Guillain–Barré syndrome following severe COVID-19 directly after kidney transplantation



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Guillain–Barré syndrome following severe COVID-19 directly after kidney transplantation
In COVID‑19, besides respiratory system manifestations, neurologic symptoms have also been reported, including Guillain–Barré syndrome (GBS). GBS is an autoimmune inflammatory neuropathy affecting peripheral nerves. Recently, there have been reports describing an association between COVID‑19 and GBS.1 We present a case of GBS following COVID‑19 that occurred 2 weeks after kidney transplantation.
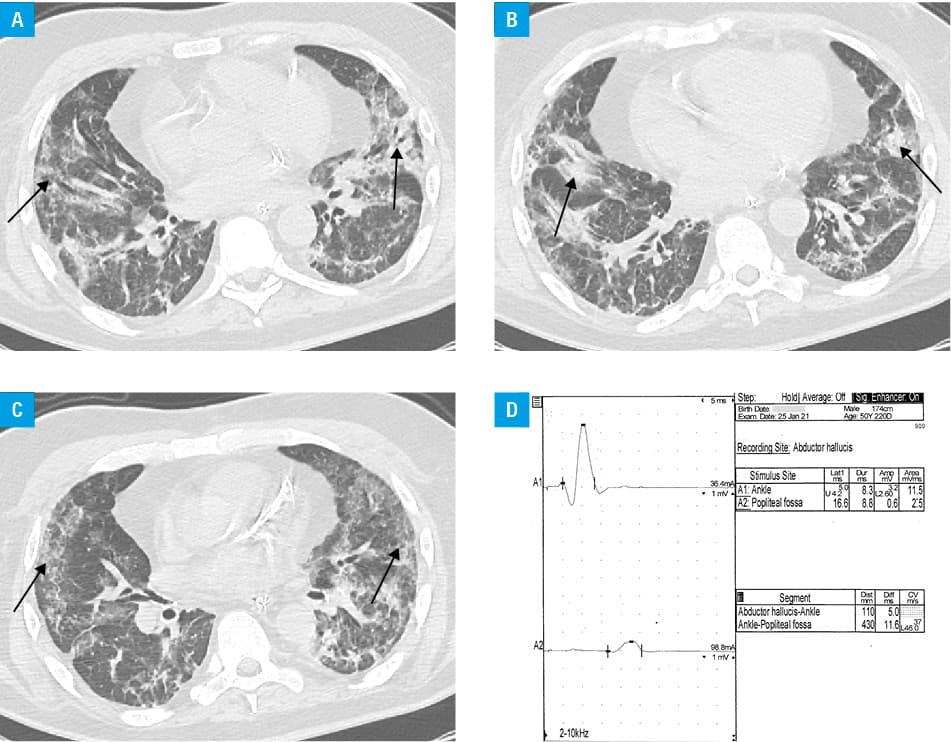
A 50‑year‑old man with end‑stage renal disease of the only kidney underwent kidney transplantation in 2020. Immunosuppressive therapy consisted of cyclosporine A, mycophenolate mofetil, and glucocorticoids, with rabbit antithymocyte globulin induction therapy. On postoperative day 19, the patient reported wheezing and chest tightness, with no increase in the levels of inflammatory markers. SARS‑CoV‑2 infection was confirmed with the polymerase chain reaction test; computed tomography revealed that 56% of the lungs were affected (Figure 1A–1C). Immunosuppression was reduced to glucocorticoids and a low dose of cyclosporine A. Despite standard (for 2020) therapy with remdesivir, glucocorticoids, and convalescent plasma, the patient’s condition deteriorated. Treatment in the intensive care unit led to a gradual improvement. On postoperative day 40, the patient developed extremity weakness with tremor, areflexia, and hypoesthesia of the lower limbs. Cerebrospinal fluid analysis revealed increased protein level (166.8 mg/dl; reference range, 14–45 mg/dl) with normal cell count (albuminocytologic dissociation). On the electroneurographic tests no response was found in any of the peroneal nerves from the extensor digitorum brevis muscles and from the tibialis anterior muscle on the right side. On the left side the motor‑evoked potential amplitude was markedly reduced (0.2 mV; reference range >4.5 mV), and the conduction velocity was 27 m/s. In both tibial nerves the amplitudes and conduction velocities were slightly reduced (37 m/s on the left side, 40 m/s on the right side; reference range >42 m/s). We were not able to obtain any F‑waves or sensory responses in the lower limb nerves (Figure 1D). On the examination performed 3 years earlier (2018), the motor conduction parameters had been completely normal. Treatment with therapeutic plasma exchange (TPE) and rehabilitation were administered. After TPE, mobility of the lower limbs improved. The patient continued rehabilitation and 12 months after GBS, he has only mild hyperesthesia of the feet and normal kidney function. He received 4 doses of an mRNA vaccine starting a month after recovery, with no recurrence of GBS.
GBS is characterized by ascending symmetric motor weakness, loss of tendon reflexes, and sensory disturbances progressing to the maximal disability within 4 weeks. The diagnosis and management should be based on current guidelines.2 Most cases of GBS in the transplant population have been reported after hematopoietic stem cell transplantation due to graft versus host disease. GBS has also been reported in heart, liver, and kidney transplant recipients following viral infections (ca 15 cases published, mainly caused by cytomegalovirus infection). The recipients were treated mainly with antiviral agents and intravenous immunoglobulins (IVIG) and TPE (5 cases).3
The COVID‑19 etiology of peripheral polyneuropathy after renal transplantation was previously reported once, and the neuropathy occurred much later than in our case (13 months vs 19 days).4 In GBS triggered by SARS‑CoV‑2 infection the onset of symptoms usually overlaps with COVID‑19. Our patient presented symptoms on the 21st day after COVID‑19 diagnosis. In most of the reported cases, the patients received a single course of IVIG (0.4 g/kg/day for 5 days), which led to improvement within 8 weeks, whereas our patient was treated with TPE and improvement was noted earlier—after 2 weeks.5 Our case adds to the growing body of evidence on the connection between COVID‑19 and GBS. SARS‑CoV‑2 infection may lead to nerve involvement both directly or by a cytokine storm. Another possible explanation are antibodies produced against a viral spike protein cross‑reacting with the host’s nerve tissue, causing damage to the spike‑bearing gangliosides and glycolipids of the peripheral nerve.1
The diagnosis of GBS should be considered in transplant recipients who experience limb weakness, with SARS‑CoV‑2 infection as a possible cause.
- Filosto M, Cotti Piccinelli S, Gazzina S, et al. Guillain‑Barré syndrome and COVID‑19: an observational multicentre study from two Italian hotspot regions. J Neurol Neurosurg Psychiatry. 2021; 92: 751‑756. | Crossref
- Leonhard SE, Mandarakas MR, Gondim FAA, et al. Diagnosis and management of Guillain‑Barré syndrome in ten steps. Nat Rev Neurol. 2019; 15: 671‑683. | Crossref
- Ostman C, Chacko B. Guillain‑Barré syndrome post renal transplant: a systematic review. Transpl Infect Dis. 2019; 21: e13021. | Crossref
- Juric I, Basic‑Jukic N. Guillain‑Barré syndrome following SARS‑CoV‑2 infection in kidney transplant recipient successfully treated with therapeutic plasma exchange. Ther Apher Dial. 2023 Jan 31. [Epub ahead of print]
- Caress JB, Castoro RJ, Simmons Z, et al. COVID‑19‑associated Guillain‑Barré syndrome: the early pandemic experience. Muscle Nerve. 2020; 62: 485‑491. | Crossref
ARTICLE INFORMATION