Oral anticoagulation challenges and therapeutic dilemmas in the very elderly: to treat and how to treat octogenarians and nonagenarians?
Key words: nonagenarians, octogenarians, oral anticoagulation, thromboprophylaxis, very elderly



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Oral anticoagulation challenges and therapeutic dilemmas in the very elderly: to treat and how to treat octogenarians and nonagenarians?
The proportion of very elderly patients, namely octogenarians and nonagenarians, is expected to rise substantially over the next decades. This population is more prone to age‑dependent diseases associated with higher thromboembolic and bleeding risks. The very elderly are under‑represented in oral anticoagulation (OAC) clinical trials. However, real‑world evidence is accumulating, in parallel with an increase in OAC coverage in this patient group. OAC treatment seems to be more beneficial in the oldest age spectrum. Direct oral anticoagulants (DOACs) have the dominant market share in most clinical scenarios necessitating OAC treatment, proving at least as safe and effective as conventional vitamin K antagonists. Dose adjustments due to age or renal function often need to be made in DOAC‑treated very elderly patients. When prescribing OAC in this population, an individualized, yet holistic, approach accounting for comorbidities, comedications, altered physiological function, pharmacovigilance, frailty, compliance, and risk of falls is useful. However, given the limited randomized‑level evidence on OAC treatment in the very elderly, there are still pending questions. This review will discuss recent evidence, important practical aspects, and future directions for anticoagulation treatment in atrial fibrillation, venous thromboembolism, and peripheral artery disease in octogenarians and nonagenarians.
Introduction
The positive correlation of age with major adverse cardiovascular events (MACEs), including bleeding and thromboembolism, has been long established.1 The aging‑induced organ dysfunction, along with the usually occurring multimorbidity and polypharmacy, create a critical conundrum over whether the anticoagulation benefits outweigh the bleeding risks. In real‑world clinical practice, oral anticoagulation (OAC) drugs are usually suboptimally prescribed in elderly and very elderly patients in need of anticoagulation due to the fear of bleeding and the lack of specific randomized trials and guidelines.2
The risk factors for ischemic and bleeding events often coexist, and bleeding episodes seem to account for higher mortality rates.3 Hence, the development of individualized recommendations is particularly important in this setting. To that end, joint approaches from international working groups aimed to practically guide the anticoagulation decisions based on the existing observational data and despite the absence of an established threshold to define “elderly” and “very elderly.”4 Nevertheless, current evidence mostly concerns elderly populations (65–79 years of age), while very elderly populations (≥ 80 years of age) have been under‑represented.2 Given the rapid aging of the global population and great heterogeneity of the very elderly population, the current review aims at gathering and critically appraising the existing literature on the anticoagulation‑related outcomes in octogenarians and nonagenarians with cardiovascular disease in need of OAC.
Aging and organ function
An ancient Greek saying warns “Fear old age, for it never comes alone.” Indeed, aging exerts a negative impact on human cells, tissues, and organs through genetic, epigenetic, and environmental modulators, which might lead to diseases and adverse events.5 The multifactorial physiological phenomena underlying the increased risk for thromboembolism and bleeding are summarized in Table 1. In brief, aging affects the whole Virchow’s triad, that is, 1) hypercoagulability6 due to altered plasma levels of the hemostatic factors,7 decreased fibrinolytic efficiency,8 and increased platelet reactivity,9 2) endothelial dysfunction and vascular pathology,7 and 3) blood stasis mainly due to immobility.7
Blood coagulation factors | Change with age |
Coagulants | |
Fibrinogen | ↑ |
Factor V | ↑ |
Factor VIII | ↑ |
Factor X | ↑ |
Factor XIII | ↑ |
von Willebrand factor | ↑ |
Anticoagulants | |
Protein C/S | ↑ |
Antithrombin | ↑ in women, ↓ in men |
Fibrinolysis and thrombolysis markers | |
Plasminogen activator inhibitor‑1 | ↑ |
Thrombin‑activatable fibrinolysis inhibitor | ↑ |
Plasminogen | ↓ in women |
D‑Dimer | ↑ |
Platelets | |
Platelet count | – |
Aggregation to adenosine 5’-diphosphate or collagen | ↑ |
Contrary to the documented prothrombotic changes, an antithrombotic environment might also develop with aging, with increased bleeding tendency in the very elderly.10 Age‑related amyloid angiopathy, vascular wall alterations, and impaired renal function are possibly associated with functional platelet disorders and, thereby, enhance the risk of bleeding.11 Acquired hemopoietic disorders (such as hemophilia A and von Willebrand disease), malnutrition, and subsequent vitamin K deficiency are further mechanisms contributing to abnormal bleeding.12
Aging and pharmacovigilance
Physiological changes in the body composition (Table 2) that occur with aging (ie, reduced blood flow and altered nephron histology) have been linked with decreased renal function.13 The observed age‑related increase in body fat and decrease in body water, serum albumin, and skeletal muscle mass (lean mass) have been associated with impaired drug distribution and creatinine clearance reduction,14 which primarily affect the kinetics of drug elimination (pharmacokinetics) by increasing their plasma concentrations and their potential side effects.15
Alteration in organ physiology related to aging | |
Physiological changes | Pharmacokinetic and pharmacodynamic changes |
↑ Gastric pH | Might affect absorption |
↓ Gastric emptying | Different bioavailability / solubility of pH‑sensitive drugs |
Decreased blood flow in organs | |
↓ Renal blood flow, ↓ Glomerular filtration rate | Impaired elimination |
↓ Liver blood flow | ↓ First‑pass metabolism |
↓ Splanchnic blood flow | |
Changes in tissue and body composition | |
Changes in renal tissue histology | Impaired elimination |
Alterations in liver architecture,
↓ Hepatocyte functional mass | Phase I enzymes affected |
↓ Body water, ↓ lean body mass | ↑ Plasma concentration of hydrophilic drugs |
↑ Body fat | ↑ Half‑life of lipophilic drugs |
↓ Serum albumin | ↑ Free fraction in plasma of highly protein‑bound acidic drugs |
Nonetheless, the biochemical and physiological effects of the prescribed medications and their mechanism of action (pharmacodynamics) are also substantially affected by aging and the associated impairment in hepatic blood flow and cytochrome activity.16 The aging process also impairs gastric emptying and absorption, and subsequently the bioavailability of the received medication. These pharmacodynamic and pharmacokinetic alterations, usually co‑occurring with polypharmacy (comedication), increase interindividual variability in plasma drug concentrations and relative response,17 drug‑drug interactions and subsequent toxicity, and potentially decrease the net therapeutic benefit of several drugs, especially when considering drugs with a narrow therapeutic index, such as warfarin.18
Primary prevention of thromboembolic events in atrial fibrillation
Based on the above, OAC use in very elderly patients is a particularly complex issue, with a delicate balance between efficacy and safety. Atrial fibrillation (AF) is the most common etiology for OAC prescription in the very elderly populations, given the constantly rising AF prevalence (estimated prevalence between 10% and 17% in those aged 80 years or older).19 Βy 2060, octogenarians and nonagenarians will represent 65.2% of the whole AF population in the European Union.20 Since the cornerstone of the Atrial fibrillation Better Care (ABC) pathway21 is to avoid stroke, determining the type and dose of OAC medication is of the utmost importance in the very elderly AF populations.
Choice of the antithrombotic treatment
Several studies have already showed that older individuals may need significantly lower doses of vitamin K antagonists (VKAs) to achieve the same target international normalized ratio (INR) than younger patients.22 The presence of anemia, prior bleeding, low body weight, and aspirin use have been associated with warfarin underprescription.23 Additionally, normalization of an elevated INR is quite a slow process in the elderly AF patients, which prolongs their exposure to supratherapeutic INR levels.24 Nevertheless, warfarin remains more effective than aspirin in AF‑related stroke prevention,25 and aging per se is not an absolute contraindication for VKA prescription in AF. However, recent guidelines on AF management emphasize high quality of VKA treatment (ie, tight monitoring; time in therapeutic range >70%) and selecting an appropriate dose to minimize bleeding risk in high‑risk groups, including the very elderly.26
The lack of direct head‑to‑head comparisons, the low numbers of this population subsets, and heterogeneous inclusion and exclusion criteria of the available trials make it particularly challenging to reach definite conclusions regarding the optimal OAC drug choice.26 The totality of the existing evidence (Table 3 and Supplementary material, Table S1) suggests that antiplatelet treatment (mainly aspirin or clopidogrel) has a limited role in the prevention of thromboembolic events in the very elderly AF patients, as compared with OACs (VKAs or DOACs).27 No age and treatment interaction has been showed to attenuate the superiority of adjusted‑dose warfarin (ie, INR close to 2) or DOACs over antiplatelets in reducing the risk of stroke or systemic embolism. Furthermore, bleeding rates on antiplatelets are similar to those on OACs.28 Hence, OAC treatment remains the most effective approach to the prevention of thromboembolic events in AF,1,29-31 and the absolute benefit seems to be the highest in the oldest old, where it by far outweighs the bleeding risk.29
Study, year | Country | Number of eligible studies | Outcome assessed | Population | Effectiveness | Safety |
Abbreviations: AF, atrial fibrillation; bid, twice daily; DOAC, direct oral anticoagulant; ICH, intracranial hemorrhage; LMWH, low‑molecular‑weight heparin; MB, major bleeding; OAC, oral anticoagulant; RCT, randomized controlled trial; VKA, vitamin K antagonist; VTE, venous thromboembolism | ||||||
Sardar et al,32 2014 | United States | Meta‑analysis of 10 RCTs (on AF- and VTE‑related OAC pharmacotherapy) | DOACs (dabigatran, rivaroxaban, apixaban) compared with conventional therapy (VKAs, LMWH) | 25 031 patients aged ≥75 years (with AF or VTE / pulmonary embolism) | DOACs were more effective than a conventional therapy in the prevention of thromboembolism or VTE. | The risk of major or clinically relevant bleeding did not differ significantly for DOACs and conventional therapy. |
Ruff et al,33 2014 | United States | Meta‑analysis of 4 RCTs on AF‑related OAC pharmacotherapy | DOACs (dabigatran, rivaroxaban, apixaban, edoxaban) compared with warfarin | 27 239 AF patients aged ≥75 years | Age ≥75 years did not correlate with the significantly decreased risk of thromboembolism on DOACs. | Age ≥75 years did not correlate with the significantly decreased risk of ICH and the increased risk of gastrointestinal bleeding on DOACs. |
Lin et al,34 2015 | Singapore | Network meta‑analysis of 25 randomized and 24 nonrandomized studies comparing DOACs, warfarin, and aspirin in elderly patients with AF | DOACs (dabigatran, rivaroxaban, apixaban, edoxaban) compared with warfarin and aspirin | 94 471 randomized AF patients (mean age, 71 years) and 803 277 nonrandomized AF patients (mean age, 72 years) | DOACs reduced the risk of thromboembolism as compared with warfarin; aspirin was associated with a significantly higher risk of thromboembolism and mortality than warfarin or DOACs. | Dabigatran and rivaroxaban showed a higher risk of MB than warfarin in the older vs younger elderly; the effect was not observed on apixaban and edoxaban. In the older elderly rivaroxaban was associated with a significantly higher risk of ICH than dabigatran, apixaban, and edoxaban. |
Sadlon et al,35 2016 | Switzerland | Meta‑analysis of 8 RCTs (on AF- and VTE‑related OAC pharmacotherapy) | DOACs (dabigatran, rivaroxaban, apixaban) compared with conventional therapy (VKAs, LMWH) | 30 655 patients aged ≥75 years (with AF or VTE / pulmonary embolism) | DOACs were superior to VKAs in the prevention of thromboembolism or VTE. | Risk of major or clinically relevant bleeding did not differ significantly for DOACs and conventional therapy. |
Kim et al,36 2018 | Korea | Meta‑analysis of 5 RCTs on AF‑related OAC pharmacotherapy | DOACs (dabigatran, rivaroxaban, apixaban, edoxaban) compared with warfarin | 28 137 AF patients aged ≥75 years | DOACs showed better efficacy (thromboembolism risk reduction) and lower mortality rates than warfarin in the elderly patients. | DOACs showed comparable safety to warfarin even in patients with moderately impaired renal function. |
Caldeira et al,37 2019 | Portugal | Meta‑analysis of 4 RCTs on AF‑related OAC pharmacotherapy | DOACs (dabigatran, rivaroxaban, apixaban, edoxaban) compared with warfarin | 24 709 AF patients aged ≥75 years | DOACs demonstrated a significant stroke risk reduction in the elderly patients as compared with VKAs. Dabigatran 110 mg bid did not significantly reduce the stroke risk as compared with warfarin. | The overall comparative risk of MB on DOACs was not different from that on VKAs. Dose‑dependent increase of MB risk was observed on dabigatran vs warfarin. |
Malik et al,38 2019 | United States | Meta‑analysis of 5 substudies of RCTs and network meta‑analysis on AF‑related OAC pharmacotherapy | DOACs (dabigatran, rivaroxaban, apixaban, edoxaban) compared with warfarin | 28 135 AF patients aged ≥75 years | DOACs were found to have superior efficacy, as compared with warfarin in reducing the risk of thromboembolism. | The rate of MB was similar, but ICH was significantly lower in the patients randomized to DOAC. Apixaban was the only DOAC that significantly reduced all 3 outcomes of systemic embolization, MB, and ICH as compared with warfarin. |
Deng et al,40 2020 | China | Bayesian network meta‑analysis of 5 RCTs on AF‑related OAC pharmacotherapy | DOACs (dabigatran, rivaroxaban, apixaban, edoxaban) compared with warfarin | 28 137 AF patients aged ≥75 years | Apixaban ranked the best in efficacy (thromboprophylaxis), followed by rivaroxaban, edoxaban, dabigatran, and warfarin. | Not significant MB risk reduction; regarding safety, apixaban ranked the best, followed by edoxaban, dabigatran, warfarin, and rivaroxaban. |
The existing meta‑analyses also concur on the superiority of DOACs over VKAs or antiplatelets in thromboembolism prevention, mortality, and bleeding risk reduction32-40 (Table 3). The major concern against VKA treatment is possible intracranial hemorrhage (ICH, the most devastating form of bleeding), the risk of which increases strikingly beyond the age of 80 years, especially in the first month of a therapy.41 In a large real‑world cohort study42 investigating the trends of OAC use among newly diagnosed very elderly AF patients (>85 years old), a 3‑fold increase in OAC initiation was observed mainly due to the introduction of DOACs,43 and the 1‑year risk of thromboembolism and mortality was lower in the era of DOACs when compared with 2009. The outcome of bleeding complications on DOACs is considered more benign than on VKAs, while the approval of DOAC reversal agents further adds to the favorable bleeding profile on DOACs.44
Interestingly, recent meta‑analyses indicate that apixaban is consistently associated with the most favorable risk‑to‑benefit profile, followed by edoxaban, dabigatran, warfarin, and rivaroxaban.38-40 However, another recent large‑sample meta‑analysis of 20 observational studies suggested that despite the DOAC‑related risk reduction of ICH, elderly patients on DOACs more frequently experienced gastrointestinal bleeding (GIB) episodes than those on VKAs.33,34,38,39 Additionally, among DOACs, rivaroxaban has been linked with increased ICH occurrence, while a dose‑dependent increase in major bleeding episodes has been documented in dabigatran users.34,37
Direct oral anticoagulant dosing and renal function: an essential equilibrium to consider
According to the meta‑analysis by Kim et al,36 DOACs had a safety profile comparable to that of warfarin, even in the patients with moderately impaired renal function, if dose reduction was appropriately applied. It is common knowledge that renal function constitutes a crucial factor to determine DOAC dosing, particularly for DOACs primarily cleared by the kidney, such as dabigatran. In the very elderly AF patients, standard‑dose dabigatran (ie, 150 mg twice daily) exhibited better efficacy and equivalent safety as compared with warfarin, except for a trend toward increased GIB episodes, whereas low‑dose dabigatran (ie, 110 mg twice daily) showed similar efficacy, and similar or better safety than warfarin.45,46 In the meta‑analysis by Ruff et al,34 the analyses of subgroups including only the patients on low doses of dabigatran and edoxaban revealed decreased magnitude of DOAC‑related thromboprophylaxis and significantly lower bleeding rates than on warfarin. Another promising study carried out in Japan47 implied that the efficacy and safety of a very low dose of edoxaban (15 mg once daily) vs placebo were broadly consistent across renal function subgroups in the very elderly AF patients who were not appropriate candidates for standard DOAC doses. Moreover, a recent study48 in the very elderly AF patients did not yield significant differences in the effectiveness or safety of low‑dose vs standard‑dose rivaroxaban, whereas low‑dose apixaban was associated with a greater risk of thromboembolism and mortality without decreasing the bleeding rate, as compared with standard‑dose apixaban.Therefore, DOAC dosing emerges as an important aspect when determining the anticoagulation strategy for octogenarians and nonagenarians,49 and an accurate assessment of the renal function (ie, using the Cockcroft–Gault equation that is additionally influenced by body mass) is the basic pillar to avoid its overestimation and subsequent DOAC overdosing, which might increase the risk of bleeding.50 Low body weight per se might increase the exposure to any (D)OAC, and as such might lead to elevated risk of bleeding. Hence, a patient with sarcopenia and low body mass index may qualify for reduced OAC regimen to mitigate the bleeding risk.
Regular monitoring of the renal function is strongly recommended in the oldest old to correct modifiable causes of renal function decline, and properly adjust DOAC dosage. According to the European Society of Cardiology position paper,51 clinicians are advised to avoid dabigatran prescription at creatinine clearance below 30 ml/min, and to avoid other DOACs once the renal function has been severely impaired (creatinine clearance <15 ml/min). However, recent data provided novel insights into the role of DOACs in AF patients with end‑stage chronic kidney disease (CKD), showing that DOACs might have similar effectiveness and safety as warfarin in this subgroup of patients.52
Secondary prevention of thromboembolic events
Besides the primary prevention of thromboembolism in the oldest old, thromboprophylaxis in those with prior ischemic stroke or systemic embolism is of paramount importance, as stroke / embolism survivors are at a high risk of recurrence.53 OAC treatment should be considered after individual assessment of all eligible patients in collaboration with geriatricians and neurologists.54 Α large propensity score‑matched cohort study in Japan55 demonstrated a significantly lower risk for cerebral reinfarction, bleeding events, and ICH in the DOAC group, as compared with the warfarin group. Further secondary prevention‑oriented studies are warranted in this subgroup of patients prior to reaching definite conclusions; however, there is no evidence yet to suggest that DOACs will be less effective or safe in the very elderly AF patients with prior thromboembolic events, and age should not be deemed as a barrier for the provision of optimal secondary prevention interventions.54,56 However, the cost‑effectiveness analysis by Coyle et al57 showed that none of the DOACs would be cost‑effective in patients with previous major stroke, while in another study the cost‑effectiveness of DOACs was inversely related to the quality of INR control achieved on warfarin.58
Embolic strokes of unknown source
Since approximately every third ischemic stroke is classified as embolic stroke of unknown source (ESUS), and the risk of stroke recurrence in these patients is substantially increased,59 establishing the required OAC treatment is of great relevance for the elderly populations with prior history of ESUS. Given that the role of (undetected) AF in the patients with ESUS has not been established yet,60 randomized controlled trials (RCTs)61 aimed at investigating the efficacy or safety of DOACs vs aspirin, which is currently offered as a standard treatment to the patients with ESUS. In the ESUS participants (>75 years old) of the RE‑SPECT trial, dabigatran significantly reduced the rate of stroke recurrence as compared with aspirin.62 Given that the ATTICUS61 (apixaban profile) and NAVIGATE‑ESUS62 (rivaroxaban profile) trials were prematurely terminated, the ongoing ARCADIA trial63 will shed further light on the role of DOACs in the prevention of stroke recurrence in the older populations with prior ESUS.
Venous thromboembolism prevention
The incidence of venous thromboembolism (VTE) is particularly age‑dependent, as physiological changes in the hemostatic system (Table 1), and acquired risk factors, such as cancer and chronic inflammatory diseases, accentuate the relative risk in the very elderly.64 Although those patients are often in need of extended prophylaxis,65 and constitute a relatively high proportion of the studied populations, only a few real‑world studies enrolled specifically octogenarians and nonagenarians, most possibly due to impaired cognitive function, severe weakness, and frailty.64
The existing data from the DOAC trials in patients with VTE suggest that DOACs have overall superior safety and efficacy profiles in elderly patients (aged ≥75 years) as compared with VKAs.32,35,66 Patients aged 75 years or older who were treated with DOACs due to VTE history did not have increased recurrence rate in comparison with younger patients. Conversely, patients aged at least 75 years and on warfarin had increased VTE recurrence as compared with younger individuals.66 In particular, apixaban or rivaroxaban showed greater safety than dabigatran as compared with VKAs.66 In subgroup analyses of elderly patients with impaired renal function, treatment with VKAs was both less effective and less safe, which might be attributed to more predictable pharmacokinetics of DOACs and to CKD‑related accumulation of DOACs leading to higher intensity of anticoagulation.67
Cancer‑associated venous thromboembolism
An important subgroup of elderly patients that should be carefully protected against VTE are those with cancer. They have been linked with a 2- to 9‑fold higher risk of recurrent VTE under anticoagulants and a 2- to 3‑fold higher risk of major bleeding episodes than patients without cancer. Hence, anticoagulation strategies should be carefully selected in treating cancer‑associated VTE.68 A network meta‑analysis assessing low‑molecular‑weight heparin (LMWH), VKAs, and DOACs for the treatment of cancer‑associated VTE showed that the effectiveness and safety of DOACs were superior to warfarin and maybe equivalent to those of LMWH regardless of the patient age.69 A recent systematic trade‑off analysis by Yan et al69 showed that DOACs were more effective than dalteparin at a cost of slightly increased risk of clinically relevant bleeding. Hence, DOACs emerge as a safe and effective alternative therapy to LMWH, and should be considered for long‑term treatment of cancer‑associated VTE in the elderly patients who are likely to benefit from them.70 Among DOACs, edoxaban seems to offer the best risk‑to‑benefit balance69; yet apixaban might be the preferred DOAC in patients with gastrointestinal malignancies.70 However, further investigations are warranted to confirm the superiority of individual DOACs in VTE prevention in cancer patients of advanced age, and to determine the optimal time for discontinuing OAC after a VTE episode in elderly patients with cancer.71
Practical considerations regarding direct oral anticoagulant dosing for venous thromboembolism treatment
Because the risk for VTE recurrence decreases following an acute event, discontinuing anticoagulant treatment for secondary VTE prevention may be an option to consider for some older patients.72 The most challenging aspect of VTE management in the oldest old is the determination of optimal treatment duration, since both bleeding and VTE risk are elevated in this age category. Nevertheless, a potential prognostic benefit of extended antithrombotic prophylaxis in elderly patients (aged ≥75 years) has been demonstrated.65 Current guidelines do not suggest switching an anticoagulant after the first 3 months, and there are no individualized recommendations for very elderly populations because of the limited evidence.
Standard doses of DOACs or LMWH are initially recommended for the elderly patients with acute VTE, and lower DOAC doses are recommended in those who need extended anticoagulation.64,73 The selection of the appropriate dose and type of anticoagulation should consider the patient preferences and values in an individualized approach, and should be set in collaboration with vascular surgeons, geriatricians, cardiologists, and oncologists, where needed. Anticoagulant regimen and dosage after the first 6 months should be clarified and tested prospectively in larger and older populations.
Peripheral artery disease
Peripheral artery disease (PAD) is considered a global epidemic particularly regarding elderly and very elderly populations. Although secondary prevention with antithrombotic treatment seems to be the cornerstone for the prevention of adverse cardiovascular events, PAD patients are often undertreated with antithrombotic agents.74
Recent RCT‑based meta‑analyses yielded promising results showing that the use of rivaroxaban and edoxaban (either standard or low dose) combined with aspirin significantly reduced the risk for major ischemic limb events offset by a relative increase in major bleeding episodes in patients with symptomatic lower extremity PAD.75 Unfortunately, these results were not replicated in patients older than 75 years, challenging the efficacy‑safety balance of DOAC use in the geriatric populations with PAD.76 Regarding dabigatran and apixaban, there is a limited long‑term or randomized evidence supporting their use in the patients with PAD.77
From a clinical point of view, daily use of low‑dose DOACs along with aspirin in stable and postrevascularization elderly PAD patients with AF at a low or intermediate risk for bleeding and without indications for full‑dose long‑term OAC treatment seems a rather safe and effective approach.78 However, the optimal OAC strategy for the elderly patients with PAD is still characterized by a notable lack of consensus guidelines and large regional disparity in treatment patterns.78 Thereby, the likelihood of suboptimal treatment is elevated.79,80 Hence, the completion of real‑world observational studies and / or RCTs of full- and low‑dose DOACs in the elderly patients with PAD could contribute to an evidenced‑based approach on a subject‑specific level, weighing cardiovascular and limb benefits against potential bleeding risks.
Challenging comorbidities in the very elderly
The aging‑related degeneration of most physiological systems leading to the accumulation of severe comorbidities81,82 makes geriatric medicine and anticoagulation particularly complex in octogenarians and nonagenarians. Rationalizing the patient medication, deprescribing potentially unnecessary medications or prescribing polypills, and reducing the burden of polypharmacy are key elements of a holistic geriatric approach.83 The clinicians should prescribe OACs according to the existing consensus guidelines; however, some evidence might not be reliably extrapolated to patients with severe comorbidities, who are underrepresented in RCTs; thus, treatment recommendations must be personalized.
Valvular heart disease
With this aging population, the prevalence of valvular heart disease (VHD) is on the rise. The comorbidity of AF with moderate or significant VHD constitutes a rather frequent yet puzzling clinical entity in the very elderly populations.84 No interaction with age has been demonstrated in the prognostic benefit from DOACs in the patients with nonmechanical and rheumatic mitral VHD.85 On the contrary, elderly patients with mechanical mitral or aortic valves on DOACs had significantly increased risk of clotting as compared with those on VKAs.86-88 Hence, there is a strong evidence behind the recommendation that patients with mechanical heart valves should be on lifelong anticoagulation with VKAs irrespective of age, with the INR treatment goal depending on patient‑specific factors.89 Regarding the subgroup of patients with rheumatic mitral stenosis or rheumatic heart disease–associated AF, VKAs also incurred consistently lower risk of MACEs than DOACs, without increased bleeding rates.90,91 Nevertheless, future RCTs or real‑world data are warranted to delineate the role of DOACs in very the elderly patients receiving a bioprosthetic valve / transcatheter aortic valve implantation, with and without a baseline indication for OAC or antiplatelet medication.92 Until then, clinicians should treat the elderly patients according to the existing evidence and use an individualized approach.89
Coronary artery disease
Given the increased prevalence of coronary artery disease (CAD) with advanced age, the relative anticoagulation strategy becomes challenging when dealing with comorbid AF. The existing literature suggests that bleeding risk is substantially elevated when a patient receives concomitantly OAC and antiplatelet therapy, hence, this should be generally avoided in the very elderly.93 The independent net clinical benefit of OACs (and especially of DOACs) has been demonstrated in the elderly patients with stable CAD and AF.94 However, the need for antiplatelet comedication is being extensively studied so that a particular approach can be reliably established for the elderly AF patients suffering from acute coronary syndrome or undergoing percutaneous coronary intervention (PCI).95
All the existing trials96-99 demonstrated that dual therapy (ie, OAC + single antiplatelet treatment, mostly clopidogrel) more significantly reduced the risk of bleeding events than triple therapy (ie, OAC + dual antiplatelet treatment [DAPT]). In the patients with very high bleeding risk, 1) DOACs should be preferred over VKAs to reduce the occurrence of major bleeding episodes,100 2) clopidogrel should be preferred over other P2Y12 inhibitors to be concomitantly received with OACs,101 3) OAC and DAPT comedication should be only considered for the period of particularly high ischemic risk (ST‑elevated myocardial infarction, left main disease or complex PCI) and for the shortest possible time (1 month),102 and 4) proton pump inhibitors, mostly pantoprazole,93 should be prescribed to reduce the risk for upper GIB during the combined dual or triple anticoagulation therapy with OACs and antiplatelets, and should be also deprescribed upon the transition to OAC monotherapy.93
End‑stage renal disease
End‑stage renal disease (ESRD) and advanced CKD constitute 2 frequent clinical entities among the very elderly patients in need of OACs. The observed platelet dysfunction and the impaired interaction between the platelets and endothelium usually affect the anticoagulation cascade in ERSD/CKD, making the OAC‑related decision taking even more challenging.103 Despite the paucity of relevant data specific for octogenarians and nonagenarians, a recent meta‑analysis in older AF patients (>65 years) demonstrated that OACs are associated with increased survival in non‑dialysis‑requiring patients, but with worse bleeding rates in those on dialysis.44 Another meta‑analysis showed that OACs did not prevent thromboembolism in (younger and older) AF patients on long‑term dialysis.104 The only real‑world study evaluating the impact of OACs in nonagenarians with CKD revealed that there was no significant prognostic difference between warfarin and non‑OAC users, whereas DOACs (especially apixaban) were associated with better prognostic course.100
Overall, the use of warfarin, dabigatran, or rivaroxaban has been associated with significantly higher bleeding rates than of apixaban or no OAC, while edoxaban has not been studied yet in the ESRD population.104 However, contradictory data exist regarding the prognostic benefit of apixaban treatment in the patients with ERSD or advanced CKD.105 Whether these data can be directly transferred to the very elderly patients with renal impairment is not clear. Hence, the benefit‑to‑harm ratio of (D)OACs in the very elderly AF patients with advanced CKD or dialysis‑requiring ERSD warrants validation in the ongoing RCTs. Until then, if the use of OAC is deemed necessary in the patients with advanced CKD (creatinine clearance 15–29 ml/min), DOACs (apixaban 2.5 mg twice daily or rivaroxaban 15 mg once daily) should be generally preferred in view of the limited efficacy and safety data on VKAs,106 along with the reported hazard of VKA‑related vascular calcification, calciphylaxis, and glomerular hemorrhage.107 Nevertheless, the decision of whether and how to initiate OACs in the patients with (dialysis‑requiring) ERSD requires a patient‑physician collaboration on a carefully considered case‑by‑case basis.107
Hematologic disorders, malignancies, and solid tumors
Hematologic disorders and solid or liquid tumors constitute further significant aging‑related comorbidities with a potential impact on OAC‑related outcomes. More specifically, anemia is commonly observed in the very elderly (prevalence of 20% to 40%),108 and has been independently associated with an increased risk of major bleeding and lower efficacy of the prescribed OACs (either VKAs or DOACs).109 Apart from the potential mechanistic explanations behind the prognostic burden of anemia (eg, reduced margination of platelets or hemostatic dysfunction), the clinicians should also consider that anemia might only be a marker of a morbidity burden, especially in the patients with CKD or tumors / malignancies, and might not be responsible for bleeding occurrence per se.110 Furthermore, thrombocytopenia has been also linked with increased bleeding risk111; therefore, both anemia and thrombocytopenia should be investigated and treated before and during OAC therapy.2
Additionally, age‑related acquired hemopoietic disorders (eg, acquired hemophilia or von Willebrand syndrome), reduction of vitamin K–dependent coagulation factors, and solid or liquid tumors might interact with the prognostic course of AF in the very elderly, increasing the risk of bleeding.112 Metabolic drug‑drug interactions (with chemotherapeutic and antibiotic agents), chemotherapy‑induced thrombocytopenia (or myelosuppression), potential metastases and frequent need for surgery or invasive procedures further increase the difficulty in solving that conundrum. A recent meta‑analysis demonstrated better safety and efficacy profiles of DOACs than VKAs in AF patients with cancer.112 Nevertheless, the exact impact of the aforementioned clinical entities on OAC outcomes in the very elderly warrants further investigation.
Cognitive impairment, dementia, and risk of falls
One of the most challenging aspects of OAC decision‑making in the very elderly is the need to consider the patient cognitive impairment, dementia, and risk of falls prior to initiating OAC therapy.26 Particularly, frailty and the subsequent risk of falls have been associated with decreased OAC prescription,113,114 which underscores the clash of evidence‑based medicine between the OAC guidelines and geriatric guidelines.54 Numerically, deaths from falls rise almost up to 25% of those dying from thromboembolic events among elderly populations54; however, the risk of falls does not outweigh the benefits of OAC according to the current AF management guidelines.115 Overall, DOACs appear to offer superior effectiveness and safety profile to warfarin in AF patients with frailty,116 and those with a history of falls or higher risk of falls.117 Interestingly, evidence suggests that DOACs (and possibly well‑controlled VKA treatment) could even play a protective role in the prevention of cognitive decline.118 Hence, frailty, cognitive impairment, and risk of falls should not discourage either the patients or the clinicians from DOAC initiation and adherence.
Follow‑up risk assessment of the oldest old
Τhromboembolic and bleeding risks are definitely dynamic in the very elderly populations because of the accumulation of risk factors over time, frequent changes of the clinical status, polypharmacy‑related challenges, and potentially deleterious consequences of the aging process. AF patients often have multiple comorbidities, and it is a currently established part of integrated care to address the risk factors in a holistic manner according to the ABC pathway (Avoid stroke, Better symptom management, Cardiovascular and other comorbidities). Early recognition and management of bleeding‑associated conditions (ie, inadequate blood pressure control, deteriorated renal function, presence of diabetes mellitus or hematologic disorders, suboptimal nutritional status and body‑mass reduction, lack of social support, decreased compliance, and increased risk of falls) are crucial in the oldest old. Counselling and education of the patient and their close relatives / care providers can improve their understanding and adherence to thromboprophylaxis. Minimizing the impact of each modifiable risk factor through accurate initial assessment and close periodic re‑evaluation of the very old patient could maximize the net clinical benefit and the safety of OAC, verify the need for dose adjustment, and add significant prognostic benefit.
Additionally, OAC‑related decisions should be dynamically reassessed during a follow‑up, according to an integral geriatric reassessment scheme comprised of functional, clinical, mental, and social valorization besides the already established CHA2DS2‑VASc, HAS‑BLED, and SAMe‑TT2R2 scores. Such indices have been recently validated for the elderly populations, including the Barthel index (functional capacity for basic activities of daily living), the 36‑Item Short Form Survey (quality of life), the Pfeiffer test or the Mini‑Mental State Examination (cognitive status), the Frail scale, the Fried criteria or the SHARE‑FI index (frailty), the APACHE score, the Charlson Comorbidity Index or the Cumulative Illness Rating Scale (comorbidity), and the Mini Nutritional Assessment Scale‑Short Form (nutritional status). To that end, research and educational curricula should inform clinical practice guidelines individually for the frail anticoagulated elderly patients with multimorbidities, who call for a new model of collaboration and teamwork between primary care physicians, geriatricians, and cardiologists to improve cardiogeriatric care.
Remaining gaps in knowledge and future considerations
The OAC field has seen substantial improvements in the last decade after the implementation of DOACs into the daily clinical practice. However, geriatric anticoagulation decisions remain challenging, hence, future RCTs and real‑world observational studies should shed further light on OAC outcomes in the very elderly populations with AF, VTE, or PAD. Specific subanalyses on the challenging comorbidities of advanced age could further add to the preventive role of DOACs. In future trials, it is particularly important to include competing risk analyses, because octogenarians and nonagenarians are at an increased risk for noncardiovascular mortality, which might affect the documented rates of thromboembolic and bleeding events, as compared with younger populations. In the future, it appears also important to compare the risk‑to‑benefit profiles of normally (“on‑label”) reduced DOAC doses and ultra‑low doses (eg, 30 mg/day vs 15 mg/day for edoxaban, but also for other DOACs), which might have some role to play in the very elderly.119
To date, the best available data come from subanalyses of the landmark DOAC RCTs, in which, however, the older or frail patients were under‑represented. Furthermore, the enrollment criteria differed in various DOAC trials, and therefore, the existing observations should be interpreted with caution when comparing DOACs for stroke prevention in the very elderly. Hence, prospective studies using established frailty criteria, and enrolling populations with challenging comorbidities, are warranted to assess efficacy and safety end points as well as clinically relevant outcomes, such as cognitive function, cancer incidence, quality of life, functional status, and maintenance of independence. Of course, AF trials in the very elderly populations comparing DOACs with nonanticoagulant therapies (eg, AF ablation, left atrial appendage occlusion) would also be of clinical relevance. Thereby, multidisciplinary consensus geriatric guidelines could develop handy scoring systems / algorithms specifically validated for guiding OAC in the very elderly after considering all the specific risk factors of this population. This could ultimately help clinicians in a more rational and evidence‑based approach to this subset population.
Moreover, the investigation of DOAC adherence and the identification of DOAC concentration thresholds linked with a lack of benefit for each DOAC would also be interesting.66 Identifying genetic polymorphisms of substrates involved in the action of DOACs (thrombin and fibrin activity) and in the action of cytochrome CYP450 might contribute to the precision prescription.120 Furthermore, the existence of a point‑of‑care test for the level of DOAC anticoagulation and better access to DOAC‑specific reversal strategies could bolster clinical decision‑making in emergent surgeries or in need for antidote in life‑threatening bleeding conditions. Shorter half‑life of DOACs has been also reported as a potential risk when doses are skipped due to noncompliance or forgetfulness. Similarly, the frequently encountered malnutrition and hypoalbuminemia (with heterogeneous binding to proteins) in the elderly populations might also affect the DOAC pharmacokinetics. Therefore, future studies should investigate whether this variability significantly affects the risk‑to‑benefit balance in the very elderly, and all patients should be thoroughly educated regarding the bleeding risk, potential side effects, drug‑food and drug‑drug interactions, and noncompliance implications.68,120 In addition, the presence of microbleeds on magnetic resonance imaging has been documented as a predictor of a future ICH in patients on VKAs121; thus, relevant research in patients on DOACs might further aid decision making in very challenging anticoagulation conundrums. Finally, the promising ongoing trials on new DOACs (FXI or FXII inhibitors)122 appear to open prospects for further enhancing the care of the very elderly with a much more effective and safer OAC therapy.
Conclusions
This review delineates the role of DOACs and VKAs in the very elderly patients with potential multimorbidity burden (Figure 1). During the last decades, the risk‑to‑benefit balance has tipped in favor of treating the very elderly patients with OACs, and in most cases with a DOAC instead of a VKA. However, the decision to initiate (D)OAC treatment and to choose the optimal dosage for the very elderly patients should be made in a patient‑focused manner with careful attention to potential drug‑drug interactions, without any age discrimination, and with an ultimate aim to maximize the risk‑to‑benefit ratio. Given that the global octogenarian population is projected to triple by 2050, existing questions remain to be answered by future mechanistic trials and geriatric observational studies or RCTs.
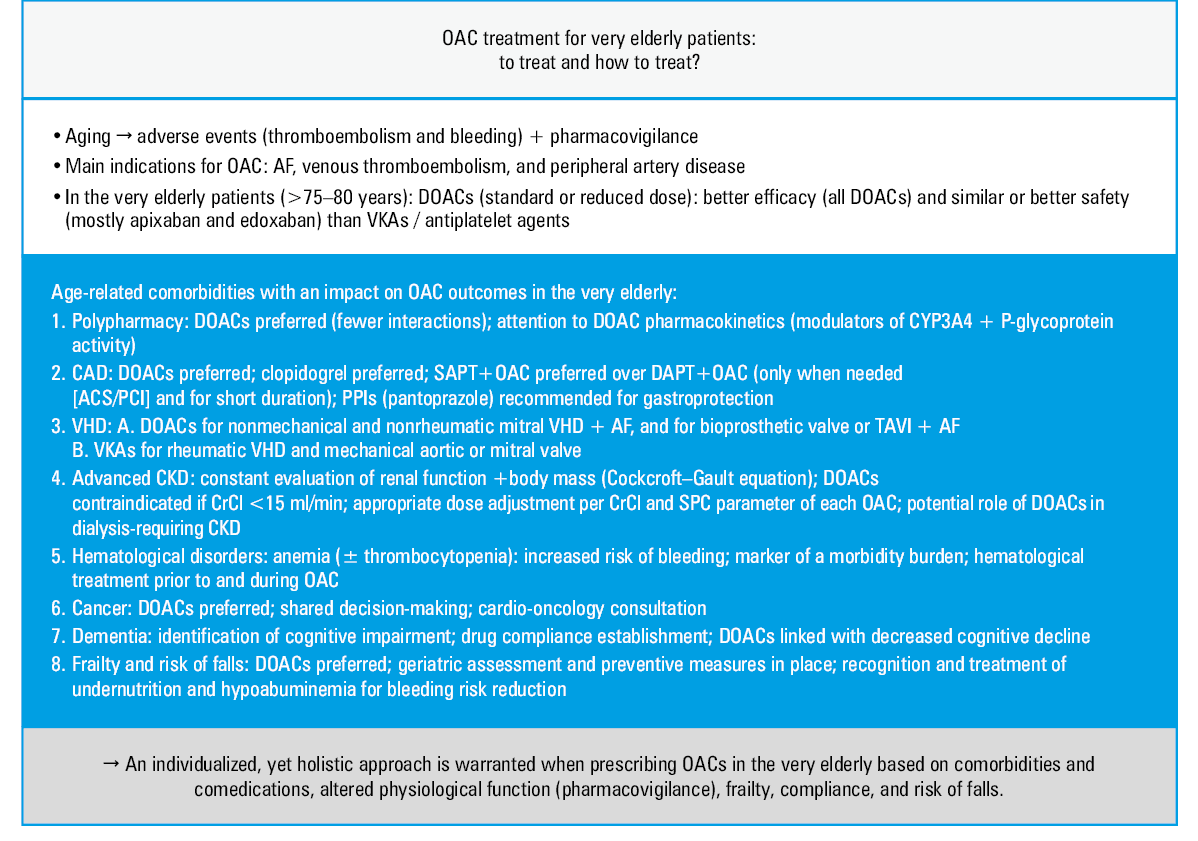
Abbreviations: ACS, acute coronary syndrome; CAD, coronary artery disease; CKD, chronic kidney disease; CrCl, creatinine clearance; CYP, cytochorme P450; DAPT, dual antiplatelet treatment; PCI, percutaneous coronary intervention; PPI, proton pump inhibitor; SAPT, single antiplatelet treatment;
SPC, summary of product characteristics; TAVI, transcatheter aortic valve implantation; VHD, valvular heart disease; others, see Table 3- Patti G, Lucerna M, Pecen L, et al. Thromboembolic risk, bleeding outcomes and effect of different antithrombotic strategies in very elderly patients with atrial fibrillation: a sub‑analysis from the PREFER in AF (PREvention oF Thromboembolic Events‑European Registry in Atrial Fibrillation). J Am Heart Assoc. 2017; 6: e005657. | Crossref
- Hindricks G, Potpara T, Dagres N, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio‑Thoracic Surgery (EACTS): the Task Force for the diagnosis and management of atrial fibrillation of the Europe. Eur Heart J. 2021; 42: 373‑498.
- Steg PG, Huber K, Andreotti F, et al. Bleeding in acute coronary syndromes and percutaneous coronary interventions: position paper by the Working Group on Thrombosis of the European Society of Cardiology. Eur Heart J. 2011; 32: 1854‑1864. | Crossref
- Singh S, Bajorek B. Defining ‘elderly’ in clinical practice guidelines for pharmacotherapy. Pharm Pract. 2014; 12: 489. | Crossref
- Khan SS, Singer BD, Vaughan DE. Molecular and physiological manifestations and measurement of aging in humans. Aging Cell. 2017; 16: 624‑633. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION