 (9.5–44) | 36.5 (17–53) | 0.002 |
None of the patients without a primary diagnosis of esophageal neoplasia was diagnosed with symptomatic ESCC over 24.2 months of follow‑up using the National Cancer Registry.
Discussion
In this parallel‑group, randomized study we demonstrated that with a similar PPV, but a lower number of biopsies required, shorter esophagus examination time, and better patient tolerance, NBI outperformed Lugol chromoendoscopy as a screening tool for esophageal squamous cell neoplasia in a high‑risk population. To our best knowledge, this is the first study with such a large sample that compared the 2 advanced imaging modalities in patients with a history of curative treatment for head and neck cancers in a controlled design. Of note, it was conducted in the Western population, whereas most of the previous reports originate from countries with a high incidence of ESCC. In our study, neoplastic lesions (both HG‑IEN and ESCC) were detected in 5 out of 294 patients (1.7%). Previous reports showed higher prevalence of esophageal squamous cell neoplasia (3.2%–14.9%).2-4 There are 3 possible explanations for these differences. Firstly, most of those studies were conducted in areas with high prevalence of ESCC (ie, Taiwan, Brazil). Secondly, in those reports, the most common index location of HNSCC was the hypopharynx, which shows the strongest association with ESCC. In our study, the most common location of HNSCC was the larynx (45.6%), which is in line with HNSCC epidemiology in Poland. Additionally, only advanced neoplastic lesions (HG‑IEN and ESCC) were considered in our analysis, whereas in some other studies, LG‑IENs were also included in the esophageal cancer group.19 The PPV of the detected and biopsied lesions for the diagnosis of esophageal neoplasia did not differ significantly between NBI and Lugol chromoendoscopy (7.69% and 8.11%), which indicates that the diagnostic performance of NBI and Lugol chromoendoscopy is comparable. In other studies, the reported PPVs ranged widely (9.8%–94.1%) for both NBI and Lugol chromoendoscopy.17-20 The PPV depends on the prevalence of the disease in the tested population; therefore, the inclusion and exclusion criteria play a pivotal role in assessing the usefulness of the test. In our study, only the patients without any symptoms of esophageal cancer (ie, dysphagia, odynophagia) were considered, whereas other studies also included patients with dysphagia and odynophagia,21,22 or even those with an established diagnosis of esophageal cancer.14,23 Moreover, in one of the previous reports,21 only patients at the highest risk of developing esophageal cancer (ie, those with hypopharyngeal carcinoma) were included. All these factors significantly affected the PPV. The low PPV in the current study can be explained by the lower incidence of esophageal cancer in Europe than in Asia, and by the strictly defined inclusion criteria. At the same time, it highlights the importance of conducting the study in the European population, and showing the differences in the incidence of esophageal cancer between patients with head and neck cancer in Europe and Asia, which is where most of the other reports come from.
Although Lugol chromoendoscopy has been considered the gold standard to enhance the visualization of early esophageal lesions, the administration of Lugol solution is time consuming and may lead to side effects, including nausea, laryngitis, chest pain, and allergic reaction to iodine. NBI is an optical technique in which the light of specific blue and green wavelengths is used to enhance the contrast between the surface of the mucosa and vascular architecture. In recent meta‑analyses,7,8 NBI presented similar sensitivity but higher specificity than Lugol chromoendoscopy. However, most of the observational studies included in these meta‑analyses compared only the diagnostic accuracy of NBI and Lugol chromoendoscopy, while neglecting a crucial comparison of very important procedure‑related parameters, such as the number of biopsies, esophagus examination time, and endoscopy tolerance. Our study is the first one to include a routine evaluation of patient endoscopy tolerance using VAS.
The likelihood of a lesion being neoplastic is known to increase with its size, and although biopsy specimens are usually obtained from lesions greater than or equal to 5 mm in diameter, some authors suggest that the cutoff point should be a diameter of 10 mm.24,25 Ide et al17 found that the performance (specificity and PPV) of NBI and Lugol chromoendoscopy increased significantly when lesions with a diameter greater than 10 mm were analyzed. In our study, the difference in size between the biopsied lesions histologically confirmed to be HG‑IEN or ESCC and the non‑neoplastic lesions was not significant. On the other hand, if biopsies had been taken only from the lesions with a diameter of 10 mm or greater, 2 cases of ESCC would not have been diagnosed.
To prevent advanced cancer and improve survival rates, early detection of ESCC in patients with a history of HNSCC treatment is necessary. Moreover, early detection offers curative treatment with minimally invasive endoscopic techniques, that is, endoscopic mucosal resection or endoscopic submucosal dissection. Complete removal of the primary tumor and the absence of regional lymph node metastases are essential for successful endoscopic treatment. The risk of lymph node metastases for lesions confined to the epithelium (m1) or lamina propria (m2) is 0% and 3.3%, respectively. When the tumor infiltrates the muscularis mucosa (m3) or the superficial third of the submucosa (sm1), the risk of lymph node metastases increases from 10.2% (m3) to 26.5% (sm1).26 Therefore, endoscopic resection has been recommended for m1 and m2 infiltrations as “absolute” indicators. Endoscopic resection could be considered curative treatment for m3 and sm1 tumors smaller than 200 µm with no clinical evidence of lymph node metastases.27 In our study, all neoplastic lesions (2 HG‑IENs, 3 ESCCs) were detected at an early stage, and all patients underwent successful endoscopic treatment. Furthermore, none of the remaining patients (ie, those without a primary diagnosis of esophageal neoplasia) was diagnosed with symptomatic ESCC over the 24.2‑month follow‑up. In addition, the mean time of ESCC development in our patients was 20.4 months from the completion of oncologic treatment for HNSCC. Thus, our observations are in agreement with other reports in which an average time interval between the diagnosis of 2 primary cancers was 3 years.28
Although there is no global consensus on the routine surveillance of ESCC in patients with HNSCC, some gastrointestinal endoscopy societies recommend upper gastrointestinal chromoendoscopy screening in patients with head and neck cancer. However, further comparative effectiveness research is necessary to generate evidence for the efficacy and cost‑effectiveness of this approach, as well as for optimal surveillance intervals. It is beyond the scope of our study to justify the need for a surveillance program in patients with HNSCC. However, once surveillance endoscopy is considered, NBI should be encouraged. Moreover, according to our results, it seems reasonable to identify the subgroup of patients with HNSCC at the highest risk of developing ESCC to optimize the surveillance programs.
Limitations
We acknowledge certain limitations of the present study. Firstly, due to the lower than assumed number of neoplastic esophageal lesions detected, the study was underpowered. Secondly, a single patient did not undergo both examinations, so it was impossible to establish the sensitivity, specificity, negative predictive value, and accuracy of each imaging modality. However, owing to the parallel‑group, randomized study design, we eliminated the potential bias of the single operator knowing the location of suspicious areas. In some publications,12,17 a sequential approach (NBI endoscopy and Lugol chromoendoscopy performed by the same endoscopist) was used, limiting blind evaluation of each diagnostic method.
The assumptions regarding PPV were based on previously conducted Asian studies because data from Western studies were not available.
Only the patients with a history of curative treatment for NHSCC were included in the study, which precluded the possibility of assessing the risk of synchronous ESCC. However, this is in line with currently proposed screening programs, which usually start after completion of curative treatment for head and neck cancers.3,29
This was a single‑center study; however, it was performed in the tertiary reference center in which most of HNSCC and ESCC patients from Poland are treated.
Conclusions
In conclusion, NBI and Lugol chromoendoscopy have a similar PPV; however, due to the lower number of biopsies required, shorter examination time, and better patient tolerance, NBI could be considered the primary advanced imaging modality in screening for ESCC among patients at high risk of developing the disease. However, further multicenter studies with a larger sample size are warranted to confirm these results.
- Slaughter DP, Southwick HW, Smejkal W. Field cancerization in oral stratified squamous epithelium; clinical implications of multicentric origin. Cancer. 1953; 6: 963‑968. | Crossref
- Moschler O, Spahn TW, Middelberg‑Bisping C, et al. Chromoendoscopy is a valuable tool for screening of high‑risk patients with head and neck cancer for early detection of esophageal cancer. Digestion. 2006; 73: 160‑166. | Crossref
- Petit T, Georges C, Jung GM, et al. Systematic esophageal endoscopy screening in patients previously treated for head and neck squamous‑cell carcinoma. Ann Oncol. 2001; 12: 643‑646. | Crossref
- Wang WL, Lee CT, Lee YC, et al. Risk factors for developing synchronous esophageal neoplasia in patients with head and neck cancer. Head Neck. 2011; 33: 77‑81. | Crossref
- Muto M, Hironaka S, Nakane M, et al. Association of multiple Lugol‑voiding lesions with synchronous and metachronous esophageal squamous cell carcinoma in patients with head and neck cancer. Gastrointest Endosc. 2002; 56: 517‑521. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION