Left ventricular end-diastolic pressure index predicts outcomes in patients with left ventricular diastolic dysfunction



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Left ventricular end-diastolic pressure index predicts outcomes in patients with left ventricular diastolic dysfunction
Introduction
Left ventricular diastolic dysfunction (LVDD) is caused by increased left ventricular (LV) chamber stiffness and impaired LV relaxation, which strongly correlate with myocardial fibrosis (MF).1 LVDD is considered the preliminary of heart failure with preserved ejection fraction (HFpEF). During the late phase of LVDD, MF induces adverse myocardial remodeling, which leads to the occurrence of HFpEF.2 In patients with HFpEF, the impaired left ventricular diastolic function (LVDF) is difficult to reverse.3,4 Poor LVDF is associated with greater all‑cause mortality and adverse cardiac events, which include newly developed myocardial ischemia, arrhythmia, myocardial infarction (MI), angina pectoris, and HF.5 Intervention in the early phase of LVDD may reverse impaired LVDF.6,7
During the early stage of LVDD, left ventricular end‑diastolic pressure (LVEDP) is the only abnormal parameter, and invasive cardiac catheterization remains the gold standard for measuring LVEDP.8 However, cardiac catheterization may be difficult to popularize in clinical settings due to the risks and costs associated with invasive hemodynamic evaluation. Several researchers have studied the relationship between noninvasive echocardiographic assessment and LVDD.9 However, very few of them have attempted to develop an equation to evaluate LVEDP when invasive real‑time detection of LVEDP by left ventricular catheter was performed as the gold standard.10,11 In our previous studies, in which we performed echocardiographic assessments during invasive cardiac catheterization, we found that left atrial volume index (LAVI), peak A duration time in mitral diastole (AD), pulmonary vein A‑wave duration time (PvaD), reverse A‑wave velocity of pulmonary veins during atrial contraction (PVa), pulmonary vein systolic S‑wave velocity (PVs), and peak velocity of tricuspid regurgitation (TRmax) were independently associated with the actual, measured LVEDP. The optimal multiple regression equation was the LVEDP index that can reflect LVEDP with high feasibility.12
In this work, we aimed to determine the effect of the LVEDP index on the prognosis of patients with LVDD. We also investigated the relationship between LVEDP index and MF, which induced LV remodeling.
Patients and methods
Study population
A total of 120 patients with suspected coronary artery disease, who underwent coronary angiography and LV catheterization between March 2017 and January 2018, were enrolled in the present study. All the patients had a preserved (≥55%) left ventricular ejection fraction (LVEF). The exclusion criteria were as follows: age below 18 years, valvular heart disease, a history of cardiac surgery, atrial fibrillation, severe mitral or aortic regurgitation, mitral stenosis or severe mitral calcification, hypothyroidism, malignant disease, lack of clinical follow‑up, MI, and poor echocardiographic images. This study was approved by the Ethics Committee of the Affiliated Hospital of Jiangsu University (SWYXLL20170601).
The patients were divided into a group with LVEDP above 15 mm Hg (n = 77) and a group with LVEDP below or equal to 15 mm Hg (n = 43), according to the LV catheterization outcomes. The echocardiography parameters were analyzed in both groups (Supplementary material, Tables S1–S3). Multiple regression analysis yielded the following optimal equation: LVEDP index = 0.292 LAVI + 0.35 PVa + 0.04 TRmax + 0.075 (PvaD –AD) – 0.109 PVs – 6.773.
Then, the patients were divided into 2 groups according to the cutoff value of the LVEDP index: 1) high level of the LVEDP index (H‑LVEDP): LVEDP index equal to or above 14.63 (n = 78), and 2) low level of the LVEDP index (L‑LVEDP): LVEDP index below 14.63 (n = 42). This was an observational study, and we did not intervene with the treatment of the primary diseases.
All the patients were regularly followed‑up every 6 months for 4 years, by both clinical visits and telephone calls. The primary end point included all‑cause mortality and adverse cardiac events. The adverse cardiac events were defined as new occurring myocardial ischemia, arrhythmia, MI, angina pectoris, and HF.
Two‑dimensional Doppler echocardiography
The echocardiographic parameters, such as pulsed‑wave peak early (E) and atrial (A) velocities of mitral inflow, their ratio (E/A), and early mitral inflow deceleration time, duration of pulmonary vein flow and mitral inflow during atrial contraction (Ar–A duration), flow propagation velocity (Vp), PVs, early diastolic D‑wave velocity (PVd), PVa, and PvaD were determined as described previously.13,14 Different grades of LVDD were diagnosed according to the 2016 American Society of Echocardiography and the European Association of Cardiovascular Imaging guidelines. Routine echocardiography was performed in all the patients at baseline and after 36 months of the follow‑up.
Enzyme‑linked immunosorbent assay
Fibrotic parameters, such as procollagen type I, procollagen type III, and matrix metallopeptidase 9 (MMP‑9), were assessed using commercial biotin / avidin‑based enzyme‑linked immunosorbent assay kits (eBiosciences, San Diego, California, United States).
Statistical analysis
Descriptive data are expressed as median with interquartile range in the case of a skewed distribution, or as mean (SD). Continuous variables were compared using the t test, continuous variables that were not normally distributed were compared using the Mann–Whitney test, and categorical variables were analyzed with the χ2 test. Spearman rank correlation tests were used to investigate bivariate correlations. The receiver operating characteristic (ROC) curves were plotted. Based on the gold standard of invasive manometry, the ROC curve was used to evaluate the diagnostic efficacy of each echocardiographic parameter on LVEDP. The echocardiographic parameters were analyzed by stepwise regression equation and the Pearson method was used to analyze the correlation between the estimated and measure value of LVEDP. The Bland–Altman plot was used to