Therapeutic challenge: a giant, infiltrating intrathyroidal thymic carcinoma of the thyroid gland



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Therapeutic challenge: a giant, infiltrating intrathyroidal thymic carcinoma of the thyroid gland
A 58‑year‑old man was transferred to an endocrine surgery department due to severe dyspnea caused by a chest tumor that rapidly developed within several weeks. His general condition was poor, with many comorbidities. Computed tomography revealed a large mass in the anterior mediastinum, which was pressing on and displacing the trachea to the right side, causing significant constriction of the respiratory tract (Figure 1A and 1B), but no obvious metastatic lesions or lymph node involvement were found. The laryngological consultation revealed deep left vocal fold paresis with proper mobility of the right side. Percutaneous gastrostomy was performed because of dysphagia. Due to the rapid progression of the disease, the main suspicion was an anaplastic carcinoma. However, core needle biopsy identified intrathyroidal thymic carcinoma (ITC). During an interdisciplinary committee meeting, a decision about surgery was made.
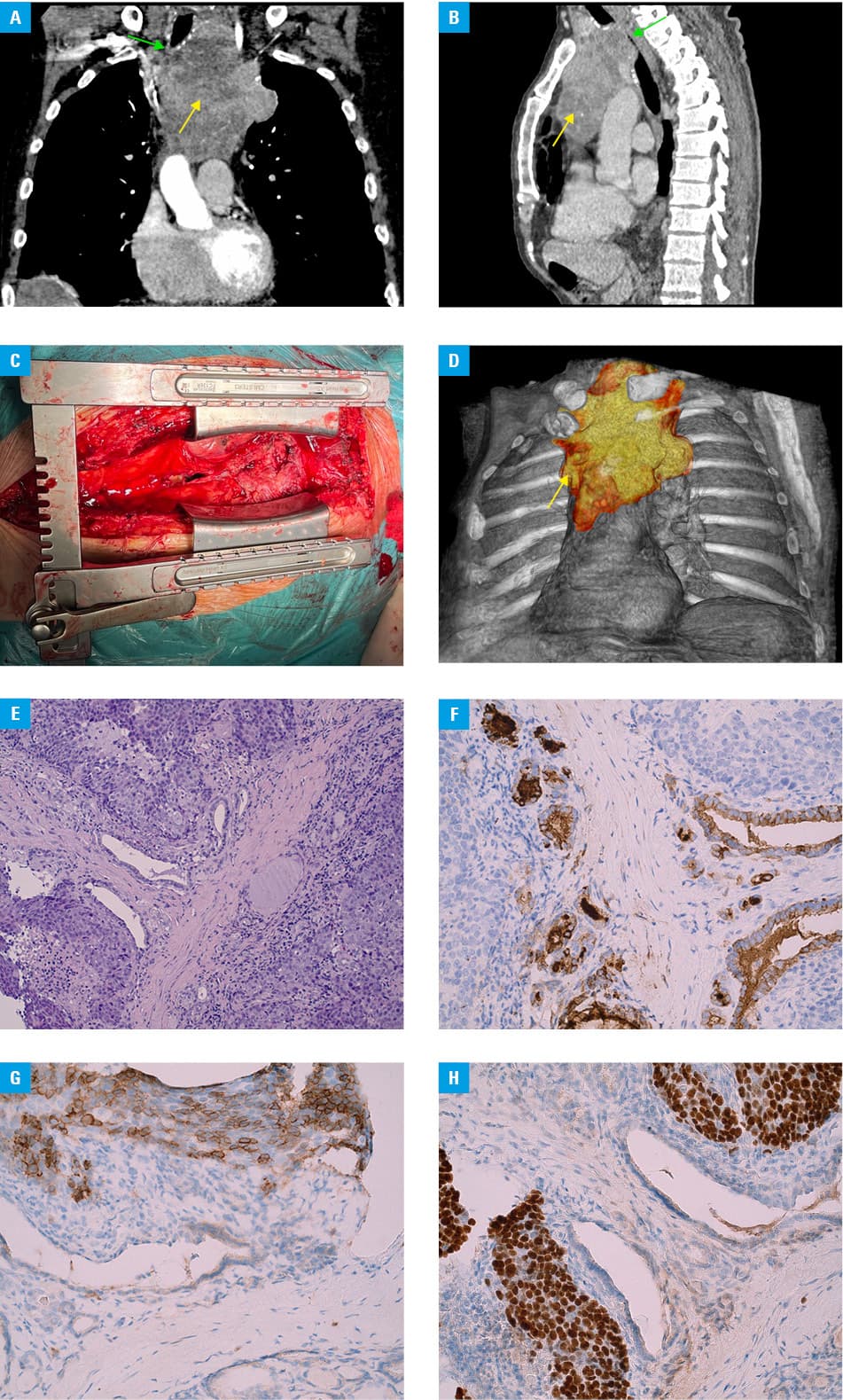
The surgical access to the tumor was made through sternotomy and collar incision (Figure 1C). Intraoperative assessment revealed an invasion of the tumor into the anterior mediastinum, both pleural cavities, the pericardium, and the aorta, including proximal parts of the coronary arteries (Figure 1D). Because of the invasion, a complete surgical removal was deemed impossible, and the procedure was halted. Surgical biopsy of the mass and tracheostomy were performed instead. The specimen was sent for pathologic examination (Figure 1E–1H). Multiple immunohistochemical staining procedures were performed. The tumor showed a positive reaction with the following antibodies: CKAE1/AE3, CK19, p40, CD117, bcl2, and in some cells also CD5 and calretinin, and a negative reaction with TTF‑1, thyroglobulin, PAX8, calcitonin, synaptophysin, chromogranin A, p53 (null), and CEA. The Ki‑67 index was 20%, which finally confirmed ITC.
There were no complications during the postoperative period. The patient was consulted by an oncologist and a radiotherapist, who assessed his condition as Eastern Cooperative Oncology Group score 4, and he was disqualified from radiotherapy and chemotherapy. With the consent of the patient and his family, he was transferred to a hospice.
ITC is a very rare thyroid gland tumor, accounting for less than 0.15% of thyroid neoplasms. Usually, it affects people in their fifth decade of life, with no significant relation to the ethnicity or sex.1,2 It was previously referred to as carcinoma showing thymus‑like differentiation, and classified by the World Health Organization in 2004 as an independent thyroid tumor. Similarly to the other thyroid neoplasms, it is characterized by extensive growth and lobulated pattern, and it is macroscopically indistinguishable from other thyroid tumors.
Proper differentiation of thyroid tumors in this location is crucial, as it has a different prognosis and treatment strategy than other advanced thyroid tumors,1 such as anaplastic cancer or undifferentiated thyroid cancer. Even though the surgery is a cornerstone of the ITC treatment,3,4 as it is typically of an indolent nature with a relatively good prognosis, in our patient’s case surgical removal was not a viable option due to the rapid advancement of the disease.
Unfortunately, similarly to anaplastic cancers, ensuring the patency of the respiratory and gastrointestinal tracts in patients with advanced, inoperative tumors is still challenging.5 The final decision should depend on the consensus of an interdisciplinary board, previous experiences, and individual patient preferences.
- Gurizzan C, Zamparini M, Volante M, et al. Outcome of patients with intrathyroidal thymic carcinoma: a pooled analysis. Endocr Relat Cancer. 2021; 28: 593‑604. | Crossref
- Sun YH, Xu J, Li M. Intrathyroid thymic carcinoma: report of two cases with pathologic and immunohistochemical studies. Int J Clin Exp Pathol. 2018; 11: 5139‑5143.
- Le QV, Nguyen HV, Mai NTK, Nguyen HX. Surgical treatment result of giant thyroid tumor: case series in Vietnam. Int J Surg Case Rep. 2019; 54: 103‑107. | Crossref
- Ge W, Yao YZ, Chen G, Ding YT. Clinical analysis of 82 cases of carcinoma showing thymus‑like differentiation of the thyroid. Oncol Lett. 2016; 11: 1321‑1326. | Crossref
- Bible KC, Kebebew E, Brierley J, et al. 2021 American Thyroid Association Guidelines for Management of Patients with Anaplastic Thyroid Cancer: American Thyroid Association Anaplastic Thyroid Cancer Guidelines Task Force. Thyroid. 2021; 31: 337‑386. | Crossref
ARTICLE INFORMATION