Benzodiazepine use and mortality in chronic heart failure
Key words: benzodiazepines, heart failure, mortality, older adults



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Benzodiazepine use and mortality in chronic heart failure
Introduction: The prognostic implications of using benzodiazepines (BZD) in heart failure (HF) patients are still unknown.
Objectives: This study aimed to assess the association of BZD use with all‑cause death in ambulatory, chronic HF patients.
Patients and methods: We investigated a retrospective cohort of ambulatory HF patients with left ventricular systolic dysfunction (LVSD). The patients were followed up from their first medical appointment until January 2021 and all‑cause mortality was the primary end point. The Cox regression analysis was used to assess the association between BZD use and all‑cause mortality. Subgroup analyses were performed considering age, sex, body mass index (BMI), respiratory disease, chronic kidney disease (CKD), and New York Heart Association (NYHA) class. Multivariable models were built to account for confounders.
Results: We studied 854 patients (69% men), of mean (SD) age 71 (13) years, of whom 51% had severe LSVD, and 242 (28.3%) regularly used BZD. During a median follow‑up of 46 months, 443 patients (51.9%) died. BZD use predicted no crude survival disadvantage in the entire investigated group and in the subgroup analysis according to sex, respiratory disease, BMI, and NYHA class. BZD use was not mortality‑associated among patients aged 75 years and younger. However, in those older than 75 years the hazard ratio (HR) of all‑cause death was 1.3 (95% CI, 0.99–1.69; P = 0.06). BZD use seemed safe in the patients without CKD, but in those with CKD it was associated with worse survival (HR, 1.33; 95% CI, 1.02–1.73). In a multivariable‑adjusted analysis, the use of BZD was independently associated with increased death risk (HR, 1.36; 95% CI, 1.06–1.75).
Conclusions: The patients medicated with BZD presented a 36% higher risk of dying. BZD should probably be used with caution, particularly in older HF patients and in those with CKD.
What's new?
The safety of benzodiazepine (BZD) use in heart failure (HF) patients is largely unknown. We report, in a relatively large cohort of chronic HF patients, that the use of BZD is associated with higher all‑cause mortality. This was particularly evident in older patients and those with chronic kidney disease. BZD are largely used in clinical practice and physicians treating HF patients should be aware of their potential risks.
Introduction
Benzodiazepines (BZD) are the most often prescribed anxiolytics and hypnotics, with 3%–5% of the general population using them chronically.1 Psychotropic medications are prescribed to 18% of the patients with heart failure (HF); and BZD are the most often used drugs, accounting for 68% of the prescriptions.2 Anxiety is highly prevalent in HF, with about 13% of the patients fulfilling the requirements for a formal diagnosis of anxiety disorder.3 Insomnia is also a common complaint in clinical practice and is frequently mentioned by HF patients, with a reported prevalence as high as 73%.4,5 Insomnia has been associated with adverse prognosis in HF patients6; in contrast, the relationship between anxiety and HF is less clear, with no studies to date showing relevant association with mortality.3,7
BZD target BZD sites of γ-aminobutyric acid (GABA) type A (GABAA) receptors and allosterically increase the GABAA receptors’ affinity for GABA. GABA is an inhibitory neurotransmitter, exerting inhibitory effects in the central nervous system (CNS), including hypnosis, anxiolysis, seizure suppression, muscle relaxation, and amnesia.8,9 Therefore, BZD, by increasing the receptors’ affinity for GABA, potentiate all these inhibitory actions.
Despite being commonly prescribed, BZD have been suggested to be associated with increased risk of HF hospitalization,10 and concerns regarding the safety of BZD use in patients with HF have been raised. The prognostic implications of BZD use in chronic HF patients are still largely unknown. We aimed to assess the prognostic impact of BZD use in ambulatory patients with chronic HF.
