Influence of smoking on disease activity and prognosis of antineutrophil cytoplasmic antibody–associated vasculitis: a retrospective cohort study
Key words: antineutrophil cytoplasmic antibody–associated vasculitis, environmental factors, granulomatosis with polyangiitis, microscopic polyangiitis, smoking



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Influence of smoking on disease activity and prognosis of antineutrophil cytoplasmic antibody–associated vasculitis: a retrospective cohort study
Introduction: Antineutrophil cytoplasmic antibody–associated vasculitides (AAV) are a group of autoimmune diseases characterized by inflammation of small blood vessels. Smoking is a potential trigger for such diseases, however, its link with AAV remains controversial.
Objectives: The aim of this study was to analyze the link between AAV and smoking based on clinical characteristics, disease activity, and mortality.
Patients and methods: This retrospective study included 223 AAV patients. Their smoking status was assessed at diagnosis and they were classified as ever smokers (ESs), including current or past smokers, and never smokers (NSs). Information regarding clinical presentation, the disease activity, immunosuppressive therapy, and survival was collected.
Results: The ESs had similar organ involvement to the NSs, except for significantly greater frequency of renal replacement therapy (31% vs 14%; P = 0.003). Median (interquartile range [IQR]) time from symptom onset to diagnosis was significantly shorter in the ESs than the NSs (4 [2–9.5] vs 6 [3–13] months; P = 0.03), with significantly higher mean (SD) value of the Birmingham Vasculitis Activity Score version 3 (19.5 [7.93] vs 17.25 [8.05]; P = 0.04). The ESs were more likely to receive cyclophosphamide therapy (P = 0.03), and had significantly higher morality than the NSs (hazard ratio, 2.89; 95% CI, 1.47–5.72; P = 0.002). There were no significant differences between the current and past smokers. The multivariable Cox proportional regression analysis found ever smoking and male sex to be independent predictors of mortality in AAV patients.
Conclusions: Ever smoking is associated with increased AAV activity and more frequent renal replacement therapy and immunosuppressive treatment, resulting in a poorer survival prognosis in AAV patients. Future multicenter studies are required to further characterize the clinical, biological, and prognostic impact of smoking on AAV.
What's new?
There is limited evidence on the link between antineutrophil cytoplasmic antibody–associated vasculitides (AAV) and smoking, especially on the impact of smoking on the disease activity and prognosis. This retrospective cohort study of 223 AAV patients (granulomatosis with polyangiitis or microscopic polyangiitis) demonstrated that ever smoking (current as well as past smokers) correlated with a significantly greater disease activity at diagnosis, greater need for renal replacement therapy, and poorer overall survival than never smoking. In a multivariable analysis, ever smoking and male sex were found to be independent factors associated with mortality in AAV patients. This provides better insights into the impact of smoking as an environmental trigger for AAV, and highlights the need for further research into this link.
Introduction
Antineutrophil cytoplasmic antibody (ANCA)-associated vasculitides (AAV) are a group of diseases characterized by necrotizing inflammation of small vessels that leads to damage and dysfunction of the supplied organs.1 They are associated with the presence of specific antibodies against proteinase 3 (PR3) or myeloperoxidase (MPO). As AAV predominantly involve small vessels (arteries, arterioles, venules, and veins), any organ of the body can be affected. These vasculitides typically involve the upper respiratory tract, lungs, and kidneys, but skin, nervous system, gastrointestinal tract, and eye may also be affected. Although the pathogenesis of AAV is not completely understood, it is thought to be multifactorial. Previous studies have suggested that it starts with an initial exposure to infectious agents, or is due to genetic or environmental factors followed by inflammatory response and increased ANCA formation.2
Smoking is one of the environmental factors that has been linked to the development of certain autoimmune diseases (AIDs). Studies suggest that smoking triggers autoantibody formation or functions as a “second hit” promoting the disease development.3 There is sufficient evidence highlighting an association of smoking with AIDs, such as rheumatoid arthritis (RA), multiple sclerosis, systemic lupus erythematosus (SLE), Graves thyroiditis, and giant cell arteritis.3-6 These findings are not limited to active smokers, as similar links with passive smoking have also been observed. Hammam et al7 found out that RA activity was significantly higher in passive smokers than in nonsmokers. Wang et al8 suggested that higher incidence of multiple sclerosis in women and children could be traced back to passive smoking, with the duration of exposure significantly influencing the risk. Although data linking smoking with the abovementioned diseases are conclusive, there are several diseases in which the effect of smoking remains controversial. Some studies on Bechet disease describe an improvement in oral and genital ulcers among smokers, while others report that smoking paired with HLA‑B51 positivity could worsen neurologic manifestations.3
Studies on smoking and AAV, however, are limited and present contradictory evidence. A previous study suggested that although the disease activity is higher in ever smokers (ESs) than in never smokers (NSs), smoking may not be a significant risk factor for AAV.9 Additionally, Haubitz et al10 has suggested that a reduced risk of AAV in smokers is potentially due to the protective role of nicotine via inhibition of immune mechanisms. On the contrary, another study associated smoking with a higher risk of AAV.11 Some data also suggest that smoking influences clinical manifestations and organ involvement in AAV patients, with upper respiratory damage being significantly less prevalent in smokers.12 Moreover, the impact of smoking on the prognosis and survival of AAV patients is yet to be studied.
This study aimed to compare AAV patients with regard to their smoking status based on clinical characteristics and the disease activity. Secondarily, it examined the impact of smoking on mortality in AAV patients.
Patients and methods
Study design
The retrospective cohort analysis included 252 patients with AAV treated in tertiary referral specialist clinics at the Medical University of Gdansk, Poland, from October 1988 to August 2020. Of those, 223 patients (46% women) diagnosed with AAV were included in the study. The remaining 29 patients were excluded from the analysis due to the lack of data regarding their smoking status. All patients met the European Medicines Agency vasculitis classification criteria13 for granulomatosis with polyangiitis (GPA) or microscopic polyangiitis. The GPA patients fulfilled also the 1990 American College of Rheumatology criteria and the Revised International Chapel Hill Consensus criteria (2012)14. Smoking meant cigarette smoking in most cases, however, medical records did not differentiate cigarette smoking from cigar or pipe smoking. The smoking status was determined based on the patient’s declaration in medical records. The patients were categorized as either current smokers, past smokers (patient‑reported being a smoker in the past), or NSs at AAV diagnosis. Due to the retrospective nature of the study, it was not possible to quantify the pack‑years or duration of smoking for sufficient number of patients. The study was conducted in accordance with the ethical standards for research involving humans, as set by the 1964 Declaration of Helsinki and its amendments. Due to its retrospective nature, a bioethics committee approval was not required.
Data collection
The patient medical records and outpatient follow‑up charts were retrieved and reviewed for relevant data pertaining to their demographic features, clinical presentation and progression, laboratory findings, treatment, and outcomes. The specific manifestations of the following organ involvement were retrieved: renal, ear, nose, throat (ENT), pulmonary, constitutional symptoms, central nervous system, dermatological, gastrointestinal, ophthalmologic, and cardiac. The disease staging was assessed according to the European Vasculitis Society guidelines15 as “limited” with upper and / or lower respiratory tract disease without any other systemic involvement or constitutional symptoms; “early systemic” without any organ involvement or life‑threatening disease; “systemic” with kidney- or other organ‑threatening disease, serum creatinine level below 500 μmol/l (5.6 mg/dl); or “severe” with kidney or other vital organ failure, serum creatinine above 500 μmol/l.12 Vasculitis activity was calculated using the Birmingham Vasculitis Activity Score version 3 (BVASv3),16 while the Disease Extent Index (DEI) was used to assess the disease severity.17 The usage of immunosuppressive therapy (cyclophosphamide) in terms of a total dose, cumulative intravenous and oral doses was also recorded. The follow‑up end points were the status of the patient at the end of the data collection (August 2020), attrition before the final date, or death. In addition, information regarding the cause of death prior to the final date was retrieved.
Statistical analysis
The Shapiro–Wilk test was applied to assess the normality of distribution. The χ2 test or the Fisher exact test was used for comparison of categorical variables. The analysis of normally distributed continuous variables was performed with the Mann–Whitney test and reported as medians and interquartile ranges (IQRs). For non‑normally distributed data, the unpaired t test was used, and the results were reported as means and SD. Comparisons were considered significant if a 2‑tailed P value was below 0.05. We performed 2 sets of comparisons: 1) NSs vs ESs (including current and past smokers), and 2) current smokers vs past smokers. The Kaplan–Meier analysis was carried out to compare the survival between these groups. The period of survival was calculated in months from the date of diagnosis until the month of data collection, death, or the last information for each patient. In order to identify factors associated with survival, the multivariable Cox proportional hazard regression analysis was carried out, including explanatory variables that were statistically significant (P <0.05) in the univariable analysis. Statistical analysis was performed with GraphPad Prism 8.0 package (GraphPad Prism Software Inc., San Diego, California, United States).
Results
The study cohort included 116 NS patients and 107 ESs (including 39 current smokers and 68 past smokers). The mean (SD) age of our cohort at diagnosis was 53.3 (15.79) years.
Ever vs never smokers
The baseline characteristics and clinical manifestations for the ESs and the NSs are listed in Table 1. There were significantly more men in the ES than the NS group (71% vs 39%; P <0.001). The groups did not differ significantly in terms of age at diagnosis.
Parameter | Ever smokers (n = 107) | Never smokers (n = 116) | P value | Current smokers (n = 39) | Past smokers (n = 68) | P value | ||
a Central nervous system involvement including meningitis, spinal cord injury, stroke, lymphatic involvement
Abbreviations: CNS, central nervous system; ENT, ear, nose, throat; RRT, renal replacement therapy | ||||||||
Sex, n (%) | Men | 76 (71) | 45 (39) | <0.001 | 33 (85) | 43 (63) | 0.03 | |
Women | 31 (29) | 71 (61) | 6 (15) | 25 (37) | ||||
Age at diagnosis, y, mean (SD) | 55.14 (14.79) | 51.6 (16.55) | 0.09 | 50.56 (13.41) | 57.76 (14.99) | 0.02 | ||
Clinical manifestations, n (%) | ||||||||
Renal involvement | Involvement at diagnosis | 77 (72) | 70 (60) | 0.09 | 29 (74) | 48 (71) | 0.82 | |
Kidney failure at diagnosis | 59 (55) | 54 (47) | 0.23 | 23 (59) | 36 (53) | 0.69 | ||
Proteinuria | 66 (62) | 62 (54) | 0.23 | 25 (64) | 41 (60) | 0.84 | ||
Hematuria | 74 (69) | 69 (59) | 0.16 | 28 (72) | 46 (68) | 0.83 | ||
Need for RRT at diagnosis | 34 (31) | 17 (14) | 0.003 | 10 (26) | 24 (35) | 0.39 | ||
ENT involvement | ENT changes at diagnosis | 64 (60) | 79 (68) | 0.21 | 23 (59) | 41 (60) | 0.99 | |
Nose | 45 (42) | 56 (48) | 0.42 | 16 (41) | 29 (43) | 0.99 | ||
Throat | 4 (4) | 10 (9) | 0.17 | 1 (3) | 3 (34) | 0.99 | ||
Larynx | 10 (9) | 12 (10) | 0.83 | 3 (8) | 7 (10) | 0.74 | ||
Sinus | 38 (36) | 50 (43) | 0.27 | 12 (31) | 26 (38) | 0.53 | ||
Salivary glands | 0 | 3 (3) | 0.25 | 0 | 0 | 0.99 | ||
Ear | 30 (28) | 29 (25) | 0.65 | 9 (23) | 21 (31) | 0.50 | ||
Mouth | 11 (10) | 12 (10) | 0.99 | 5 (13) | 6 (9) | 0.53 | ||
Pulmonary involvement | Involvement during the disease | 72 (67) | 71 (61) | 0.4 | 28 (72) | 44 (65) | 0.52 | |
Cough | 59 (55) | 54 (47) | 0.23 | 24 (62) | 35 (51) | 0.42 | ||
Dyspnea | 45 (42) | 38 (33) | 0.17 | 19 (49) | 26 (38) | 0.32 | ||
Pleural fluid | 13 (12) | 7 (6) | 0.16 | 6 (15) | 7 (10) | 0.54 | ||
Intravesical bleeding / hemoptysis | 31 (29) | 21 (18) | 0.06 | 12 (31) | 19 (28) | 0.83 | ||
Respiratory failure | 10 (9) | 9 (8) | 0.81 | 2 (5) | 8 (12) | 0.32 | ||
Nodular / infiltrative lesions (on imaging) | 47 (44) | 43 (37) | 0.34 | 21 (54) | 26 (38) | 0.16 | ||
Interstitial lesions (on imaging) | 38 (36) | 45 (39) | 0.68 | 14 (36) | 24 (35) | 0.99 | ||
Bronchial distress / narrowing | 11 (10) | 7 (6) | 0.33 | 3 (8) | 8 (12) | 0.74 | ||
Constitutional symptoms | Joint involvement | 55 (51) | 68 (59) | 0.29 | 20 (51) | 35 (51) | 0.99 | |
Fever | 61 (57) | 67 (58) | 0.99 | 24 (62) | 37 (54) | 0.55 | ||
Loss of weight | 47 (44) | 47 (41) | 0.68 | 20 (51) | 27 (40) | 0.31 | ||
CNS involvement | Peripheral neuropathy at diagnosis | 14 (13) | 17 (15) | 0.85 | 6 (15) | 8 (12) | 0.77 | |
CNSa | 14 (13) | 12 (10) | 0.54 | 3 (8) | 11 (16) | 0.25 | ||
CNS disease (in general) | 15 (14) | 8 (7) | 0.12 | 4 (10) | 11 (16) | 0.57 | ||
Dermatological involvement | Purpura | 32 (30) | 23 (20) | 0.09 | 10 (26) | 22 (32) | 0.52 | |
Skin ulceration / necrosis / other | 23 (21) | 19 (16) | 0.39 | 9 (23) | 14 (21) | 0.81 | ||
Gastrointestinal involvement | 13 (12) | 9 (8) | 0.37 | 6 (15) | 7 (10) | 0.81 | ||
Ophthalmologic involvement | 26 (24) | 32 (28) | 0.65 | 9 (23) | 17 (25) | 0.57 | ||
Cardiac involvement | 3 (3) | 5 (4) | 0.72 | 2 (5) | 1 (1) | 0.55 | ||
The groups differed only in the need for renal replacement therapy (RRT) at diagnosis (31% vs 14%; P = 0.003), with the ESs requiring RRT more often than the NSs. The groups had similar frequency of other organ involvement and symptoms.
The details related to the disease activity, relapses, laboratory findings, and ANCA positivity are presented in Table 2. The median (IQR) time from the onset of symptoms to AAV diagnosis was significantly shorter in the ESs than the NSs (4 [2–9.5] vs 6 [3–13] months; P = 0.03). The disease activity assessed as mean BVASv3 was significantly higher in the ESs than in the NSs (19 [7.93] vs 17.25 [8.05]; P = 0.04). However, the DEI and the disease stage at onset did not differ significantly between the groups. Both groups had a similar number of relapses and the time from diagnosis to the first relapse. The groups were also similar in terms of laboratory abnormalities and inflammatory parameters. However, the ESs had a significantly higher median C‑reactive protein level than the NSs (P = 0.01). There was no difference in the positivity of cytoplasmic ANCA, PR3‑ANCA, perinuclear ANCA, and MPO‑ANCA between the groups.
Parameter | Ever smokers (n = 107) | Never smokers (n = 116) | P value | Current smokers (n = 39) | Past smokers (n = 68) | P value | |
Abbreviations: BVASv3, Birmingham Vasculitis Activity Score version 3; cANCA, cytoplasmic antineutrophil cytoplasmic antibody; CRP, C‑reactive protein; DEI, disease extent index; ESR, erythrocyte sedimentation rate; Hb, hemoglobin; IQR, interquartile range; MPO, myeloperoxidase; pANCA, perinuclear antineutrophil cytoplasmic antibody; PR3, proteinase 3 | |||||||
Time from symptom onset to diagnosis, mo, median (IQR) | 4 (2–9.5) | 6 (3–13) | 0.03 | 3.5 (2–6.5) | 4 (2–12) | 0.34 | |
BVASv3 at diagnosis, mean (SD) | 19.5 (7.93) | 17.25 (8.05) | 0.04 | 20.62 (9.21) | 18.87 (7.09) | 0.28 | |
DEI, mean (SD) | 6.79 (2.62) | 6.96 (2.86) | 0.64 | 7.1 (2.47) | 6.6 (2.72) | 0.34 | |
Disease onset form, n (%) | Limited | 7 (7) | 16 (14) | 0.15 | 2 (5) | 5 (7) | 0.83 |
Early systemic | 37 (35) | 40 (34) | – | 12 (31) | 25 (37) | – | |
Systemic | 32 (30) | 38 (33) | – | 12 (31) | 20 (29) | – | |
Severe | 31 (29) | 22 (19) | – | 13 (33) | 18 (26) | – | |
Relapses, n (%) | 0 | 58 (54) | 62 (53) | 0.97 | 23 (59) | 35 (51) | 0.53 |
1–2 | 36 (34) | 37 (32) | – | 13 (33) | 23 (34) | – | |
>3 | 13 (12) | 15 (13) | – | 3 (8) | 10 (14) | – | |
Missing data | – | 2 (2) | – | – | – | – | |
Time from diagnosis to first relapse, mo, median (IQR) | 24 (10–35.75) | 23 (12–36) | 0.85 | 24 (13–34) | 22 (9.5–36) | 0.67 | |
Patients under observation, n (%) | Yes | 62 (58) | 12 (10) | <0.001 | 24 (62) | 38 (56) | 0.83 |
No | 20 (19) | 94 (81) | – | 7 (18) | 13 (19) | – | |
Deceased | 25 (23) | 10 (9) | – | 8 (21) | 17 (25) | – | |
Anemia at onset (Hb; women <12 g/dl; men <13.5 g/dl), n (%) | Yes | 83 (78) | 77 (66) | 0.16 | 31 (79) | 52 (76) | 0.8 |
No | 21 (20) | 31 (27) | – | 7 (18) | 14 (21) | – | |
Not performed | 3 (3) | 8 (7) | – | 1 (3) | 2 (3) | – | |
Leukocytosis, >10 000/μl, n (%) | Yes | 47 (44) | 42 (36) | 0.48 | 19 (49) | 28 (41) | 0.53 |
No | 52 (49) | 59 (51) | – | 17 (44) | 35 (41) | – | |
Not performed | 8 (7) | 15 (13) | – | 3 (8) | 5 (7) | – | |
Thrombocytosis, >400 G/l, n (%) | Yes | 41 (38) | 33 (28) | 0.15 | 17 (44) | 24 (35) | 0.29 |
No | 58 (54) | 72 (62) | – | 18 (46) | 40 (59) | – | |
Not performed | 8 (7) | 11 (9) | – | 4 (10) | 4 (6) | – | |
CRP, mg/l, median (IQR) | 86 (30–161) | 63.5 (16.2–113.5) | 0.01 | 105 (45–203) | 79 (28.5–151) | 0.13 | |
ESR, mm/h, median (IQR) | 64 (39–95) | 62.5 (29.75–104.3) | 0.79 | 76 (40.75–120) | 58 (37–87) | 0.11 | |
cANCA positive, n (%) | 66 (62) | 69 (59) | 0.57 | 23 (59) | 43 (63) | 0.83 | |
PR3‑ANCA positive, n (%) | 56 (52) | 69 (59) | 0.89 | 20 (51) | 36 (53) | 0.67 | |
pANCA positive, n (%) | 33 (31) | 33 (28) | 0.77 | 11 (28) | 22 (32) | >0.99 | |
MPO‑ANCA positive, n (%) | 26 (24) | 29 (25) | >0.99 | 8 (21) | 18 (26) | 0.63 | |
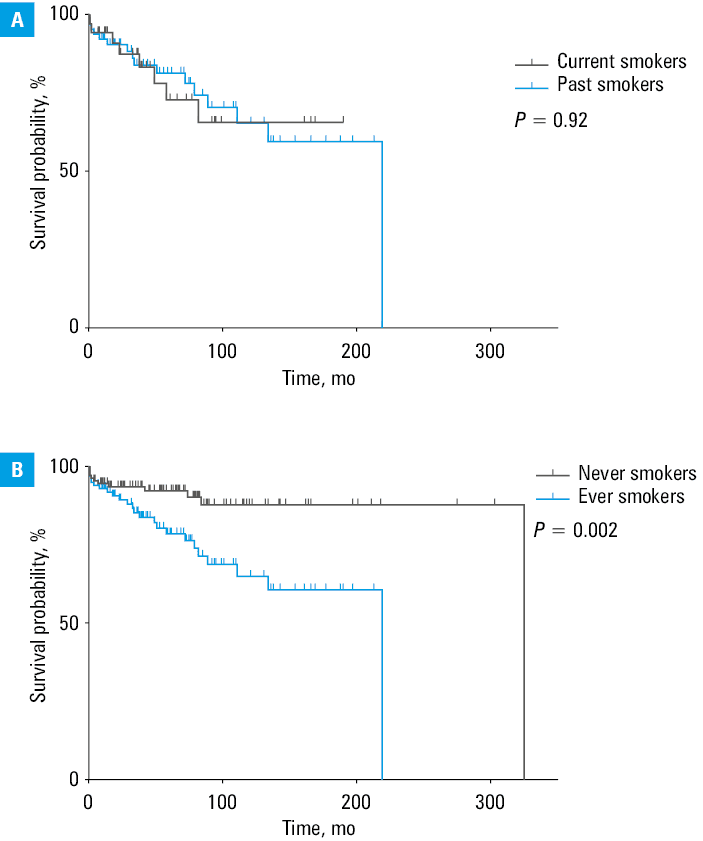
The information regarding treatment regimen, follow‑up period, and mortality is provided in Table 3. Immunosuppressive treatment did not differ between the groups, but more ESs than NSs received cyclophosphamide (92% vs 81%; P = 0.03). Both groups had similar follow‑up duration. In our cohort, the mortality was significantly higher for the ESs than the NSs (23% vs 9%; P <0.001). In the Kaplan–Meier analysis, the ESs were found to have significantly greater mortality hazard (hazard ratio [HR], 2.89; 95% CI, 1.47–5.72; P = 0.002) (Figure 1A). There was no significant difference in terms of the cause of death between the 2 groups. In the multivariable Cox proportional hazard regression analysis, smoking status (ever smoking) (HR, 2.39; 95% CI, 1.11–5.54; P = 0.03) and male sex (HR, 0.67; 95% CI, 0.31–1.45; P = 0.01) were found to be independent predictors of mortality in AAV patients (Table 4).
Parameter | Ever smokers (n = 107) | Never smokers (n = 116) | P value | Current smokers (n = 39) | Past smokers (n = 68) | P value | |
a Two outliers removed in current smokers (diagnosed in 1988 and 1998, PO doses 120 and 168, respectively)
Abbreviations: AAV, ANCA‑associated vasculitis; IV, intravenous; PO, per os; others, see Table 2 | |||||||
Patients treated with cyclophosphamide, n (%) | Total | 98 (92) | 94 (81) | 0.03 | 37 (95) | 61 (90) | 0.48 |
IV administration | 90 (84) | 86 (74) | 0.07 | 33 (85) | 57 (84) | >0.99 | |
PO administration | 19 (18) | 14 (12) | 0.26 | 8 (21) | 11 (16) | 0.61 | |
Cyclophosphamide doses, g, median (IQR) | Total dose | 7.4 (5.6–13.2) | 7.5 (4.8–11.3) | 0.37 | 8.69 (6.5–14.5) | 7.1 (5.5–12.8) | 0.27 |
Cumulative IV dose | 6.95 (5.2–9.4) | 7.1 (4.5–9.1) | 0.62 | 7.1 (5–8.9) | 6.6 (5.4–10.4) | 0.76 | |
Cumulative PO dose | 20 (9–50) | 23.3 (9.8–63.5) | 0.87 | 21.5 (15.75–55)a | 18 (6–36) | 0.32 | |
Follow‑up period, mo, median (IQR) | 43.5 (1892) | 63 (24.8–103) | 0.18 | 41.5 (18–82) | 46.5 (17.5–102.8) | 0.81 | |
Mortality | Yes | 25 (23) | 11 (9) | 0.006 | 8 (21) | 17 (25) | 0.81 |
No | 81 (76) | 105 (91) | – | 30 (77) | 51 (75) | – | |
Missing data | 1 (1) | – | – | 1 (3) | – | – | |
Mortality, hazard ratio (95% CI) | 2.89 (1.47–5.72) | reference | 0.002 | 1.04 (0.44–2.49) | reference | 0.92 | |
Cause of death, n (%) | AAV‑related | 13 (52) | 6 (55) | >0.99 | 4 (50) | 9 (50) | >0.99 |
Other causes | 9 (36) | 5 (45) | – | 3 (38) | 6 (35) | – | |
No cause reported | 3 (12) | 0 | – | 1 (13) | 2 (12) | – | |
Variable | Hazard ratio | 95% CI | P value | ||
Sex | Women | 1 (ref) | 1 (ref) | 1 (ref) | |
Men | 0.67 | 0.31–1.45 | 0.29 | ||
Age at diagnosis | 1.04 | 1.01–1.08 | 0.01 | ||
Smoking status | Never | 1 (ref) | 1 (ref) | 1 (ref) | |
Ever | 2.39 | 1.11–5.54 | 0.03 | ||
Need for RRT | No | 1 (ref) | 1 (ref) | 1 (ref) | |
Yes | 1.54 | 0.7–3.32 | 0.27 | ||
Time from symptom onset to diagnosis | 1 (ref) | 0.97–1.02 | 0.89 | ||
BVASv3 | 1.07 | 0.99–1.14 | 0.05 | ||
DEI | 1.03 | 0.85–1.25 | 0.74 | ||
In the subgroup analysis, the ES men were found to have significantly greater need for RRT (36% vs 18%; P = 0.04) and lower sinus involvement (30% vs 53%; P = 0.02) than the NS men (Supplementary material, Table S1). Mortality was also significantly greater in the ES men than the NS men (22% vs 4%; P = 0.009). There were no differences in terms of renal and ENT involvement, and mortality in the EN and the NS women (Supplementary material, Table S1).
Current vs past smokers
To further unravel the influence of smoking on AAV, the current smokers were compared with past smokers. The baseline characteristics of these patients are reported in Table 1. There were significantly more men who were current smokers than past smokers (85% vs 62%; P = 0.03). The current smokers were significantly younger at diagnosis than the past smokers (mean [SD], 57.76 [14.99] vs 50.56 [13.41] years; P = 0.02).
The groups had similar frequencies of various clinical manifestations and organ involvement (Table 1). The period between the symptom onset and AAV diagnosis was similar in both groups. The disease activity also did not differ between the current and past smokers as demonstrated by the BVASv3 score, and the DEI and disease onset forms were similar. The groups also experienced similar number of relapses and similar time to the first relapse (Table 2). No significant variations in terms of complete blood count, inflammatory parameters, and ANCA positivity were observed among the current and past smokers (Table 2). The need for and cumulative dose of cyclophosphamide also did not differ between the 2 groups (Table 3). The number of deaths and mortality hazard were also similar in the current and past smokers (Table 3, Figure 1B).
Discussion
This retrospective analysis of AAV patients treated at a single Polish institution found that smoking is associated with younger age and greater disease activity at diagnosis and poorer survival. The smoking status did not influence clinical manifestations of AAV, except for the need for RRT, which was significantly higher in the smokers. The mortality hazard in our cohort was approximately 3 times greater in the ESs than in the NSs. These differences were not confirmed between current and past smokers, suggesting that smoking at any point in life predicts advanced disease and worse prognosis of AAV.
Previous studies have primarily focused on determining whether smoking is a risk factor for systemic vasculitis. Tobacco smoking induces several deleterious mechanisms with immunomodulatory effects leading to increased production and hyperresponsiveness of B/T cells, augmentation of autoreactive B cells, and suppression of T regulatory cells.18,19 Such effects result in autoantibody formation and elevated levels of proinflammatory mediators. Additionally, smoking‑induced tissue hypoxia and toxin‑mediated cellular necrosis intensify the release of intracellular antigens and overburden the scavenging capacity of the immune system. Based on these pathomechanisms, smoking is suspected to have a significant clinical and prognostic impact on AIDs. Several studies have demonstrated that smokers have higher levels of autoantibodies, such as anti–citrullinated peptide antibodies, anti–double stranded DNA antibodies, and anti–red blood cell antibodies, which are associated with AIDs, such as RA, SLE, and autoimmune hemolytic anemia.20-22 However, PR3/MPO‑ANCA positivity associated with AAV appears to be similar in smokers and nonsmokers, as evidenced by our results and 3 earlier studies.11,23-25 On the contrary, Benarous et al24 found that MPO‑positivity was lower in smokers than nonsmokers. These findings may again suggest smoking as a risk factor for AAV via the mechanism of autoantibody generation. Furthermore, several case‑control studies have failed to show an increased risk of AAV among smokers. Khabbazi et al,9 who investigated 126 primary systemic vasculitis (PSV) patients matched with 210 controls, found that ESs did not have a greater risk of developing PSV. Similarly, Lane et al,26 who examined environmental exposures associated with PSV, did not find any significant variations in the smoking status between their patients and controls. Haubitz et al10 suggested that smoking decreased the risk of AAV primarily because the prevalence of smoking was significantly lower in their cohort at diagnosis than in the general German population. On the other hand, recent data from a large United States‑based case‑control study revealed that AAV patients, especially those MPO‑positive, were more likely to be former or current smokers.11 There is no conclusive evidence whether smoking increases AAV risk, however, smoking‑induced harmful effects may adversely affect severity and prognosis of AAV.
Chronic exposure to tobacco smoke generates a proinflammatory environment via cytokine production (tumor necrosis factor α, interleukin [IL]-1, IL‑6, and IL‑8), and increasing circulating neutrophils, while simultaneously suppressing anti‑inflammatory cytokines, such as IL‑10.27 Smoking also increases oxidative stress and endothelial dysfunction, which leads to generalized vascular injury, and may contribute to the progression of vasculitis.28 Through such an environment, smoking might result in greater disease activity characterized by, as observed in our study, younger age and higher BVASv3 score at diagnosis, and shorter period from the symptom onset to diagnosis. However, the clinical expression of the disease did not differ between the smokers and nonsmokers. The most commonly involved organ systems in either group were the renal, ENT, and pulmonary systems. The only difference identified was the frequency of RRT (for end‑stage kidney disease [ESKD]), which was significantly greater in smokers at diagnosis. In addition to the abovementioned detrimental pathophysiological mechanisms resulting from smoking, it is also evidenced that smoking is a nephrotoxic factor. It accelerates renal tissue damage and fibrosis via increasing the levels of molecular fibrosis markers, suppressing antifibrosis factors, activating growth factors (angiotensin‑II, endothelin‑1), negatively affecting lipoprotein metabolism, and inducing insulin resistance.29,30 Moreover, nicotine has been identified as a promotor of mesangial proliferation and extracellular matrix production.31 These processes cause progressive fibrosis of the renal tissue resulting in kidney function decline and development of chronic kidney disease (CKD). A recent meta‑analysis found smoking to be an independent risk factor for CKD, with a dose‑dependent, cause‑effect relationship.32 A retrospective Korean cohort study showed that current and past smokers had a significantly greater risk of developing ESKD than nonsmokers.32 Such findings indicate a close relationship between smoking and renal function deterioration.
In line with our results, Mohammad et al12 found that ESKD developed more frequently in smoking than nonsmoking PSV patients. In a retrospective analysis of 122 AAV patients, Yamaguchi et al23 also showed that smokers had significantly higher serum creatinine concentration and more often needed RRT than nonsmokers. Additionally, smokers were found to have a significantly higher risk of a relapse in comparison with nonsmokers (P = 0.003), with kidney involvement cited as the most common symptom during the relapse. Although their results regarding ESKD are in agreement with ours, we did not find any association between smoking status and relapse. On the contrary, Haubitz et al10 reported that smoking did not affect the frequency of clinical manifestations, ESKD, relapse rate, or mortality in their cohort. Khabbazi et al9 also did not identify any variations in organ involvement between smokers and nonsmokers. However, similarly to our findings, the BVAS score of smokers at diagnosis was significantly greater in their cohort as compared with nonsmokers. On the other hand, Benarous et al24 suggested that smoking might differentially affect various AAV manifestations, with current smokers presenting with a significantly lower BVAS score and less frequently suffering from peripheral neuropathy. In a subgroup analysis, smokers with GPA were found to have more frequent skin involvement and similar BVAS scores than nonsmokers. However, that analysis only included 76 current smokers compared with 1089 current nonsmokers, which might have influenced these findings. In addition, the majority of the studies10,23,24 reported that smokers with AAV were significantly younger and more often men than in the case of nonsmokers, as also evidenced in our report. Although it seems reasonable to associate smoking‑induced inflammation and vascular injury with greater disease activity and ESKD frequency in AAV patients, there is a minor heterogeneity in the current evidence. Possible explanations could include differences in ethnicity of the studied cohorts, exposure to other risk factors, proportion of AAV phenotypes, and treatment.
Study strengths and limitations
A strong point of our study is the analysis of frequency and dose of cyclophosphamide therapy among smokers and nonsmokers. While no differences in the total, cumulative intravenous and oral doses were observed based on the smoking status, we found that the ESs required immunosuppressive therapy more frequently than the NSs. This may further suggest that the severity of the disease increases significantly with exposure to tobacco smoke, as cyclophosphamide therapy is introduced if organ- or life‑threatening disease occurs.33 The more widespread use of this therapy, effective in over 90% of AAV patients, in smokers, along with the hypothesized lower AAV severity in nonsmokers might explain the similar relapse rates in our groups, contrary to the findings of Yamaguchi et al.23 This further supports our explanation of interstudy discrepancies regarding smoking effect on clinical features of AAV. Another novel finding of our study is the significantly greater mortality hazard in smokers than in nonsmokers. Therefore, it is vital to introduce smoking cessation counselling and to offer smoking cessation agents to AAV patients at diagnosis in order to optimize their management and outcomes.34
Our study is limited by the lack of quantitative data on smoking exposure (pack‑years, smoking cessation years, etc.), which additionally was based on patient self‑reporting during the primary admission. Due to the retrospective nature of our analysis, only an association between smoking and AAV severity and prognosis can be established, rather than a cause‑effect relationship. However, our study is the first to present an in‑depth assessment of clinical manifestations and treatment regimens, and to identify a considerably poor prognosis of AAV in the smokers, especially in the Polish population. These findings are especially relevant due to limited and controversial evidence on the effect of smoking on AAV.
Conclusions
In summary, our findings suggest that smoking significantly increases AAV activity at onset and the need for RRT and immunosuppressive treatment, eventually resulting in a poorer survival prognosis in AAV patients. Smoking at any point in life (ES) and male sex are identified as independent predictors of mortality in AAV patients. Future studies should aim at analyzing the clinical, biological, and prognostic impact of smoking on AAV with quantitative and prospectively collected smoking‑related information, assessing smoking impact on various AAV phenotypes, as well as examining the effect of passive smoking to further investigate the relationship.
- Al‑Hussain T, Hussein MH, Conca W, et al. Pathophysiology of ANCA‑associated vasculitis. Adv Anat Pathol. 2017; 24: 226‑234. | Crossref
- Salvador F. ANCA associated vasculitis. Eur J Intern Med. 2020; 74: 18‑28. | Crossref
- Perricone C, Versini M, Ben‑Ami D, et al. Smoke and autoimmunity: the fire behind the disease. Autoimmun Rev. 2016; 15: 354‑374. | Crossref
- Rosso M, Chitnis T. Association between cigarette smoking and multiple sclerosis: a review. JAMA Neurol. 2020; 77: 245‑253. | Crossref
- Speyer CB, Costenbader KH. Cigarette smoking and the pathogenesis of systemic lupus erythematosus. Expert Rev Clin Immunol. 2018; 14: 481‑487. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION