Two cases of port catheter migration to the right ventricle: is it a rare complication in patients with cancer?



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Two cases of port catheter migration to the right ventricle: is it a rare complication in patients with cancer?
Due to the constantly growing pool of available chemotherapy regimens, the use of central venous catheters (CVCs) has become an increasingly common method of therapy delivery that ensures safe and effective administration of chemotherapy.1,2 Furthermore, in patients with cancer, CVCs are used to administer other medications, fluid therapy, as well as total parenteral nutrition.3 Despite the advantages of using vascular ports, complications associated with their use can be very dangerous and, if untreated, potentially fatal.4 One of the most serious complications is a migration of the whole catheter or its part to the heart, which may occur through 2 main mechanisms: detachment or rupture.5 This paper presents 2 cases of complications related to port catheter use that occurred in the Lower Silesian Oncology, Pulmonology and Hematology Center in Wrocław, Poland.
Patient 1 was a 49‑year‑old woman with an asthenic body build, who was undergoing treatment for breast cancer. She was admitted to receive another chemotherapeutic infusion. A suspicion of catheter obstruction was raised during drug delivery through the port. Chest X‑ray showed complete separation of a fragment of the catheter, which had migrated into the right atrium and ventricle (Figure 1A). No other alarming symptoms were observed, but the situation was considered urgent and the patient was referred for vascular surgery. Endovascular removal of the detached catheter was performed by puncture of the right femoral vein in the groin under local anesthesia. An introducer was inserted through the inferior vena cava to the right ventricle, which was clamped at the proximal end of the embolized catheter. The entire catheter was removed using a 6‑F snare (Figure 1B). The procedure took approximately 1.5 hours. The catheter removal resulted in a quick recovery of the patient, who was able to continue her therapy.
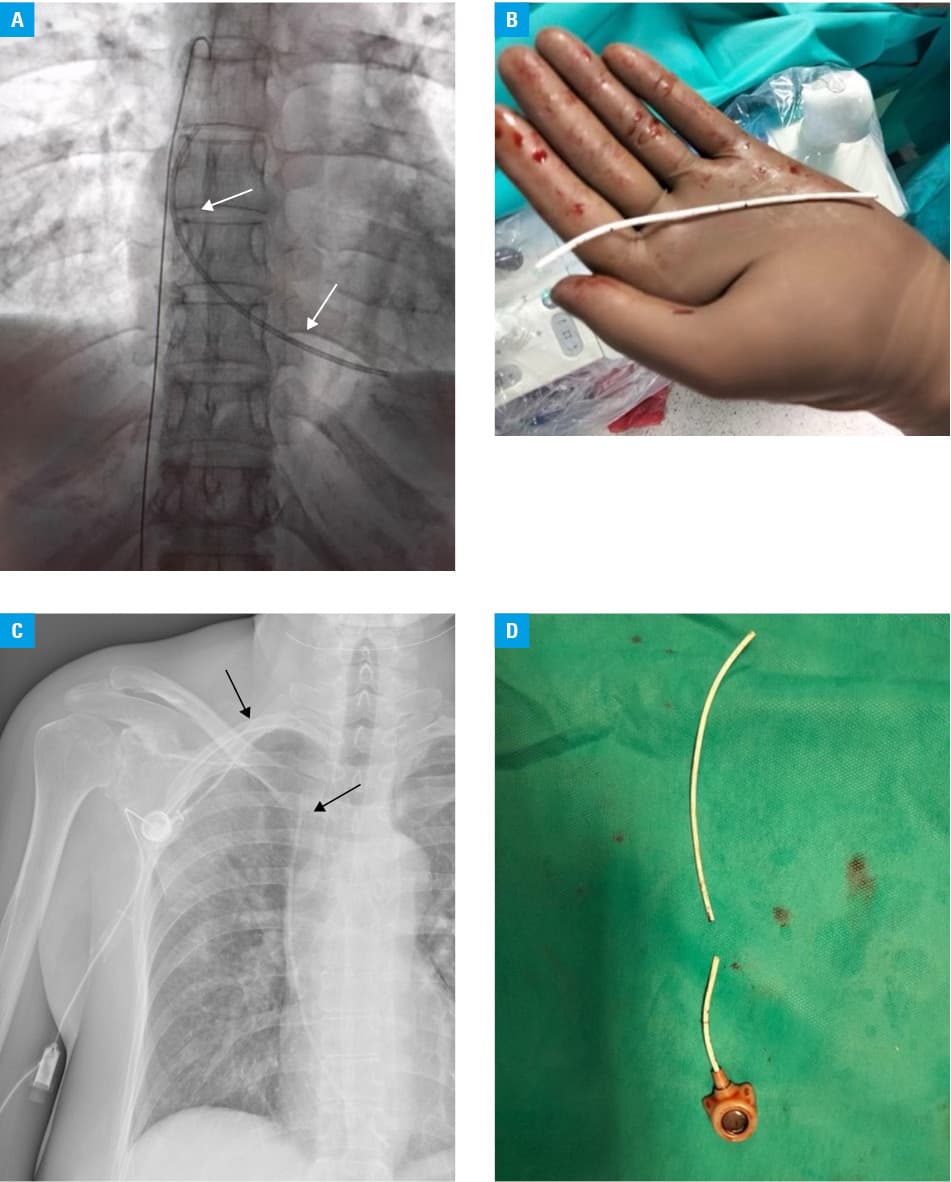
Patient 2, a 43‑year‑old woman treated for breast cancer (pT3N1a), was admitted for a diagnostic liver biopsy. The day after the biopsy, it was reported that the port could not be flushed during nursing procedures, and the patient reported pain during removal of the needle from the port by a nurse. Chest X‑ray showed rupture of the vascular catheter in the projection of the sternal extremity of the clavicle. It was visible on the image that the distal end of the catheter had moved to the right ventricle (Figure 1C). No other suspicious symptoms were observed in the postbiopsy period; however, due to a high risk of complications, the patient was urgently referred for vascular surgery. On the same day, endovascular removal of the fractured part of the catheter was performed (Figure 1D). After removal of the fragment of the vascular catheter from the right ventricle, the patient had the port removed and replaced with a new one. The postprocedural period was uneventful.
Port catheter detachment is an uncommon diagnosis that may lead to potentially harmful complications. Due to numerous risk factors, the group that requires special supervision are breast cancer patients. Because of the growing importance of chemotherapy in modern oncologic treatment and the increasing number of patients with cancer, complications related to vascular port use may become more frequent in clinical practice.4,5
- Walser EM. Venous access ports: indications, implantation technique, follow‑up, and complications. Cardiovasc Intervent Radiol. 2012; 35: 751‑764. | Crossref
- Jordan K, Behlendorf T, Surov A, et al. Venous access ports: frequency and management of complications in oncology patients. Onkologie. 2008; 31: 404‑410. | Crossref
- Bishop L, Dougherty L, Bodenham A, et al. Guidelines on the insertion and management of central venous access devices in adults. Int J Lab Hematol. 2007; 29: 261‑278. | Crossref
- Intagliata E, Basile F, Vecchio R. Totally implantable catheter migration and its percutaneous retrieval: case report and review of the literature. G Chir. 2017; 37: 211‑215. | Crossref
- Rossi UG, Rollandi GA, Ierardi AM, et al. Materials and techniques for percutaneous retrieval of intravascular foreign bodies. J Vasc Access. 2019; 20: 87‑94. | Crossref
ARTICLE INFORMATION