Patients and Methods
We conducted a retrospective cohort study in ambulatory patients with HF with left ventricular systolic dysfunction (LVSD) followed in a specialized HF clinic of a tertiary care academic hospital. The HF clinic of the Internal Medicine Department of the São João Hospital Center was founded in 1996, and follows adult patients mainly with HF with ejection fraction (EF) below 50%. The patients with EF equal to or above 50% with difficult congestion management are also attended to.
HF was considered according to the updated guidelines11,12 as a condition characterized by the presence of symptoms and signs of congestion and / or hypoperfusion, and echocardiographic documentation of functional abnormalities. Only the patients with LVSD (EF <50%) were considered in the analysis. Left ventricular dysfunction was considered severe when the left ventricular EF was equal to or below 30%. All consecutive adult (aged 18 years or above) patients with HF with EF below 50% attending the clinic from 2012 onward were eligible for the study. Patients with no information regarding BZD use and those with EF equal to or above 50% (preserved HF or fully recovered HF) were excluded from the analysis. The index observation was considered the first medical visit of each consecutive patient from January 2012 until May 2018. Demographic data and data concerning comorbidities, physical examination, laboratory parameters, and medication at the end of the index visit were recorded. Comorbidities were defined as described below. Arterial hypertension was defined as systolic blood pressure equal to or above 140 mm Hg and / or diastolic blood pressure equal to or above 90 mm Hg on at least 2 separate measurements, the presence of a previous diagnosis, or record of antihypertensive pharmacological treatment. Diabetes mellitus (DM) was defined as a known previous diagnosis, current prescription of hypoglycemic agents, fasting venous blood glucose level above 126 mg/dl, or random glucose level above 200 mg/dl. In addition, all patients with glycosylated hemoglobin level equal to or above 6.5% were considered diabetic. Coronary heart disease (CHD) was defined as a history of acute myocardial infarction or significant CHD confirmed on imaging. Data on respiratory disease were taken from medical records and included obstructive sleep apnea and / or chronic obstructive pulmonary disease. The patients were considered to have chronic kidney disease (CKD) if the index estimated glomerular filtration rate (eGFR) according to the Modification Diet and Renal Disease formula was below 60 ml/min/1.73 m2. Cerebrovascular disease was considered when the patients had a history of previous stroke or cerebral hemorrhage or if cerebral vascular lesions were confirmed on imaging. Dementia was considered in the case of a known previous diagnosis or prescription of antidementia drugs.
The patients were followed from the first medical appointment in the HF clinic until January 2021. Follow‑up was set since the first medical appointment from 2012 onwards. The end point was all‑cause mortality, and vital status was ascertained by consulting the hospital registries and by telephone contact with the patients or their relatives. No patient was lost to the follow‑up.
The study protocol conformed to the ethical guidelines of the declaration of Helsinki. It was approved by institutional ethics committee (CE‑89‑23). Due to the retrospective nature of the study design the patient informed consent was waived.
Statistical analysis
Categorical variables are presented as numbers and percentages. Continuous variables are presented as mean with SD when normally distributed, and as median and interquartile range (IQR) when non‑normally distributed. Patients were categorized according to their BZD use, and those using and not using BZD were compared with the χ2 test for categorical variables, the t test for continuous variables with a normal distribution, and the Mann–Whitney test for continuous variables with a skewed distribution. The Kaplan–Meier method was used to determine survival curves in the patients using and not using BZD, and the log‑rank test was employed to compare the curves. The Cox regression analysis was used to assess the association between BZD use and all‑cause mortality. Subgroup analyses were additionally performed considering age (≤75 and >75 years), sex, body mass index (BMI) (≤25 and >25 kg/m2), coexistence of respiratory disease, CKD, and New York Heart Association (NYHA) class (<II vs ≥II). Multivariable analyses adjusting for confounders were also performed. Model 1 considered adjustments for age, sex, BMI, respiratory disease, CKD, and NYHA class; model 2 included age, sex, BMI, respiratory disease, CKD, NYHA class, and major comorbidities (DM, arterial hypertension, atrial fibrillation, ischemic HF, cerebrovascular disease, and dementia); and model 3 included variables considered in model 2 and also disease‑modifying therapy, and hemoglobin and B‑type natriuretic peptide (BNP) levels.
The P value was considered significant if it was below 0.05. The data were stored and analyzed using the SPSS software version 20.0 (IBM, Armonk, New York, United States).
Results
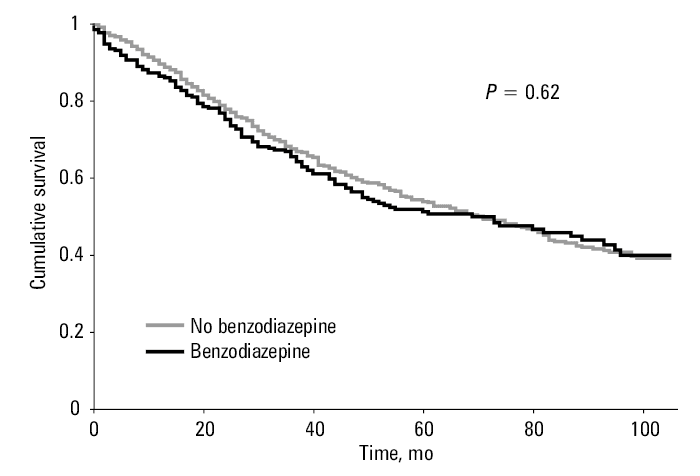
A total of 854 chronic HF patients were investigated (69% men), of mean age 73 (13) years. Of those, 51% had severe LSVD, and their HF was ischemic in 46.8%. Comorbidity burden was high: 61.2% of the patients had arterial hypertension and 38.6% were diabetic. At the end of the index appointment, 92.4% patients were on β-blockers, 83.6% on angiotensin‑converting enzyme inhibitors or on angiotensin receptor blockers, and 29.3% on mineralocorticoid receptor antagonists. A total of 242 (28.3%) patients used BZD regularly. Most of the patients (214 [88.4%]) were treated with intermediate‑action BDZ, 22 (2.6%) were medicated with long‑action BDZ, and only 6 (0.7%) were on short‑action BDZ. Over 95% of the patients were already taking BDZ upon referral to the HF clinic. The drugs were mostly prescribed by their primary care physician, and insomnia was the main cause for their initiation. A residual proportion of the patients (<5%) had a psychiatric consultation prior to BDZ prescription. Detailed and accurate causes for BDZ use were not possible to ascertain in most of the cases. During a median (IQR) follow‑up of 46 (26–77) months, 443 (51.9%) patients died. Table 1 shows general characteristics of the patients and a comparison between those medicated and not medicated with BZD. No major differences existed between the patients using and not using BZD, except for a significantly higher prevalence of men in the group not using BZD. The patients medicated with BZD were slightly younger (70 vs 71 years), and presented better renal function. Among the non‑BZD users, 51.6% died after a median follow‑up of 46 months, and among BZD users, mortality rate was 52.5% over a similar follow‑up period. Figure 1 depicts the Kaplan–Meier survival curves according to BZD use. Globally, the use of BZD predicted no survival disadvantage in chronic HF, with a crude hazard ratio (HR) of 1.05 (95% CI, 0.86–1.29; P = 0.62). Table 2 shows the crude association with mortality according to the prespecified subgroups. BZD use also did not predict crude survival disadvantage in the patients with and without respiratory disease, either in men or women, in patients with BMI equal to or below 25 kg/m2 and those with excess body weight, or in patients in NYHA class I and those in higher classes. When considering age, the use of BZD appeared safe among patients up to 75 years, however, the HR of all‑cause death in those older than 75 years was 1.3 (95% CI, 0.99–1.69; P = 0.06). When considering renal function, the use of BZD showed no association with mortality in the patients without CKD, but in those with CKD the use of BZD was associated with worse survival (HR, 1.33; 95% CI, 1.02–1.73; P = 0.04).
Characteristics | All (n = 854) | Not using BZD (n = 612) | Using BZD (n = 242) | P value |
SI conversion factors: to convert hemoglobin to g/l, multiply by 10, BNP to mg/l, by 1.
Abbreviations: BNP, B‑type natriuretic peptide; BZD, benzodiazepine; eGFR, estimated glomerular filtration rate; HF, heart failure; IQR, interquartile range; LVSD, left ventricular systolic dysfunction; MRA, mineralocorticoid receptor antagonist; NYHA, New York Heart Association; RASi, renin angiotensin system inhibitor | ||||
Age, y, mean (SD) | 71 (13) | 71 (13) | 70 (13) | 0.04 |
Male sex, n (%) | 555 (65) | 415 (67.8) | 140 (57.9) | 0.006 |
Arterial hypertension, n (%) | 523 (61.2) | 375 (61.3) | 148 (61.2) | 0.97 |
Diabetes mellitus, n (%) | 330 (38.6) | 243 (39.7) | 87 (36) | 0.31 |
Atrial fibrillation, n (%) | 281 (32.9) | 207 (33.8) | 74 (30.6) | 0.36 |
Ischemic HF, n (%) | 400 (46.8) | 291 (47.5) | 109 (45) | 0.51 |
Respiratory disease, n (%) | 192 (22.5) | 147 (24) | 45 (18.6) | 0.08 |
Dementia, n (%) | 45 (5.3) | 30 (4.9) | 15 (6.2) | 0.45 |
Cerebrovascular disease, n (%) | 155 (18.2) | 107 (17.5) | 48 (19.8) | 0.43 |
Hemoglobin, g/dl, mean (SD) | 13.1 (1.8) | 13.1 (1.8) | 13.1 (1.8) | 0.85 |
eGFR, ml/min/1.73 m2, median (IQR) | 55 (40–74) | 54 (38–73) | 60 (42–77) | 0.04 |
BNP, pg/ml, median (IQR) | 283 (121–637) | 285 (115–624) | 273 (129–652) | 0.75 |
Severe LVSD, n (%) | 438 (51.3) | 310 (50.7) | 128 (52.9) | 0.55 |
NYHA class I | 286 (33.5) | 210 (34.3) | 76 (31.4) | 0.33 |
NYHA class II | 391 (45.8) | 283 (46.2) | 108 (44.6) | |
NYHA class III/IV | 177 (20.7) | 119 (19.4) | 58 (24) | |
β-Blockers, n (%) | 789 (92.4) | 570 (93.1) | 219 (90.5) | 0.19 |
RASi, n (%) | 714 (83.6) | 519 (84.8) | 195 (80.6) | 0.13 |
MRA, n (%) | 229 (29.2) | 177 (28.9) | 72 (29.8) | 0.81 |
Follow‑up, mo, median (IQR) | 46 (26–77) | 16 (27–77) | 46 (24–74) | 0.43 |
Mortality, n (%) | 413 (51.9) | 316 (51.6) | 127 (52.5) | 0.82 |
Parameter | BZD use: crude HR (95% CI) | P value |
Abbreviations: BMI, body mass index; HR, hazard ratio; others, see Table 1 | ||
No respiratory disease (n = 653) | 1.51 (0.91–1.45) | 0.24 |
Respiratory disease (n = 192) | 0.78 (0.50–1.24) | 0.29 |
Women (n = 299) | 0.89 (0.63–1.25) | 0.51 |
Men (n = 555) | 1.18 (0.91–1.52) | 0.22 |
Age ≤75 years (n = 473) | 0.94 (0.68–1.29) | 0.71 |
Age >75 years (n = 381) | 1.29 (0.99–1.69) | 0.06 |
BMI <25 kg/m2 (n = 517) | 1.26 (0.91–1.73) | 0.16 |
BMI ≥25 kg/m2 (n = 335) | 0.92 (0.67–1.26) | 0.59 |
NYHA I (n = 286) | 1.03 (0.67–1.29) | 0.89 |
NYHA ≥II (n = 568) | 1.04 (0.82–1.31) | 0.75 |
eGFR ≥ 60 ml/min/1.73 m2 (n = 364) | 1.00 (0.68–1.47) | 0.99 |
eGFR <60 ml/min/1.73 m2 (n = 490) | 1.33 (1.02–1.73) | 0.04 |
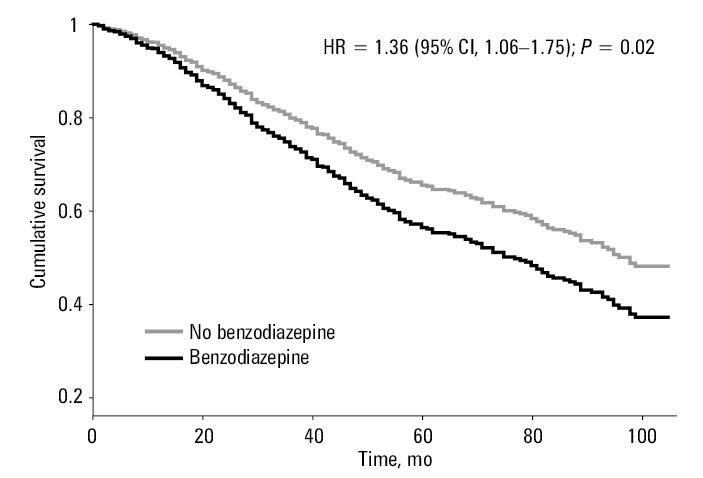
In a multivariable model including the prespecified subgroups as confounding variables, the safety of BZD use was additionally challenged, and the patients medicated with BZD had a multivariable adjusted HR of dying in the upcoming 4 years of 1.31 (95% CI, 1.03–1.67; P = 0.03). With successive models including further possible confounders, the association of BZD use with mortality persisted, even after adjusting for BNP levels, a clearly established and robust prognostic biomarker in HF.13,14 Table 3 shows the crude and multivariable adjusted‑analysis associations of BZD use with all‑cause mortality. Figure 2 depicts the adjusted survival curves. The HF patients with LVSD using BZD presented significantly higher all‑cause mortality than those not medicated with BZD.
Benzodiazepine use | All‑cause mortality: HR (95% CI) | P value |
Model 1: adjustment for sex, age (per 10‑year increase), eGFR (per 10 ml/min/1.73 m2), BMI (per kg/m2 increase), symptomatic HF (NYHA class ≥II), and concomitant respiratory disease
Model 2: adjustment for variables in model 1+ comorbidities (diabetes, arterial hypertension, atrial fibrillation, ischemic HF, cerebrovascular disease, and dementia)
Model 3: adjustment for variables in model 2 + basal hemoglobin, basal BNP (per pg/ml), and disease‑modifying therapy (β-blockers, RASis, and MRA)
| ||
Crude | 1.05 (0.86–1.29) | 0.62 |
Multivariable‑adjusted model 1 | 1.29 (1.01–1.64) | 0.04 |
Multivariable‑adjusted model 2 | 1.31 (1.03–1.66) | 0.03 |
Multivariable‑adjusted model 3 | 1.36 (1.06–1.75) | 0.02 |
Discussion
Our findings in a real‑world cohort of HF patients with LVSD question the safety of BZD use. Despite crude survival being similar in patients medicated and not medicated with BZD, in the subgroup analysis we report significantly higher death risk for patients with eGFR below 60 ml/min/1.73 m2 and nonsignificantly worse survival in older patients (>75 years). The older patients are an increasing subset of HF population,15 and CKD is highly prevalent among individuals with HF.16 Therefore, the use of BZD appears to negatively impact prognosis in 2 important subgroups of the HF population. Additionally, with successive adjustments for potential confounders, an independent association between BZD use and higher all‑cause mortality persisted. The patients medicated with BZD had an overall 36% (95% CI, 5%–75%) higher risk of all‑cause mortality in the long run.
Despite previous studies in non‑HF specific contexts showing mixed results regarding the association between BZD use and all‑cause mortality,17 recent literature suggests an excessive risk of death associated with BZD use; in some cases it was associated with a 2‑fold increase in all‑cause mortality.18,19 To date, the mechanisms behind this trend toward higher mortality among BZD users are not well understood. Possible explanations include the described association of BZD use with falls and cognitive impairment, and the fact that withdrawal syndrome may occur and be life‑threatening.1,20 Additionally, combination of BZD with other drugs, such as opioids, has been reported to confer increased long‑term mortality risk in older adult patients and in polymedicated ones.19
In addition to their impact on mortality in the global population, BZD have also been linked to increased hospitalizations for HF in HF patients. The relationship between insomnia, hypnotics use, and HF prognosis is largely unknown.10 It may be partially explained by activation of the hypothalamic pituitary adrenal axis and activation of the renin‑angiotensin‑aldosterone and sympathetic nervous systems.9,10,21
BZD prescription in CKD is challenging as there is an increased risk of enhanced central depressant effect. Most BZD are oxidatively metabolized by the cytochrome P450 (CYP540) enzymes (phase I), conjugated with glucuronide (phase II), and excreted almost entirely with urine. This effect of BZD is probably multifactorial, resulting from reduced hepatic clearance due to limited CYP450 activity, reduced protein‑binding due to increased unbound fraction, increased levels of BZD, and enhanced sensitivity of the CNS to BZD.22 Literature regarding the safety of BZD use in CKD is scarce; some studies suggest an increased risk of death in this group of patients, particularly in those with end‑stage kidney disease on renal replacement therapy with hemodialysis.23,24 Furthermore, the association between BZD and mortality was independent of the disease severity, age, and comorbidities.25 The higher death risk in this subgroup of patients may be attributable to changes in pharmacodynamics and pharmacokinetics, resulting in increased accumulation of BZD and amplification of their effects leading to adverse cognitive and psychomotor outcomes.25 Our results concur with those findings in patients with renal impairment, and support the claim that BZD should be used with greater caution in this group of patients.
The possible influence of age on the prognostic impact of BZD use is also largely undetermined. Studies have showed diverse results concerning the association of BZD use with mortality in older adults.17,20,26,27 No association has been reported between BZD use and increased all‑cause mortality in individuals aged 85 years or older, however, an increase in mortality related to fractures was observed among BZD users.27 Mathieu et al20 reported an association between BZD use and increased risk of all‑cause mortality in older adults, which was particularly higher in patients aged 65 to 80 years. Moreover, the use of BZD has been associated with poor outcomes in hip fractures, motor vehicle crashes, and suicides. Additionally, it may exacerbate pre‑existing conditions, such as obstructive sleep apnea, or may be associated with psychomotor impairment and cognitive problems.26 Our results in chronic HF patients indicate a higher risk of death among older BZD users. The mechanisms underlying the increased mortality risk are still unknown, however, altered pharmacodynamics is a potential explanation.28
Study limitations
Our study has some limitations that should be addressed. It was a retrospective, single‑center study with inherent setbacks concerning data quality and availability, and generalizability of the results. Our cohort included HF patients followed in a specialized HF clinic of a tertiary care academic hospital, and therefore cannot be directly applicable to the whole HF patient population. Another major limitation is the fact that the patients did not undergo a systematic psychiatric evaluation, and the reasons for chronic BZD use were not systematically collected. The patients often arrived at the clinic with the prescription of BZD from their primary care physician, and the prescription of noncardiovascular drugs is generally maintained, except for cases with clear side effects or evident contraindications. Our analysis was not adjusted for conditions such as anxiety and / or depression, with the last clearly recognized to be associated with worse prognosis in HF.9,10 Delirium, although rare in ambulatory patients, was also not accounted for in the multivariable models. However, the prevalence of conditions such as dementia and cerebrovascular disease was similar in the patients taking and not taking BZD, and these comorbidities were accounted for in the multivariable adjustment. Despite being a 21st century real‑world HF population, the patients were still not on drugs currently recognized as clear prognosis‑modifying drugs in HF with reduced EF, such as sodium‑glucose cotransporter‑2 inhibitors and angiotensin receptor / neprilysin inhibitors. It is intriguing that after adjustment for confounders, a significant association between BDZ use and mortality was found, while no crude association was detected. Still, the fact that multivariable models can unravel an association undetected in a crude analysis is known and statistically explained.29 Notwithstanding all the shortcomings, this is the first European report based on nonadministrative data that addresses the safety of BZD use in chronic HF. We studied a large enough population for a long enough time to detect a significantly shortened survival among BZD users. Chung et al30 have recently described a similar hazardous effect of BDZ use in a large cohort of HF patients with reduced EF, however, their study was based on the administrative Taiwanese databases.30 Another strength of our study, when comparing to that work, is the fact that we collected information on the eGFR, and creatinine clearance has been suggested as a potential confounder in the association of BDZ with mortality.23
BZD are commonly prescribed drugs for a multitude of frequent, difficult to characterize and diagnose mental conditions, and their potential hazardous association with decreased survival should lead clinicians to exercise greater caution while prescribing them. This brings to light a new concept of medication reconciliation. The problem is being increasingly recognized, particularly in older adults with higher vulnerability to inappropriately prescribed drugs that is mainly due to the changes in the drug pharmacokinetics and pharmacodynamics with age, higher rates of multimorbidity and polypharmacy, and lower adherence to complex treatment regimens.31,32 The use of available tools, such as the Screening Tool of Older Person’s Prescriptions and the Screening Tool to Alert to Right Treatment may help capture the cases of common, potentially inappropriate medications in patients aged 65 years or older.33,34 In addition to these tools, widely used in Europe, the Beers Criteria for Potentially Inappropriate Medication Use in Older Adults,35 published by the American Geriatrics Society, emphasize the need for deprescribing of superfluous medications to promote the patient safety. BZD are encouraged to be prescribed carefully, as their use may be associated with an increased risk of falls, worsening of chronic respiratory failure, and impaired cognitive functions.35
Conclusions
We question the safety of using BZD in the patients with chronic HF with LVSD. The patients medicated with BZD presented a 36% higher risk of dying in the upcoming 4 years. BZD should probably be used with caution, and their use should be revised particularly in older adult HF patients and in those with CKD.
- Soyka M. Treatment of benzodiazepine dependence. N Engl J Med. 2017; 376: 2399‑2400. | Crossref
- Cromhout PF, Christensen AV, Jorgensen MB, et al. Exploring the use of psychotropic medication in cardiac patients with and without anxiety and its association with 1‑year mortality. Eur J Cardiovasc Nurs. 2022; 21: 612‑619. | Crossref
- Celano CM, Villegas AC, Albanese AM, et al. Depression and anxiety in heart failure: a review. Harv Rev Psychiatry. 2018; 26: 175‑184. | Crossref
- Guilbert JJ. The world health report 2002 ‑ reducing risks, promoting healthy life. Educ Health (Abingdon). 2003; 16: 230. | Crossref
- Milani SA, Raji MA, Chen L, et al. Trends in the use of benzodiazepines, Z‑hypnotics, and serotonergic drugs among US women and men before and during the COVID‑19 pandemic. JAMA Netw Open. 2021; 4: e2131012. | Crossref
ARTICLE INFORMATION