Intussusception caused by an extremely rare tumor: undifferentiated spindle cell sarcoma



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Intussusception caused by an extremely rare tumor: undifferentiated spindle cell sarcoma
A 28‑year‑old woman with no significant medical history was admitted to the surgical department with a suspicion of intussusception. The patient complained of abdominal pain lasting for about 2 weeks. Moreover, for 4 weeks she suffered from persistent diarrhea (up to 7 stools per day), and there was rectal bleeding on the day of admission. The laboratory workup showed white blood count of 11.7 × 109/l (reference range [RR], 4–10 × 109/l) and a C‑reactive protein level of 16.3 mg/l (RR, <5 mg/l). On physical examination, the abdomen was soft, painful on palpation in the lower quadrant, with the greatest intensity in the right iliac fossa, with a positive Blumberg sign locally. Computed tomography revealed displaced intestinal loops in layers, with the presence of double intestinal loops intersecting each other. The length of the intussusception was approximately 15 cm. At the end of the lesion, a soft tissue conglomerate was found of an estimated size 35 mm × 38 mm (Figure 1A and 1B). The patient was qualified for urgent surgery. Intraoperative intussusception of the cecum with the distal ileum was exposed (Figure 1C). After incision of the cecum, a tumor with a wide base emerging from the intestine was found in its lumen (Figure 1D). Right hemicolectomy was performed. The continuity of the digestive tract was restored with a side‑to‑side antiperistaltic anastomosis. The tumor was excised totally, and the margins of the resection were negative (R0 resection). The postoperative course was uneventful. The cross‑sections of the lesion showed a 4.5 cm × 4 cm large intestine tumor.
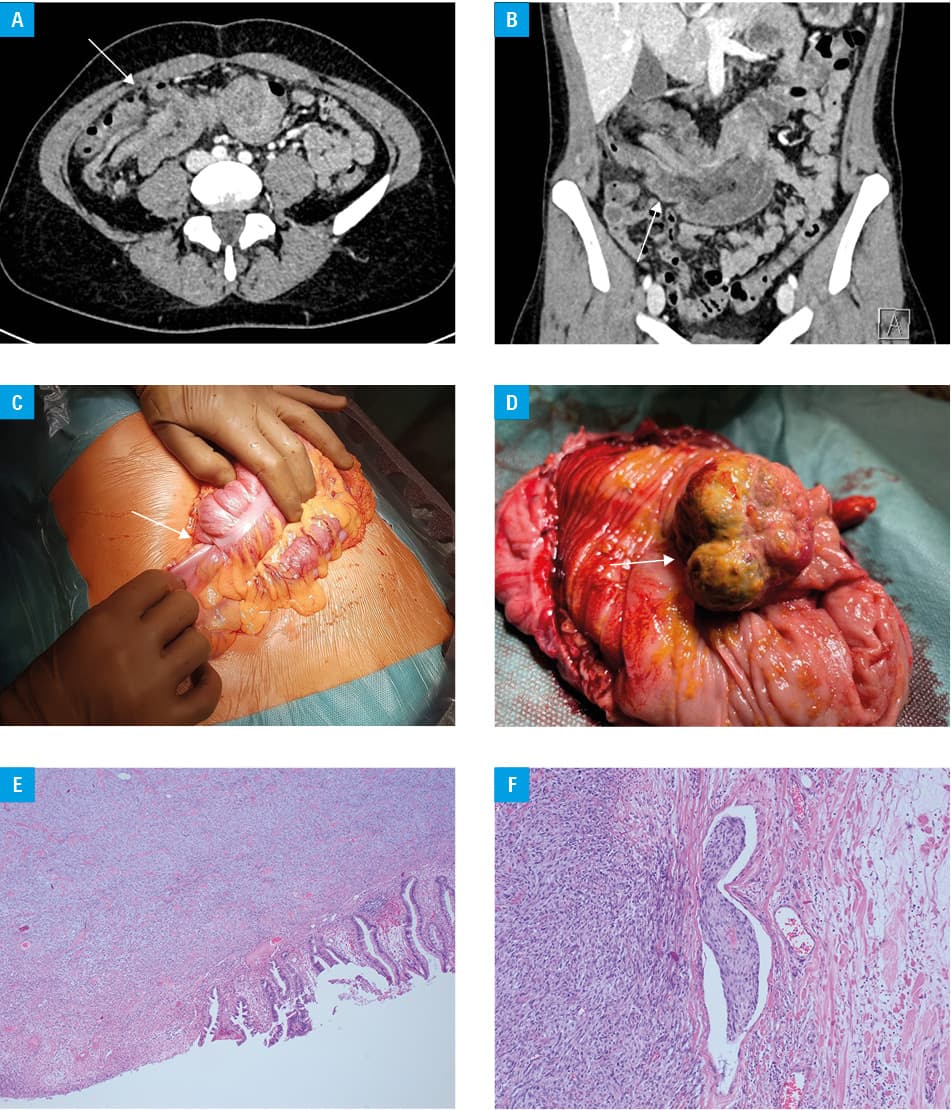
Histopathologic examination revealed a tumor composed of bundles of short spindle neoplastic cells with brisk mitotic activity (Figure 1E and 1F). The tumor invaded full thickness of the colon wall and pericolonic tissues. On immunohistochemical staining, the tumor cells showed diffuse CD10 and SDHB, and focal CD34 and panCK expression. There was no expression of CD117, S100, EMA, SMA, Desmin, Caldesmon, DOG1, STAT6, ALK1, DOG1, Pan‑Trk, SOX10, or MDM2. The Ki67 proliferation index was high, up to 65%. Molecular tests for the rearrangement of the SS18 gene, mutations in the KIT and PDGFRA genes, and the next generation sequencing analysis with FusionPlex Expanded Sarcoma Kit for Illumina (ArcherDx, Boulder, Colorado, United States) were performed. The tests did not confirm the rearrangements or mutations in any of the examined genes. The final histopathologic diagnosis was established as undifferentiated spindle cell sarcoma (USCS), histologic Fédération Française des Centres de Lutte Contre le Cancer grade 3. Three lymph nodes and a section of the greater omentum were found in the specimen, all of them without neoplastic changes.
According to the etiology of adult intussusception, the pooled rates of malignant tumors, benign tumors, and idiopathic causes are respectively 32.9%, 37.4%, and 15.1%.1 Undifferentiated spindle cell sarcomas are exceedingly rare tumors. Between 1998 and 2010 there were only 3 cases of USCS of the colon or rectum described in the literature.2 USCSs belong to the category of nongastrointestinal tumor (non‑GIST) spindle cell sarcomas. The distinction between gastrointestinal tumors (GISTs) and non‑GISTs is clinically important due to different treatment and outcomes.2 GISTs can be treated with several drugs, such as oral tyrosine kinase inhibitor, or radiotherapy,3 and for non‑GISTs the radical surgery remains the best possible treatment.2 Due to the small number of USCS cases, more sophisticated diagnostic methods of distinguishing GISTs from non‑GISTs should be established. A recent study provides results that seem to support the usage of radiomics in diagnostics of gastrointenstinal tumors.4 Further research should focus on faster differential diagnosis of intra‑abdominal tumors in order to establish diagnostic standards.
- Hong KD, Kim J, Ji W, Wexner SD. Adult intussusception: a systematic review and meta‑analysis. Tech Coloproctol. 2019; 23: 315‑324. | Crossref
- Ikoma N, Roland CL, Cormier JN, et al. Nongastrointestinal stromal tumor spindle cell sarcomas of the colon or rectum. Am Surg. 2018; 84: 570‑575. | Crossref
- Cassier PA, Fumagalli E, Rutkowski P, et al. Outcome of patients with platelet‑derived growth factor receptor alpha‑mutated gastrointestinal stromal tumors in the tyrosine kinase inhibitor era. Clin Cancer Res. 2012; 18: 4458‑4464. | Crossref
- Starmans MPA, Timbergen MJM, Vos M, et al. Differential diagnosis and molecular stratification of gastrointestinal stromal tumors on CT images using a radiomics approach. J Digit Imaging. 2022; 35: 127‑136. | Crossref
ARTICLE INFORMATION