analyze the agreement between the LVEDP index and the measured LVEDP. The optimal prognostic cutoff value (Youden index) of the LVEDP index was derived from the area under the curve (AUC) assessed at baseline. The optimal cutoff point was calculated with the following formula: Sensitivity + Specificity – 1. We tested whether the LVEDP index was associated with the primary end point by using the Cox regression analysis. Baseline clinical characteristics and echocardiographic parameters were used as adjustment variables. The primary outcome was a successful completion of 80% or more of the scheduled treatment observations in the 4 years following randomization. We used CIs for one proportion of PASS to calculate the minimum sample size. A sample size of 70 was found to produce a 2‑sided 95% CI with a width equal to 0.199 when the sample proportion was 0.8. All the analyses were performed using the SPSS software (v. 11.5, SPSS, Chicago, Illinois, United States). P values below 0.05 were considered significant.
Results
Receiver operating characteristic curve for predicting left ventricular end‑diastolic pressure using the left ventricular end‑diastolic pressure index
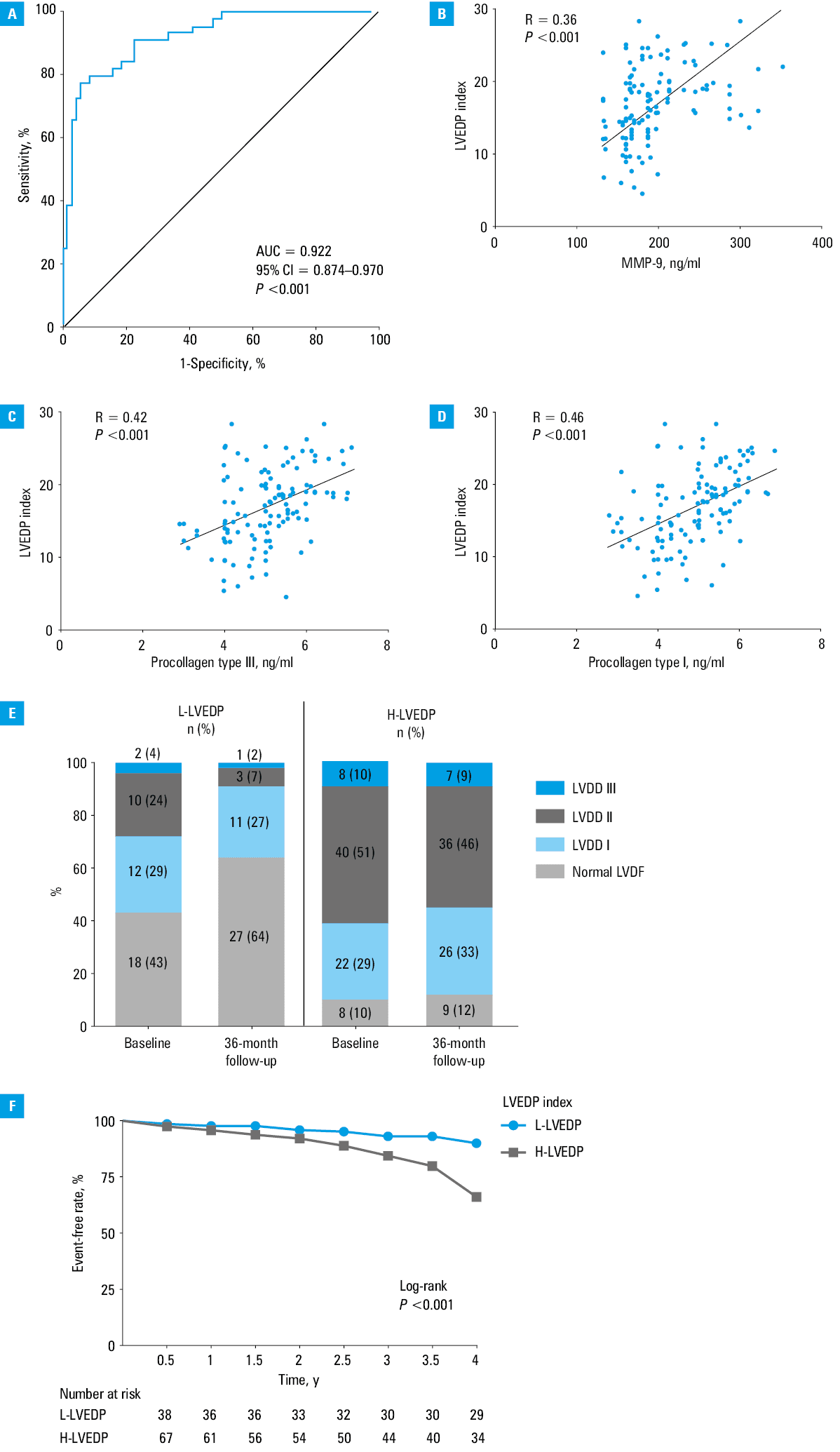
Using the ROC curves, we observed that the AUC of the LVEDP index for predicting LVEDP was 0.922 (95% CI, 0.874–0.970; P <0.001), and the cutoff value was 14.63 (Figure 1A).
Characteristics of the patients
According to the cutoff value of the LVEDP index, the patients were divided into the L‑LVEDP group and the H‑LVEDP group. Based on the clinical and echocardiographic characteristics of all participants, the thickness of the interventricular septal end diastole, LAVI, TRmax, the average ratio of early diastolic mitral velocity to early diastolic mitral annulus velocity (E/e’), A, and E values were higher in the H‑LVEDP group than in the L‑LVEDP group (Supplementary material, Table S4).
Relationship between the left ventricular end‑diastolic pressure index and fibrotic parameters
The LVEDP index positively correlated with the levels of procollagen type I (R = 0.46; P <0.001), procollagen type III (R = 0.42; P <0.001), and MMP‑9 (R = 0.36; P <0.001) (Figure 1B–1D).
Assessment of the prognosis of left ventricular diastolic dysfunction patients
Based on the treatment of primary diseases, we reevaluated the LVDF at the 36 months into the follow‑up. We observed that the proportion of patients with normal LVDF in the L‑LVEDP group was greater than in the H‑LVEDP group, both at baseline and 36 months into the follow‑up. However, the patients in the H‑LVEDP group showed no significant improvement at the 36 months follow‑up (Figure 1E).
During the 4 years of the follow‑up, 57 patients (48%) met the composite primary end point. The patients with abnormal LVEDP index (≥14.63) showed a higher probability of adverse cardiac events and all‑cause mortality than those with lower level of the LVEDP index (<14.63). Notably, the LVEDP index was also significantly associated with an increased risk of the primary end point after multivariable adjustment for the baseline clinical characteristics and echocardiographic parameters (HR = 1.49; 95%CI, 1.33–2.15; P = 0.002) (Figure 1F, Supplementary material, Table S5).
Discussion
LVDD requires frequent hospitalizations and is associated with poor quality of life and all‑cause death.15 Our previous studies have verified the accuracy and reliability of the LVEDP index according to the LVEDP from LV catheterization, which is the gold standard for the evaluation of LVDD. In the present study, we further established that a high LVEDP index could reflect the state of MF, which can contribute to myocardial remodeling in LVDD patients. An elevated level of the LVEDP index could be used as an independent predictor of outcome in LVDD patients.
According to the guidelines issued in 2016 by the American Society of Echocardiography and the European Association of Cardiovascular Imaging, LVDF can be reflected by several echocardiographic parameters, including average E/e’ ratio, mitral E/A ratio, LAVI, and TRmax. The LVEDP index we describe consisted of several echocardiographic parameters and outperformed any single parameter in the evaluation of LVDF. The LVEDP index showed excellent value in predicting the prognosis of LVDD.
According to the cutoff value of the LVEDP index, its higher value was strongly associated with poorer prognosis. It also positively correlated with the levels of fibrosis‑related cytokines, indicating that the LVDD patients with a higher LVEDP index would have a worse outcome. Excessive myocardial collagen deposition leads to high myocardial diastolic stiffness, contributing to LVDD.2 Several echocardiographic parameters, such as PVd and LAVI, have been found to be related to the myocardial diastolic stiffness, and these parameters have also been integrated into the LVEDP index, demonstrating that the index is likely to reflect the myocardial diastolic stiffness. The fact that the LVEDP index has been found to be closely related to the fibrotic parameters suggests that it might reflect the impairment of myocardial diastolic stiffness caused by excessive myocardial collagen deposition. This way, higher LVEDP index indicates exacerbation of MF and irreversible ventricular remodeling.
However, this study was a single‑center one, and the sample size was small. It is necessary to conduct multicenter studies with greater sample size. In conclusion, the LVEDP index could be a suitable marker for the evaluation of the LVDF and better prediction of the prognosis of LVDD patients.
- Lee HJ, Lee H, Kim SM, et al. Diffuse myocardial fibrosis and diastolic function in aortic stenosis. JACC Cardiovasc Imaging. 2020; 13: 2561‑2572. | Crossref
- Hamdani N, Paulus WJ. Myocardial titin and collagen in cardiac diastolic dysfunction: partners in crime. Circulation. 2013; 128: 5‑8. | Crossref
- Ibrahim EH, Dennison J, Frank L, et al. Diastolic cardiac function by MRI‑imaging capabilities and clinical applications. Tomography. 2021; 7: 893‑914. | Crossref
- Pieske B, Tschöpe C, De Boer RA, et al. How to diagnose heart failure with preserved ejection fraction: the HFA‑PEFF diagnostic algorithm: a consensus recommendation from the Heart Failure Association (HFA) of the European Society of Cardiology (ESC). Eur Heart J. 2019; 40: 3297‑3317. | Crossref
- Klein AL, Hatle LK, Taliercio CP, et al. Prognostic significance of Doppler measures of diastolic function in cardiac amyloidosis. A Doppler echocardiography study. Circulation. 1991; 83: 808‑816. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION