Consistency assessment and visualization of recommendations on gastroesophageal reflux disease: a scoping review of clinical practice guidelines
Key words: clinical practice guideline, evidence, gastroesophageal reflux disease, inconsistency, recommendation



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Consistency assessment and visualization of recommendations on gastroesophageal reflux disease: a scoping review of clinical practice guidelines
Introduction: Gastroesophageal reflux disease (GERD) is a highly prevalent gastrointestinal disorder that causes diverse esophageal and extraesophageal symptoms. Many clinical practice guidelines (CPGs) have been issued around the world to provide practical evidence regarding GERD management. However, some of the recommendations discussed in various CPGs are inconsistent across individual documents.
Objectives: We aimed to summarize the evidence from CPGs on GERD and assess the consistency of the recommendations.
Methods: In this scoping review, we identified current CPGs on the clinical management of GERD, which were comprehensively searched for in electronic databases and on relevant scientific websites. The recommendations were extracted using the population‑intervention‑comparison framework and were subsequently categorized into Tables.
Results: Ultimately, 24 CPGs were identified. They included 86 recommendations, which were classified into 5 categories: definition, epidemiology, diagnosis, treatment, and complications. Among the identified recommendations, 68 were proposed in at least 2 CPGs, and they were assessed for the consistency of direction and strength. Overall, 32.4% of the recommendations (22/68) were consistent in direction and strength, whereas 60.3% (41/68) were consistent in direction but inconsistent in strength. Moreover, 7.4% (5/68) were inconsistent in direction. These referred to the relationship between GERD and tobacco consumption, Helicobacter pylori infection, diagnostic utility of the 2‑week proton pump inhibitor test, cessation of special food, and antireflux surgery for GERD with extraesophageal symptoms.
Conclusions: Most CPG recommendations regarding GERD were consistent in direction, except for 5 discrepancies, for which further well‑designed, large‑scale research is required to explain the inconsistency.
What's new?
Gastroesophageal reflux disease (GERD) is a common gastrointestinal disorder that imposes a heavy economic burden around the world. Our study identified clinical practice guidelines (CPGs) issued after 2010 and summarized the recommendations on GERD management with respect to definition, epidemiology, diagnosis, treatment, and complications. In addition, we assessed the consistency of the evidence and reported the current inconsistencies, which referred to the relationship between GERD and tobacco consumption, Helicobacter pylori infection, diagnostic utility of the 2‑week proton pump inhibitor test, cessation of special food, and antireflux surgery for GERD with extraesophageal symptoms. These inconsistencies in the included CPGs might be linked to the reviewed evidence, local conditions, and CPG developers’ preference. More well‑designed trials are warranted in the future to clarify the observed inconsistencies.
Introduction
Gastroesophageal reflux disease (GERD) is a common gastrointestinal disorder characterized by a complex presentation and substantial morbidity. It is likely caused by the imbalance between reflux exposure, epithelial resistance, and visceral sensitivity.1 GERD is generally defined as pathologic regurgitation of gastric contents into the esophagus or mouth. It causes diverse esophageal and extraesophageal syndromes, such as heartburn, regurgitation, esophagitis, and even esophageal adenocarcinoma.2 It is estimated that GERD affects approximately 10% to 30% of the population worldwide, and the overall prevalence of GERD symptoms experienced at least once a week is around 13.3%, with a considerable geographic variation.3 The 2017 Global Burden of Diseases, Injuries, and Risk Factors Study4 reported that the all‑age prevalence of GERD increased by 18.1% (from 7.86% in 1990 to 9.28% in 2017). It was higher in the United States, Eastern Europe, Latin America, North Africa, and the Middle East, and lower in Asia Pacific, East Asia, France, and Iceland. Of note, the prevalence of GERD had been increasing due to the aging of the population, and it peaked at 18.82% among individuals aged 75 to 79 years. The research on GERD has advanced a lot in recent years due to the abovementioned severe disease burden, and encompasses aspects such as utility of the diagnostic methods, long‑term safety of proton pump inhibitors (PPIs), role of lifestyle modifications, and effect comparison of surgical therapeutic modalities.2
To date, quite a few evidence‑based clinical practice guidelines (CPGs) have been issued to present standards for the management of GERD in various countries and territories. However, as a result of diversity in demography as well as medical technology advancement and availability, these documents focused on different aspects and offered inconsistent perspectives. Typically, when independent CPG development groups review the relevant evidence and reach inconsistent conclusions regarding the same recommendation, likely considering various preferences and local conditions, the credibility of the evidence would decrease and the inconsistencies can cause confusion.5 Therefore, any inconsistencies require thorough comparison and discussion, which might help avoid clinical practice errors and improve patient outcomes.
Although the CPGs on GERD management are relatively abundant, the consistency of the recommendations proposed in individual documents has not yet been assessed. Therefore, we performed this scoping review to summarize the available evidence and evaluate the consistency of the recommendations included in current GERD‑related CPGs.
Methods
The present review was based on the methodological framework for conducting scoping studies.6 Due to the fact that it did not involve any patient data, ethics review and approval were not required.
Search strategy
A comprehensive search was performed in 6 electronic databases, including PubMed (via Medline), Embase, the Cochrane Library, China Knowledge Resource Integrated Database, Chinese Biomedical Database, and the WanFang Database, from the inception to June 9, 2022, using variations on the search terms gastroesophageal reflux and guideline. We also searched websites such as UpToDate (www.uptodate.com), Medlive (a Chinese website presenting domestic and foreign guidelines; www.medlive.cn), and websites of relevant professional societies, such as the World Gastroenterology Organization, International Society for Diseases of the Esophagus, American Gastroenterological Association, American College of Gastroenterology (ACG), American Society for Gastrointestinal Endoscopy, European Association of Endoscopic Surgery, Asian Pacific Association of Gastroenterology, and Japanese Society of Gastroenterology. Furthermore, a manual search was conducted by screening the reference lists of the relevant records. The search strategies used in the study are presented in Supplementary material, Table S1.
Selection criteria
We identified the CPGs that discussed the management of GERD and presented clear recommendations. Considering the applicability and availability, we only included the CPGs developed or updated after January 2010 and published in English or Chinese. Two reviewers (X‑YZ and K‑LY) screened the titles and abstracts of the records retrieved from the databases and independently screened the full texts for eligible studies. Any disagreements between the 2 reviewers were solved by consulting a third reviewer (QW).
Data extraction
Two reviewers (X‑YZ and K‑LY) independently used a data extraction sheet to extract data from the included CPGs. The following information was extracted: author / organization, year of publication, country / region, and recommendations (including the contents of recommendations, quality of evidence, and strength of recommendations). For the sake of consistency and comparability, we extracted the recommendations using the population‑intervention‑comparison (PIC) framework5 and classified them into the following 5 categories: definition, epidemiology, diagnosis, treatment, and complications, based on the general aspects considered in the CPGs.
Consistency assessment
Two reviewers (X‑YZ and K‑LY) independently determined the direction and strength of each recommendation listed in the included CPGs, and assessed their consistency using a simplified version of the method proposed by Alper et al.5 The direction of each recommendation was assessed based on the relation between the Intervention (I) and Comparison (C). The relation was described as “for” (ie, I recommended over C), “against” (ie, I not recommended, but C recommended), or “insufficient” (ie, no clear statement on which one was better). Only the recommendations proposed in 2 or more CPGs concerning the same aspect were assessed for consistency in direction (ie, consistent or inconsistent). If the direction of a single recommendation was assessed as the same in all CPGs, it was considered consistent in direction. If the recommendation was evaluated as “for” in at least 1 CPG and “against” in at least 1 other CPG, it was considered inconsistent in direction. When the recommendation was simultaneously evaluated as “for” and “insufficient” or “against” and “insufficient,” it was considered consistent in direction if labelled in the same way in at least 80% of cases; otherwise, it was considered inconsistent in direction.
The strength of each recommendation was rated as “strong” (ie, strongly recommended), “weak” (ie, weakly or conditionally recommended), or “not reported.” Only the recommendations that were consistent in direction were assessed for consistency in strength. Consistency in strength meant that the strength of a single recommendation was the same in all CPGs, except for those that did not report it. Inconsistency in strength indicated that the recommendation was simultaneously evaluated as “strong” in at least 1 CPG and as “weak” in at least 1 other CPG.
Statistical analysis
The characteristics of the included CPGs and the qualitative synthesis of GERD‑related recommendations are presented in a descriptive, narrative form and in a Table format using Excel 2019 (Microsoft, Redmond, Washington, United States). We used a bar graph to show the results of the recommendation consistency assessment, with numbers of cases and percentages, using Excel 2019. Furthermore, we prepared a bubble chart to demonstrate the details of the inconsistency analysis using Photoshop 2018 (Adobe, San Jose, California, United States).
Results
Literature search and study selection
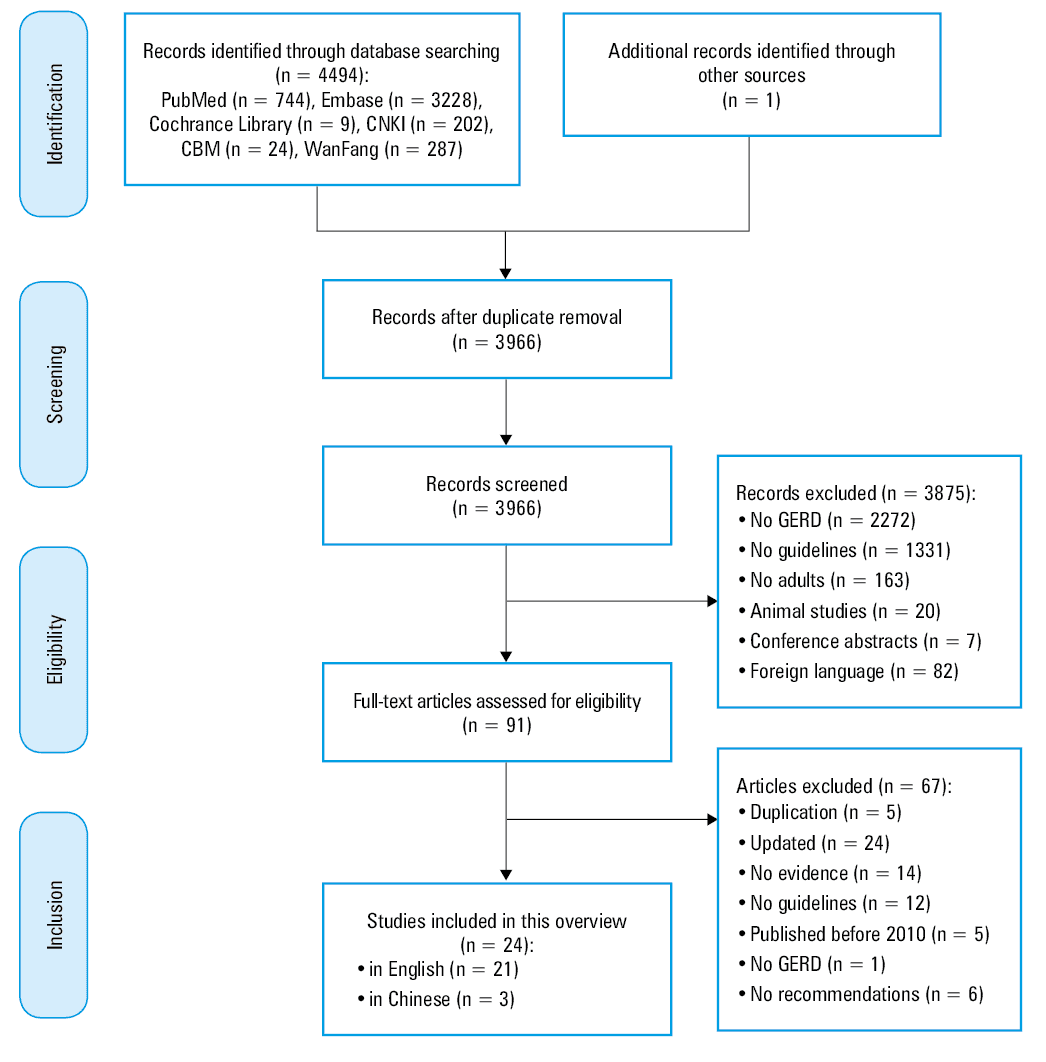
Initially, 4495 potentially relevant records were identified. Of those, 529 were excluded due to duplication, 3875 were excluded after assessing the titles and abstracts for consistency with the inclusion and exclusion criteria, and 91 potential studies were found eligible for full‑text screening. We finally analyzed 24 CPGs, including 21 documents in English and 3 in Chinese. The flowchart of the literature search and study selection process is shown in Figure 1.
Characteristics of the included studies
Among the 24 CPGs included in the study, 13 were issued in Asia (including China,7-10 Japan,11 Thailand,12 South Korea,13,14 India,15 Pakistan,16 Philippines,17 and Asian regional organizations18,19), 4 were published in Europe (including Poland,20 Romania,21 and European regional organizations22,23), 3 in the United States,24-26 1 in Brazil,27 and 3 documents were developed by international organizations.28-30 All the CPGs were published between 2010 and 2022. There were 22 CPGs that reported the system used for the hierarchy of evidence, comprising the Grading of Recommendations Assessment, Development, and Evaluation (GRADE; n = 177-14,17-19,21,24-26,28,30), Oxford Centre for Evidence‑Based Medicine (OCEBM; n = 416,20,23,27), and Canadian Task Force on the Periodic Health Examination (CTFPHE; n = 115). In total, 21 CPGs7,9-21,23-28,30 reported the quality of evidence and 13 CPGs10-19,21,24,25 reported the strength of recommendations. The characteristics of the included CPGs are summarized in Table 1.
Region | First / corresponding author, year | Country | Organization | Contents | Hierarchy of evidence system |
Abbreviations: CTFPHE, Canadian Task Force on the Periodic Health Examination; GRADE, Grading of Recommendations Assessment, Development, and Evaluation; OCEBM, Oxford Centre for Evidence‑Based Medicine | |||||
International | Pauwels et al,28 2019 | – | International Society for Diseases of the Esophagus (ISDE) | Treatment, complications | GRADE |
Hunt et al,29 2017 | – | World Gastroenterology Organization (WGO) | Epidemiology, diagnosis, treatment, complications | – | |
Roman et al,30 2017 | – | Porto consensus | Diagnosis, treatment | GRADE | |
Asia | Iwakiri et al,11 2022 | Japan | Japanese Society of Gastroenterology (JSGE) | Definition, epidemiology, diagnosis, treatment, complications | GRADE |
Maneerattanaporn et al,12 2022 | Thailand | – | Definition, diagnosis, treatment, complications | GRADE | |
Hou et al,7 2021 | China | Chinese Association of Gastroenterologist and Hepatologists, Chinese Society of Digestive Endoscopology | Definition, diagnosis, treatment | GRADE | |
Goh et al,18 2021 | South‑East Asia | – | Epidemiology, diagnosis, treatment | GRADE | |
Jung et al,13 2021 | South Korea | Korean Society of Neurogastroenterology and Motility (KSNM) | Definition, epidemiology, diagnosis, treatment | GRADE | |
Chen et al,8 2020 | China | Chinese Society of Gastroenterology, Chinese Medical Association | Definition, diagnosis, treatment, complications | GRADE | |
Bhatia et al,15 2019 | India | Indian Society of Gastroenterology (ISG) | Definition, epidemiology, diagnosis, treatment, complications | CTFPHE | |
Wu et al,9 2019 | China | Chinese Association for International Exchange and Promotion of Healthcare | Definition, epidemiology, diagnosis, treatment, complications | GRADE | |
Seo et al,14 2018 | South Korea | Korean Anti‑Reflux Surgery Study Group (KARS) | Definition, diagnosis, treatment | GRADE | |
Fock et al,19 2016 | Asian‑Pacific region | Asian Pacific Association of Gastroenterology (APAGE) | Definition, epidemiology, diagnosis, treatment, complications | GRADE | |
Niaz et al,16 2015 | Pakistan | Pakistan Society of Gastroenterology | Definition, diagnosis, treatment, complications | OCEBM | |
Sollano et al,17 2015 | Philippines | Philippine Society of Gastroenterology (PSG) | Definition, diagnosis, treatment, complications | GRADE | |
Sheu et al,10 2015 | Taiwan, China | – | Epidemiology, diagnosis, treatment, complications | GRADE | |
Europe | Świdnicka‑Siergiejko et al,20 2022 | Poland | Polish Society of Gastroenterology | Definition, diagnosis, treatment, complications | OCEBM |
Zerbib et al,22 2021 | Europe | European Society for Neurogastroenterology and Motility (ESNM) | Definition, epidemiology, diagnosis, treatment | – | |
Surdea‑Blaga et al,21 2016 | Romania | Romanian Society of Neurogastroenterology | Treatment | GRADE | |
Fuchs et al,23 2014 | Europe | European Association of Endoscopic Surgery (EAES) | Definition, epidemiology, diagnosis, treatment, complications | OCEBM | |
North America | Katz et al,24 2022 | US | American College of Gastroenterology (ACG) | Diagnosis, treatment, complications | GRADE |
Slater et al,25 2021 | US | Society of American Gastrointestinal Endoscopic Surgeons (SAGES) | Treatment | GRADE | |
Muthusamy et al,26 2015 | US | American Society for Gastrointestinal Endoscopy (ASGE) | Diagnosis, treatment, complications | GRADE | |
South America | Moraes‑Filho et al,27 2010 | Brazil | Brazilian Medical Association | Diagnosis, treatment | OCEBM |
Contents of recommendations
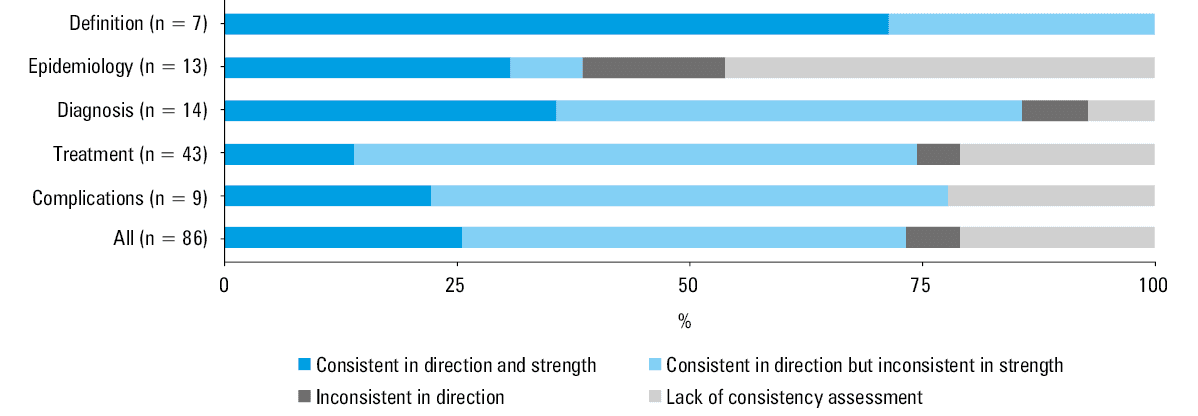
Based on the 24 CPGs included in the analysis, we generated 86 recommendations with respect to definition (n = 7), epidemiology (n = 13), diagnosis (n = 14), treatment (n = 43), and complications (n = 9). The details are listed in Figure 2.
Definition
There were 7 recommendations regarding definition, including the definition of GERD, nonerosive reflux disease (NERD), and refractory GERD (Supplementary material, Table S2). The definitions that were proposed in the guidelines most often referred to GERD (7 documents11-13,15,17,20,23), refractory GERD (8 documents8,12,13,15,17,19,20,22), typical symptoms (6 documents7-9,12,23,29), and extraesophageal symptoms (6 documents9,12,13,15-17). A single CPG9 proposed the concept of GERD as a multidisciplinary disease due to its overlapping presentation involving the fields of gastroenterology, otorhinolaryngology, stomatology, thoracic surgery, cardiology, respiratory, and mental health.
In summary, 7 recommendations were assessed for consistency, and all of them were consistent in direction. Moreover, 5 recommendations were consistent in strength, whereas 2 were not.
Epidemiology
There were 13 recommendations regarding epidemiology, including morbidity in various regions of the world, prevalence of various GERD types, and risk factors (Supplementary material, Table S3). According to the included CPGs,9,10,13,15,18,19 the epidemiologic investigation concerning GERD was unbalanced and inadequate worldwide, and the overall prevalence of GERD was reported to be increasing, particularly in Asia. NERD was reported to be the most common manifestation of GERD,18,19,29 and reflux esophagitis (RE) and extraesophageal symptoms were less prevalent.18,19 Obesity,15,19,29 tobacco consumption,15 diet,15,29 intra‑abdominal pressure,15 posture,15 and Helicobacter pylori infection10,15 were reported to be linked with the symptoms of GERD. However, in some documents, there was insufficient evidence for the association between tobacco / alcohol consumption and GERD.15,29
To sum up, 7 recommendations were assessed for consistency. Of those, 5 were consistent in direction, but 1 of them was inconsistent in strength. The recommendations that were inconsistent in direction concerned tobacco consumption and H. pylori infection. Tobacco consumption was considered as a risk factor for GERD in 1 CPG,15 but another document suggested insufficient evidence to support such an association.29 With respect to the association between H. pylori infection and GERD, 2 CPGs19,22 indicated that the decline in H. pylori infection was unlikely to have a major role in the increasing prevalence of GERD. Two other documents10,15 reported an inverse association between the prevalence of H. pylori infection and GERD, whereas in 1 CPG29 the relationship was found not to be causative (Figure 3 and Table 2).
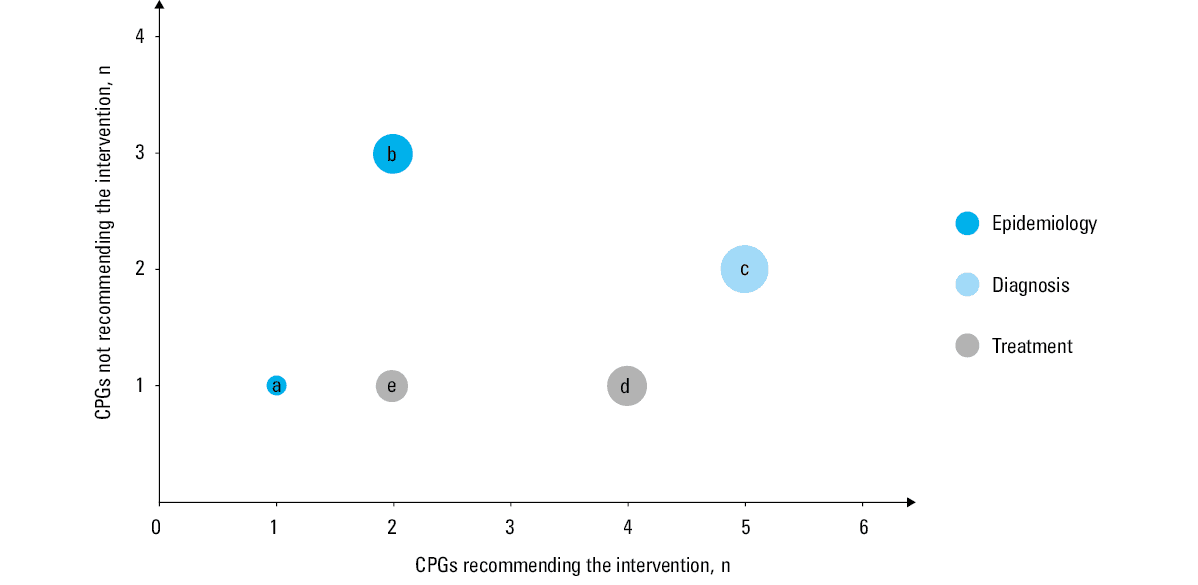
a Consumption of tobacco is a risk factor for GERD.
b Decline in Helicobacter pylori infection does not affect the prevalence of GERD.
c A 2‑week proton pump inhibitor trial therapy is a sensitive and practical test.
d Triggers for reflux symptoms should be avoided.
e Antireflux surgery is recommended for extraesophageal GERD.
Inconsistent items | CPGs | Recommendations | |
Abbreviations: CPGs, clinical practice guidelines; GERD, gastroesophageal reflux disease; H. pylori, Helicobacter pylori; PPI, proton pump inhibitor; WHO, World Health Organization | |||
Relationship between GERD and tobacco consumption | Recommended (n = 1) | Bhatia et al,15 2019 (India) | Consumption of tobacco is a risk factor for GERD. |
Not recommended (n = 1) | Hunt et al,29 2017 (WHO) | The role of smoking as a risk factor for GERD is unclear, although similarly to alcohol consumption, it is associated with an increased risk of malignancy. | |
Relationship between GERD and H. pylori infection | Recommended (n = 3) | Sheu et al,10 2015 (China) | In Taiwan, the prevalence of GERD is increasing while that of H. pylori infection is declining. |
Bhatia et al,15 2019 (India) | There is an inverse association between the prevalence of H. pylori infection and GERD. | ||
Hunt et al,29 2017 (WHO) | Although epidemiologic studies show a negative association between the prevalence of H. pylori infection and the presence and severity of GERD, this is no proof of causation. | ||
Not recommended (n = 2) | Fock et al,19 2016 (Asia‑Pacific) | The decline in H. pylori infection is unlikely to have a major role in the increase of GERD prevalence. | |
Zerbib et al,22 2021 (Europe) | Refractory GERD symptoms are not associated with the presence or absence of H. pylori infection. | ||
Diagnostic utility of the 2‑week PPI test | Recommended (n = 5) | Hou et al,7 2021 (China); Chen et al,8 2020 (China); Wu et al,9 2019 (China) | The PPI test is simple and feasible and can be used for the diagnosis of GERD. |
Maneerattanaporn et al,12 2022 (Thailand) | Patients with typical reflux symptoms without alarm features can be diagnosed with GERD if they respond to a 2‑week PPI trial. | ||
Jung et al,13 2021 (South Korea) | A 2‑week trial course of a standard‑dose PPI should be recommended as a sensitive and practical test for GERD diagnosis in patients with typical GERD symptoms. | ||
Not recommended (n = 2) | Świdnicka‑Siergiejko et al,20 2022 (Poland) | The 14‑day PPI test should not be used routinely for GERD diagnosis. | |
Hunt et al,29 2017 (WHO) | It is no longer recommended to administer an empirical short‑term (1 to 2 week) course of high‑dose PPI treatment to determine whether or not the patient’s symptoms are acid‑related, since this is neither sensitive nor specific. | ||
Cessation of special food | Recommended (n = 4) | Wu et al,9 2019 (China) | Avoid foods that may promote reflux symptoms (eg, chocolate, coffee, spicy food, oranges, tomatoes, high‑fat food). |
Bhatia et al,15 2019 (India) | Triggers for reflux symptoms (caffeine, smoking, alcohol, chocolates, spicy food), if identified, should be avoided. | ||
Niaz et al,16 2015 (Pakistan) | Other lifestyle modifications including, but not limited to, avoiding late meals, avoiding specific foods, or avoiding specific activities should be tailored to the circumstances of the individual patient. | ||
Katz et al,24 2022 (United States) | We suggest avoidance of “trigger foods” for GERD symptom control. | ||
Not recommended (n = 1) | Goh et al,18 2021 (South‑East Asia) | Routine avoidance of specific foods and drinks is not recommended. | |
Antireflux surgery for extraesophageal GERD | Recommended (n = 2) | Seo et al,13 2018 (South Korea) | Antireflux surgery is recommended for GERD patients with extraesophageal manifestations. |
Katz et al,24 2022 (United States) | In patients treated for extraesophageal reflux disease, surgical or endoscopic antireflux procedures are only recommended in patients with objective evidence of reflux. | ||
Not recommended (n = 1) | Świdnicka‑Siergiejko et al,20 2022 (Poland) | Surgical treatment is not recommended in patients with extraesophageal GERD symptoms, especially those with isolated GERD and unresponsive to PPI therapy. It can only be considered in patients with objectively confirmed GERD that is refractory to pharmacologic treatment. | |
Diagnosis
There were 14 recommendations regarding diagnosis. They discussed 7 diagnostic methods, including symptom‑based diagnosis, the 2‑week PPI test, endoscopy, pH reflux monitoring, esophageal manometry, barium esophagogram, and esophageal biopsy (Supplementary material, Table S4). Symptom‑based diagnosis8,10,12,13,15-17,20,26,27 and the 2‑week PPI test7-9,12,13 were found to be the most cost‑effective diagnostic methods. Next, pH reflux monitoring was considered to be the gold standard diagnosis in 3 CPGs.8,9,15 Barium esophagogram15,24,29 and esophageal biopsy12,20,29 were not routinely suggested for the diagnosis of GERD.
Among 13 recommendations assessed for consistency, 12 were consistent in direction. Of these, 5 recommendation were consistent in strength, and 7 were not. The recommendation that was inconsistent in direction concerned the 2‑week PPI test. Three CPGs7-9 reported that a 2‑week trial treatment with a standard‑dose PPI was a sensitive and practical test, 2 documents12,13 suggested to use the PPI test only in GERD patients with typical symptoms, and 2 CPGs20,29 stated that the 2‑week PPI test should not be routinely used (Figure 3 and Table 2).
Treatment
There were 43 recommendations regarding treatment, and they comprised lifestyle modifications, medical treatment, and surgical treatment (Supplementary material, Table S5).
There were 6 recommendations on lifestyle modifications, including weight reduction, cessation of tobacco or alcohol consumption, cessation of special food (ie, food products triggering GERD symptoms), avoiding meals before bedtime, head‑of‑bed elevation, and left lateral position while sleeping. Five recommendations were assessed for consistency, and 4 of them were consistent in direction. Among these 4, all were inconsistent in strength. The recommendation on cessation of special food was inconsistent in direction. Four CPGs9,15,16,24 indicated that the triggers for reflux symptoms (such as caffeine, tobacco, alcohol, chocolate, and spicy food), if identified, should be avoided, whereas 1 document18 proposed that routine avoidance of specific food and drinks was not recommended (Figure 3 and Table 2).
There were 25 recommendations on medical treatment, including PPI, potassium competitive acid blockers, H2 receptor antagonists (H2RAs), antacids, alginates, sucralfate, and prokinetic drugs. In this group of recommendations, 22 were assessed for consistency, and all were consistent in direction. Among these 22, 4 and 18 recommendations were consistent and inconsistent in strength, respectively. PPIs were regarded as the mainstay of treatment for GERD in 4 CPGs.9,18,20,23
There were 12 recommendations on surgical treatment, including laparoscopic and endoscopic antireflux surgeries. Seven recommendations were assessed for consistency, and 6 of them were consistent in direction. Among these 6 recommendations, 2 were consistent and 4 were inconsistent in strength. The recommendation on antireflux surgery for extraesophageal GERD was inconsistent in direction. Two CPGs14,24 recommended antireflux surgery for extraesophageal GERD, whereas 1 document20 did not (Figure 3 and Table 2).
Complications
There were 9 recommendations regarding complications, and all of them concerned Barrett’s esophagus (BE)—its prevalence, surveillance, diagnosis, and treatment (Supplementary material, Table S6). BE was defined as columnar metaplasia,9,15,19,20,23 and in all the relevant documents it was stated that its diagnosis required histopathologic confirmation.8,9,15-17,19,20,26
Seven recommendations were assessed for consistency, and all of them were consistent in direction. Among these 7 recommendations, 2 were consistent and 5 were inconsistent in strength.
Discussion
Our scoping review systematically presented the recommendations on the clinical management of GERD proposed by the current CPGs. Among those recommendations, the ones regarding treatment, including lifestyle modifications, pharmacotherapy, and surgical treatment, accounted for the largest part, and those regarding diagnosis were the second most numerous. Most of the abovementioned evidence was consistent in direction; however, 5 recommendations, including those on risk factors, the 2‑week PPI test, lifestyle modifications, and antireflux surgery, were inconsistent in direction among the included CPGs. This might be linked to the local conditions, reviewed evidence, developers’ preference, and insufficient number of randomized trials. Most of the included documents used the GRADE system to rate the quality of evidence and grade the strength of recommendations. The GRADE system is widely adopted by most organizations, such as the World Health Organization, UpToDate, and the Cochrane Collaboration, due to its simplicity, transparency, and clarity.31 Nevertheless, our results showed that the CPGs issued in Europe more often used the OCEBM system developed by the Oxford Center, which classified the quality of evidence into 5 levels and recommendation strength into 3 levels.20,23
The definitions of GERD adopted in most CPGs were similar to the Montreal definition published in 2006, which encompassed the recognized etiologic agent (ie, gastroesophageal reflux) and the identifiable signs and symptoms (ie, esophageal mucosal injuries or burdensome symptoms).1,11,13 GERD is mostly classified into NERD with reflux symptoms only and RE with esophageal mucosal injuries, which should be distinguished from functional esophageal disorders, such as reflux hypersensitivity and functional heartburn.13 With respect to the spectrum of reflux symptoms, abnormal acid exposure was the most common symptom in GERD, whereas hypersensitivity prevailed in reflux hypersensitivity and functional heartburn.32 The prevalence of GERD varied in different parts of the world, but an overall growing trend was observed.3 Before 2010, the incidence rates of GERD in Europe and the United States ranged from 10% to 20%, whereas reports on the incidence in developing countries were scarce.33 In the past decade, epidemiologic data from Asia have been increasingly reported, along with the growing prevalence, whereas data from Africa are still insufficient.29
As for the epidemiology, obesity was identified as a major and independent risk factor for GERD symptoms, mostly due to the predisposition for hiatal hernias and the direct impact of visceral adiposity.11,20,24 Nilsson et al34 found that a body mass index (BMI) increase of more than 3.5 kg/m2 was associated with a 2.7‑fold (95% CI, 2.3–3.2) greater risk of reflux symptoms.34 The participants with obesity were reported to be 2.5 times more prone to experiencing GERD symptoms or esophageal erosions than those with normal BMI.35 Apart from exacerbating GERD, obesity can also reduce the efficacy of antireflux surgery.9 Therefore, weight reduction (including lifestyle modifications and bariatric surgery) was recommended for overweight patients with GERD in 13 CPGs.7,8,12,13,15-20,22,24,29 However, other risk factors tended to be weakly associated with GERD symptoms. For example, high dietary fat intake, consumption of carbonated drinks, limited physical activity, or high intra‑abdominal pressure could induce GERD symptoms, and these factors are frequently found in individuals with obesity. Thus, the interplay between the abovementioned factors is complex and requires more epidemiologic studies.
The association between tobacco consumption (eg, smoking and chewing) and GERD was inconsistent according to the current evidence. A meta‑analysis of 30 studies reported a higher pooled prevalence of GERD symptoms in current smokers than in nonsmokers, although there was significant heterogeneity among the included studies.3 Sharma et al36 identified tobacco smoking, but not chewing, as a risk factor for GERD.36 However, several studies showed no association between tobacco consumption and GERD. To sum up, although there is no conclusive evidence on whether tobacco consumption is a risk factor for GERD, we still suggest that patients avoid any form of tobacco consumption, mainly due to the fact that it could inhibit the lower esophageal sphincter pressure and contribute to the development of reflux symptoms.15
Another frequently mentioned risk factor for GERD was H. pylori infection. A negative association between H. pylori infection and GERD has been shown in the current epidemiologic studies. The frequency of H. pylori infection is lower and that of GERD is higher in developed regions of North America, Western Europe, and Australia, whereas the trend is reversed in developing regions of South America, Eastern Europe, Asia, and Africa.37 H. pylori infection leads to a substantial inflammatory response in the gastric mucosa, which may reduce gastric acid secretion and the severity of GERD. However, this does not mean that H. pylori eradication would affect the clinical course of GERD and the efficacy of treatment. A large‑scale cohort study from South Korea38 reported that H. pylori eradication only increased the incidence of GERD and RE to the level observed in H. pylori–negative patients, and did not affect the course of GERD. Thus, a strong inverse association, but not causation, was found between these 2 factors.
Due to the efficacy of PPIs in the treatment of GERD, the response to a trial course of PPIs is currently used as a common diagnostic test. However, the accuracy of this approach was found questionable and controversial among the included CPGs. The PPI test was considered an experimental diagnosis for patients with suspected GERD, particularly for those with normal endoscopy findings, due to its simplicity, wide availability, and low cost.9 It was reported that the sensitivity and specificity of the PPI test were approximately 71% to 88.1% and 44% to 54%, respectively.39 Despite lower specificity, considering its high sensitivity and comprehensive clinical value, Chinese CPGs indicated that the PPI test could be routinely used among patients with GERD and typical symptoms, atypical symptoms, or extraesophageal symptoms.7-9 However, the CPGs issued in Thailand12 and South Korea13 only recommended to use the PPI test in patients with GERD and typical symptoms, stating that the sensitivity and specificity of this method were lower than those of the combination of endoscopy and pH‑metry in patients with GERD and atypical symptoms. In this specific subgroup of patients, the diagnostic utility of the PPI test was found to be limited, and its routine use led to overdiagnosis of GERD.40 A multinational trial evaluating the diagnostic performance of the PPI test found that a positive response to the test was observed in 69% of patients with GERD and 51% of patients without GERD.41 The CPGs issued in Poland20 and those proposed by the World Gastroenterology Organization29 suggested that the PPI test should not be used routinely for GERD diagnosis. Therefore, the observed controversy was likely to be linked to the different focus of the CPGs—the Chinese documents were focused on how to take full advantage of the PPI test, whereas the other CPGs were focused on the prevention of PPI abuse.
Reflux monitoring and esophageal manometry were also discussed in some of the CPGs as valuable diagnostic methods. pH reflux monitoring, especially 24‑hour ambulatory monitoring, could confirm excessive esophageal acid exposure and abnormal reflux events by means of comprehensive reflux parameters.9,15 An Indian study42 involving 70 patients who underwent 6 various diagnostic tests reported that pH monitoring showed the highest diagnostic accuracy (82.2%), as compared with the other 5 tests, such as esophageal biopsy (74.2%), omeprazole challenge test (74.2%), endoscopy (71.4%), barium swallow (50%), and scintigraphy (44.2%). This method had also the highest diagnostic accuracy (91.6%) for diagnosing patients with NERD (ie, GERD patients with negative endoscopy findings). However, only 3 of the included CPGs7,9,15 stated that 24‑hour pH impedance monitoring was the gold standard diagnostic method. Generally, the gold standard for the diagnosis of GERD is not universal worldwide. Thus, in one of the CPGs24 it was stated that the diagnosis of GERD should be based on a combination of symptom presentation, endoscopic evaluation of the esophageal mucosa, reflux monitoring, and response to the therapeutic intervention.
As for the treatment of GERD, PPIs have been the mainstay over the past decades.18,20 This class of drugs (eg, omeprazole, lansoprazole, pantoprazole, rabeprazole, and esomeprazole) can reduce gastric acid secretion and relieve reflux symptoms significantly by inhibiting the H+/K+ transport mechanism of the proton pump.9,17 Therefore, PPIs were recommended as the first‑line initial treatment and long‑term maintenance in most of the CPGs. Precisely due to their importance, concerns about side effects caused by overuse or long‑term use of PPIs have been raised. However, Thomson et al43 reported that there was no convincing evidence proving that the long‑term use of PPIs could cause alterations in gastric histology, iron deficiency, vitamin B12 deficiency, hip fracture, nosocomial pneumonia, or diarrhea. Most of the abovementioned side effects were only found in observational studies, with a substantial risk of confounding.44 As a result, the risk of these side effects should not be a reason for avoiding PPI use in patients with true indications, nor should it lead to unnecessary discontinuation.45 On the other hand, although PPIs are the first‑choice drugs, clinicians often prefer to use dual therapy due to better efficacy and control of GERD complications, for example, a combination of PPIs and prokinetic drugs to lower reflux exposure, or a combination of PPIs and H2RAs to inhibit nocturnal reflux.9
A consensus was reached that antireflux surgery should be commonly recommended to patients with PPI‑resistant GERD or those who refuse long‑term PPI therapy.9,15,16,28 However, there is disagreement over whether antireflux surgery should be recommended to patients with GERD and extraesophageal symptoms. Some studies showed that antireflux surgery could effectively relieve extraesophageal manifestations, such as laryngopharyngeal reflux, cough, and asthma.9,13 A large retrospective review of 420 patients with extraesophageal symptoms reported that complete resolution of symptoms was observed in the majority of participants after antireflux surgery, and that 72% of the patients were satisfied with their symptom control at the latest follow‑up.46 Therefore, the CPG14 published in South Korea in 2018 strongly recommended the surgery. However, in their review of 25 studies, Iqbal et al47 reported that the extent of symptom improvement was wide, ranging from 15% to 95%. Furthermore, in the ACG guideline,24 the recommendation for surgery was weak. The 2022 Polish CPG20 proposed that surgical treatment should not be performed in patients with extraesophageal GERD symptoms, mainly due to the lack of sufficient data from randomized trials. Thus, the conclusive view on the role of surgery in the treatment of extraesophageal symptoms requires larger, prospective, and controlled studies.
BE, first described by Norman Barrett in 1950, refers to the pathologic presence of columnar metaplasia in the esophagus.48 The surveillance of BE is not recommended in the general population; however, it is recommended in high‑risk groups (eg, men over 60 years old with GERD symptoms present for at least 10 years), as BE is a premalignant lesion potentially leading to esophageal adenocarcinoma, with an annual incidence of 0.33% (progression from BE without dysplasia), 0.54% (progression from BE with low‑grade dysplasia), and 6.58% (progression from BE with high‑grade dysplasia).49 With the current advances in the field of endoscopic techniques, some novel endoscopic detection methods for patients with BE have emerged, such as chromoendoscopy, enhanced‑magnification endoscopy, narrow‑band imaging magnification procedure, linked color imaging, blue laser imaging systems, and confocal laser endoscopy. A meta‑analysis by Bennett et al49 indicated that the current random biopsy protocols could be replaced by targeted biopsies with chromoendoscopy, narrow‑band imaging, and confocal laser endoscopy. Although endoscopy plays a main role in the surveillance of BE patients, it remains controversial due to insufficient data from randomized trials, especially on the surveillance of BE without dysplasia. In the CPG published in Pakistan16 it was stated that the overall survival benefit associated with endoscopic surveillance was not clear. A population‑based cohort study50 showed that the overall mortality rate in patients with BE was similar to that observed in an age- and sex‑matched control group. The esophageal adenocarcinoma–related mortality in patients with BE was reported to be low, irrespective of whether the patients underwent endoscopic surveillance.49 In contrast, some CPGs8,19 suggested that follow‑up of the BE patients without dysplasia should take place every 3 to 5 years, and the BE patients with dysplasia should be monitored even more closely. To some extent, these recommendations are likely to be linked with the local economy. Therefore, the optimal protocol for follow‑up endoscopic surveillance in patients with BE needs further research.
Limitations
There are some limitations to our study. First, we only included CPGs published in English and Chinese. This might have led to missing out some GERD‑related guidelines published in other languages. Second, some recommendations cannot be presented by the PIC framework, which might result in difficulties in terms of recommendation comparison. Third, for some main research questions, there might be reporting bias due to the diverse preference and focus on different CPGs.
Conclusions
Our study presented the currently available evidence and displayed the inconsistency in direction of the recommendations by summarizing the published CPGs on the management of GERD to provide a reference for future research and clinical practice. Further well‑designed, large‑scale studies should be performed to provide more data on the aspects that were found inconclusive in the analyzed CPGs, that is, the impact of tobacco consumption and H. pylori infection on the prevalence of GERD, the indications for the 2‑week PPI test among patients with different presentations of GERD, and the efficacy of antireflux surgery in patients with extraesophageal GERD.
- Vakil N, van Zanten SV, Kahrilas P, et al. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence‑based consensus. Am J Gastroenterol. 2006; 101: 1900‑1920. | Crossref
- Katzka DA, Kahrilas PJ. Advances in the diagnosis and management of gastroesophageal reflux disease. BMJ. 2020; 371: m3786. | Crossref
- Eusebi LH, Ratnakumaran R, Yuan Y, et al. Global prevalence of, and risk factors for, gastro‑oesophageal reflux symptoms: a meta‑analysis. Gut. 2018; 67: 430‑440. | Crossref
- Dirac MA, Safiri S, Tsoi D, et al. The global, regional, and national burden of gastro‑oesophageal reflux disease in 195 countries and territories, 1990‑2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol Hepatol. 2020; 5: 561‑581.
- Alper BS, Price A, van Zuuren EJ, et al. Consistency of recommendations for evaluation and management of hypertension. JAMA Netw Open. 2019; 2: e1915975. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION