Permanent single-chamber atrial pacing: an obsolete or viable alternative to dual-chamber pacing in selected patients with sinus node disease?
Key words: atrial fibrillation, atrial pacing, atrioventricular block, sick sinus syndrome



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Permanent single-chamber atrial pacing: an obsolete or viable alternative to dual-chamber pacing in selected patients with sinus node disease?
Introduction: Single atrial stimulation (AAI) has been commonly used for permanent pacing in sick sinus syndrome and significant bradycardia.
Objectives: The study aimed to evaluate long‑term AAI pacing and to identify timing and reasons for pacing mode change.
Patients and methods: Retrospectively, we included 207 patients (60% women) with initial AAI pacing, who were followed‑up for an average of 12 years.
Results: At the time of death or loss to follow‑up, 71 patients (34.3%) had unchanged AAI pacing mode. The reason for an upgrade of the pacing system was development of atrial fibrillation (AF) in 43 patients (20.78%) and atrioventricular block (AVB) in 34 patients (16.4%). The cumulative ratio for a pacemaker upgrade reoperation reached 2.77 per 100 patient‑years of the follow‑up. Cumulative ventricular pacing below 10% after an upgrade to dual‑chamber pacemaker was observed in 28.6% of the patients. Younger age at implant was the leading independent predictor of the change to dual‑chamber simulation (hazard ratio, 1.98; 95% CI, 1.976–1.988; P = 0.001). There were 11 (5%) lead malfunctions that required reoperation. Subclavian vein occlusion was noted in 9 upgrade procedures (11%). One cardiac device–related infection was observed.
Conclusions: The reliability of AAI pacing decreases with each year of observation due to development of AF and AVB. However, in the current era of effective AF treatment, the advantages of AAI pacemakers, such as lower incidence of lead malfunction, venous occlusion, and infection, as compared with dual‑chamber pacemakers, may make AAI pacemakers a viable option.
What's new?
Sick sinus syndrome or sinus node dysfunction is a common heart rhythm disorder in everyday internal medicine practice. Over 10 years ago, single atrial stimulation (AAI) was commonly used, but after the DANPACE study, it became a second choice to dual‑chamber pacemakers. As a result, the AAI mode has become obsolete as the primary implantation choice. However, some patients with these pacemakers are still alive and benefit from this pacing mode. The most common reason for pacing mode change is development of atrial fibrillation (AF). A decade after the DANPACE trial, with improved access to and effectiveness of AF ablation, the role of AAI pacing in heart rhythm management should be reconsidered. We present the longest follow‑up to date, lasting on average for 12 years, in a large group of patients with de novo AAI pacing mode, and provide a detailed analysis of pacing mode changes and complications. Additionally, we retrospectively examine the reasons for the change from the AAI pacing mode.
Introduction
Until 2011, it was uncertain which device, single‑lead atrial pacemaker (AAI) or dual‑chamber pacemaker (DDD), was the superior treatment option for patients with sinus node disease (SND). The choice of pacemaker type depended largely on the presence or absence of atrioventricular (AV) disturbances or the Wenckebach point rate higher than 120 bpm, which favored dual‑chamber pacing.1 However, the DANPACE trial (Danish Multicentre Randomized Trial on Single Lead Atrial Pacing vs Dual Chamber Pacing in Sick Sinus Syndrome)2 shifted this choice toward the DDD pacemaker, as it showed that AAI pacing was associated with higher incidence of paroxysmal atrial fibrillation (AF) and a 2‑fold increased risk of the pacemaker reoperation.
In 2013, following the publication of the European Society of Cardiology on pacing guidelines, AAI pacing became the second or even third choice in the SND treatment algorithm.3 While the DANPACE study found no differences between DDD rate modulation (R) and AAI(R) pacing in all‑cause mortality, the risk of undergoing the pacemaker reoperation was twice as high in the AAI(R) group than in the DDD(R) group, mainly due to AV block (AVB).1 Additionally, the authors found higher incidence of paroxysmal AF in AAI, as compared with the DDD mode, which was an unexpected finding given the results of a previous randomized controlled trial.4 The results obtained retrospectively in our center and published in 2013 were similar to those of DANPACE in terms of a higher risk of the pacemaker reoperation.5
Although AAI pacing is often termed the forgotten pacing mode, it is still used in selected patients with sick sinus syndrome (SSS) and appears beneficial in some clinical conditions.6 Evidence on prolonged follow‑up outcomes may help identify patient groups who benefit from the single‑lead atrial pacing.7-9 In this study, we report an extended observation of patients with AAI pacemakers to assess durability of this pacing mode.
Unlike in many other AAI trials and retrospective observational studies,1,4,7,8 the present retrospective analysis focuses on a permanent loss of the AAI pacing system during extended follow‑up of over 10 years. We aimed to identify the causes of AAI pacing mode change, such as development of permanent AF, AVB, endocavitary lead malfunction, and infections. Additionally, we demonstrate patient characteristics that predict uninterrupted use of AAI pacing.
Patients and methods
We examined the medical records of all consecutive patients (n = 254) who underwent AAI implantation at St. John Paul II Hospital in Kraków, Poland, between January 1995 and December 2019. Inclusion criteria required the patients to have at least 1 postimplant clinic visit per year until death or July 2020, resulting in 207 patients being included. The patients were excluded if they were lost to follow‑up or transferred to another pacemaker center. Indications for AAI pacing were based on a diagnosis of SND and the Wenckebach point measurement over 120 bpm.2 We gathered the information for this study from the electronic database Impuls‑BIS (ITAM, Zabrze, Poland) and IMPULS records of outpatient clinics and operative reports. The reviewed information included patient demographics, implantation date, reoperation date, development of AF or AVB, lead dysfunction, venous occlusion during reoperation, and pacemaker infections. It is worth noting that the ratio of AAI to DDD pacing for SND patients at the Electrocardiology Department of St. John Paul II Hospital in Kraków was 1 to 3.5 between 2000 and 2010.
Ethics statement
The study was approved by the institutional review board (NB.0710.012.2022). The need for informed consent was waived due to the retrospective nature of the work.
Statistical analysis
The data were presented as numbers and percentages for categorical variables, with means and SD for normally distributed continuous variables or medians and interquartile ranges (IQRs) for continuous variables with a non‑normal distribution. The normality of the data distribution was verified with the Kolmogorov–Smirnov test. The χ2 test or the Fisher exact test was used to analyze categorical variables. Normally distributed continuous variables were compared using the t test, and non‑normally distributed variables were compared using the Mann–Whitney test.
Graphic presentation of the long‑term AAI mode survival is depicted with the Kaplan–Meier curves, which were compared using the log‑rank test. In addition, the univariable Cox proportional hazards model was used to test the effects of clinically significant predictors of AAI mode change. Finally, the χ2 Cochran–Armitage test was used for trend analysis.
The pacing mode change incidence rate was presented as the number of events per 100 patient‑years of follow‑up.
All statistical tests were 2‑tailed, and a P value below 0.05 was considered significant. All the analyses were performed with IBM SPSS Statistics for Windows package, version 25.0 (IBM Corp., Armonk, New York, United States).
Results
From 1995 to 2019, a total of 254 patients received de novo AAI pacemaker implant in our center. Of those, 47 individuals were lost to follow‑up and were excluded from the analysis. We analyzed data from 207 patients with a median follow‑up of 12.2 years (IQR, 6.4–18.6; max. 31.6 years) (P<0.001). The mean (SD) patient age at implantation was 62.3 (13.5) years, and 60.4% of the participants were women. Table 1 presents the patient characteristics and comorbidities.
Parameter | Value |
Data are presented as number (percentage) or median (interquartile range) unless indicated otherwise.
Abbreviations: AAI, atrial chamber pacemaker; AF, atrial fibrillation; IFG, impaired fasting glycemia; LVEF, left ventricular ejection fraction | |
Age, y, mean (SD) | 62.3 (13.5) |
Women | 125 (60.4) |
Duration of follow‑up, y | 12.15 (6.4–18.6); max, 31.6 |
Time to mode change from initial AAI, y | 7.8 (5.1–9.9) |
Comorbidities at the initial evaluation | |
History of paroxysmal AF | 56 (27.1) |
Hypertension | 161 (77.8) |
Diabetes mellitus / IFG | 47 (22.7) |
Reduced LVEF <50% | 12 (5.8) |
Ischemic heart disease | 76 (36.7) |
During the study period, 128 patients (61.83%) had no pacing mode changes, while 79 (38.2%) underwent a mode change to DDD and single ventricular pacing mode (VVI) or received an implantable cardioverter defibrillator (ICD). Seventy‑one patients (34.3%) died during the study period. The AAI mode survival rate at 1, 5, 10, and 15 years was 99%, 91%, 72%, and 66%, respectively. The median time to mode change was 7.8 years (IQR, 5.1–9.9). The first battery replacement without pacing mode change was performed in 119 patients, the second in 48 patients, and 4 underwent a third AAI generator change. Distribution of the pacemaker events in time was not linear, with significantly more frequent mode change until the first replacement (P = 0.005). A detailed flowchart representing the pacemaker replacements and other events is presented in Figure 1.
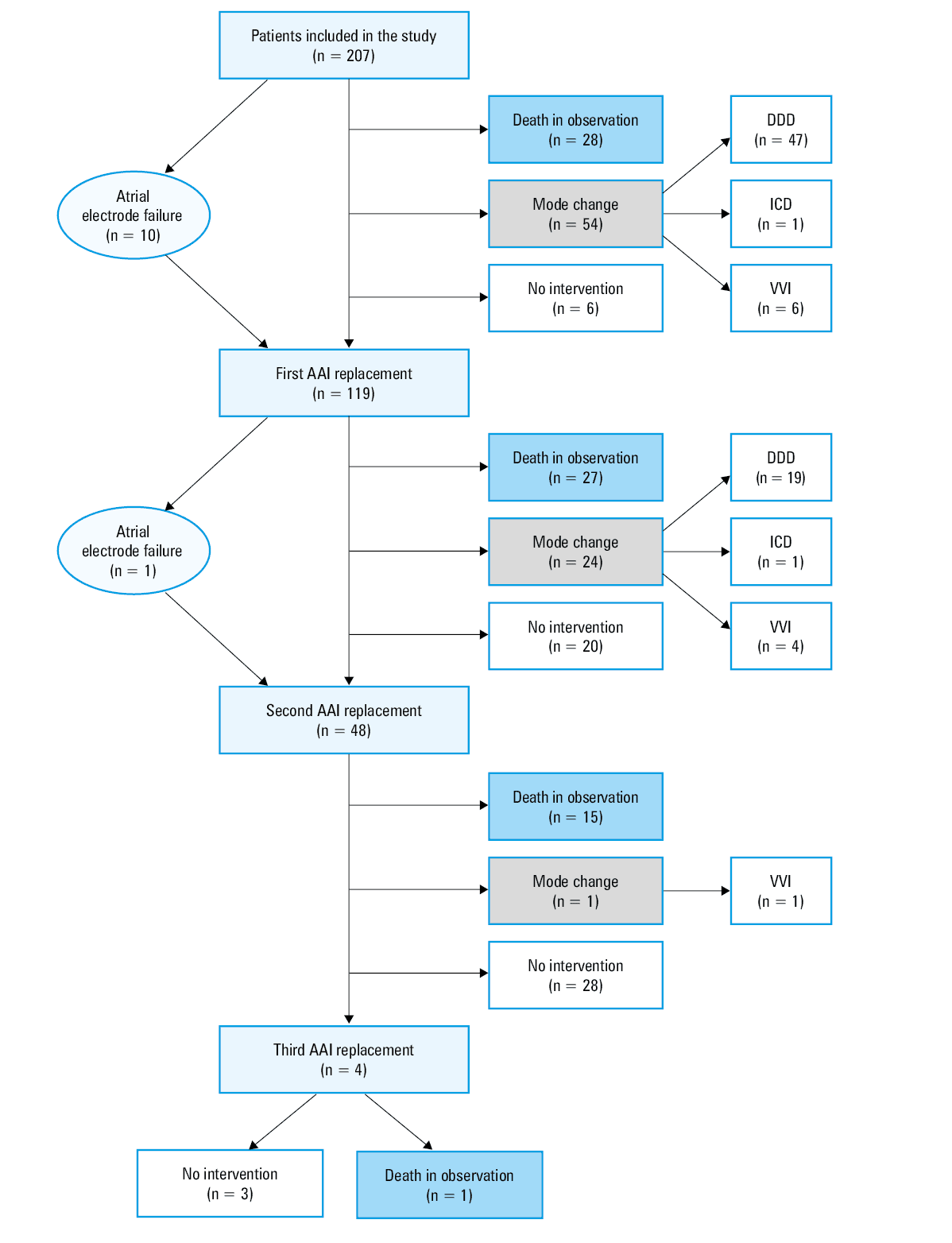
Abbreviations: DDD, dual‑chamber pacemaker; ICD, implantable cardioverter‑defibrillator; VVI, single ventricular pacing mode; others, see Table 1
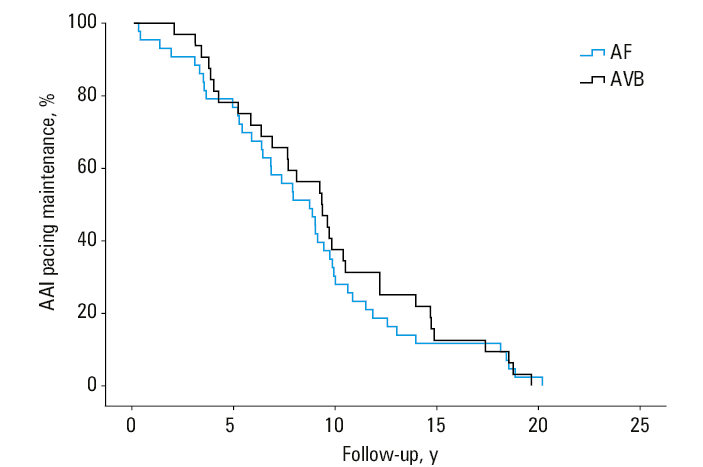
Of the 79 patients who required mode change, 77 had pacing ventricular lead implantation (66 commenced DDD pacing, and 11 were switched directly to VVI mode), and 2 were upgraded to an ICD. Specifically, in 43 patients (1.55 per 100 patient‑years of follow‑up), development of persistent AF with a slow ventricular rate necessitated an upgrade, with a median time to mode change of 7.86 years (IQR, 5.3–10.1). Additionally, 34 patients (1.22 per 100‑patient‑years of follow‑up) required an upgrade due to AVB, with a median time of 7.62 years (IQR, 3.9–9.8). Among the patients with AF, 11 (14%) had their pacing mode changed directly to VVI mode. Lastly, 2 patients (2.5%) required implantation of a defibrillator lead due to development of heart failure. Overall, the rate of reoperation reached 2.77 per 100 patient‑years. The Kaplan–Meier survival curves for AAI mode are presented in Figure 2.
Abbreviations: AVB, atrioventricular block; others, see Table 1
Subclavian vein stenosis was encountered at the device upgrade in 9 patients (11.4%). In addition, we noted an association between venous occlusion and elderly age (age bracket, 75–81 years; P = 0.05) and an indication for mode change (AVB vs AF; P <0.001).
Lead failure was diagnosed in 11 cases, accounting for 5.3% of the patients (0.55 per 100 patient‑years). The implantation technique was as follows: 112 leads (54%) were implanted via cephalic vein venesection, and 95 leads (46%) via a subclavian puncture. The subclavian puncture was associated with mechanical damage of the atrial lead (P = 0.003). Lead complications occurred mainly among women of younger age (P = 0.005). The median time to lead damage was 6.15 years (IQR, 4.8–8.4). All dysfunctional electrodes were extracted.
Two patients (1%) required implantation of an ICD due to progression of heart failure. We observed a single case of local infection but no instances of infective endocarditis. Table 2 presents all cases in which the patients required pacemaker reoperation.
Parameter | Value |
Deaths during follow‑up with AAI pacing, n (incidence per 100 person‑years) | 71 (3.52) |
AAI mode without intervention, n (%) | 128 (61.83) |
AAI mode requiring change, n (%) | 79 (38.16) |
AVB with mode change, n (incidence per 100 person‑years) | 34 (1.22) |
AF with mode change, n (incidence per 100 person‑years) | 43 (1.55) |
Total of mode change from AAI to DDD or VVI, n (incidence per 100 person‑years) | 77 (2.77) |
Mode change from AAI to DDD, n (%) | 66 (83.54) |
Mode change from AAI to VVI, n (%) | 11 (13.92) |
Total of mode change from AAI to ICD, n (%) | 2 (0.97) |
Atrial lead failure, n (%); incidence per 100 person‑years | 11 (5.3); 0.55 |
Subclavian vein occlusion, n (%) | 9 (11.39) |
Median time to lead failure, y (IQR) | 6.15 (4.8–8.4) |
Infection related to the pacing system, n (%) | 1 (0.48) |
Median ventricular pacing burden after an upgrade procedure, % (IQR) | 42.3 (0–96.5) |
Patients without ventricular stimulation after an upgrade procedure, n (%) | 22 (28.6) |
The Cox univariable analysis was conducted to identify risk factors for the loss of AAI due to AF or AVB. Age was found to be a significant predictor, with each additional year the risk of AF growing by 6% (hazard ratio [HR], 1.061/y; P <0.001) and the risk of AVB by 3.6% (HR, 1.036/y; P = 0.03). Additionally, a history of paroxysmal AF at the time of implantation was a significant predictor of AF (HR, 11.3; P <0.001). Other factors did not have a significant impact on AAI pacing mode change. Table 3 presents detailed data from the Cox regression analysis.
Parameter | HR | 95% Cl | P value |
Univariable analysis for the development of AF | |||
Age (per year) | 1.061 | 1.03–1.09 | <0.001 |
Sex | 0.876 | 0.49–1.56 | 0.66 |
Hypertension | 1.037 | 0.52–2.08 | 0.92 |
Diabetes mellitus | 1.253 | 0.69–2.26 | 0.45 |
Paroxysmal AF | 11.312 | 5.21–24.57 | <0.001 |
Heart failure | 1.456 | 0.58–2.08 | 0.43 |
Ischemic heart disease | 0.698 | 0.422–1.198 | 0.46 |
Univariable analysis for the development of AVB | |||
Age (per year) | 1.036 | 1.004–1.069 | 0.03 |
Sex | 1.629 | 0.824–3.223 | 0.16 |
Hypertension | 0.914 | 0.388–2.154 | 0.84 |
Diabetes mellitus | 0.6 | 0.231–1.56 | 0.3 |
Heart failure | 2.088 | 0.722–6.04 | 0.17 |
Ischemic heart disease | 0.702 | 0.502–1.212 | 0.61 |
Univariable analysis for pacing mode change combined for AF and AVB | |||
Age (per year) | 1.982 | 1.976–1.988 | <0.001 |
Our analysis of the upgrade procedure indications revealed that 19 patients (9.2%) had symptomatic bradycardia. The ventricular pacing burden in medical files ranged from 0% to 100%, with a median of 42.3% (IQR, 0%–96.5%). During DDD follow‑up, 21 patients (27.3%) experienced over 90% cumulative ventricular stimulation, while 22 patients (28.6%) had less than 10% of ventricular stimulation at the last check‑up. Data were retrieved from pacing devices to evaluate the percentage of pacing burden. Available Holter monitoring recordings indicated that ventricular stimulation mainly occurred at night, and many patients did not report any differences after the mode change.
Discussion
AAI pacing, which is primarily used to treat SND, is usually continued during generator reimplantation. Although this type of stimulation is beneficial in preventing unnecessary ventricular stimulation, lead‑related tricuspid regurgitation, or valve degeneration, the risk of reoperation increases significantly in the long run. The DANPACE study demonstrated that the risk of reoperation and AAI pacing mode change increased significantly from 2.3%/y in a 5.4‑year observation to 4.5%/y in an 8.9‑year observation.7 Our previous study found that the annual risk of reoperation to change the pacing mode (from AAI) was 1.61 per 100 patient‑years for a mean (SD) follow‑up of 4.3 (2.08) years, which increased to 2.77 per 100 patient‑years in over 12 years of observation.4 The AAI mode survival rate significantly decreased from 91% to 72% between 5 and 10 years of observation (Figure 1). In comparison with a similar study on patients with DDD mode, with a survival percentage change from 86% to 77% in AAI between 5 and 10 years of observation, the change we observed can be considered abrupt.10 The change between 10 and 15 years of observation was significantly smaller (from 72% to 66%) (P = 0.005), indicating reduced incidence of mode change over a more extended observation.
The primary reasons for AAI mode change are AF and AVB. In both cases, age remains the primary, independent predictor, with a generally increased risk of reoperation for this predictor reaching 4.3% per year, 6% in the case of AF development and 3.6% in the case of AVB block development. The incidence of AF development was higher because many patients had a history of paroxysmal AF that is inherently associated with SSS. The median time to the AAI mode change was 7.8 years.
According to the presented results, a decision about the pacemaker mode change in the case of asymptomatic patients who had developed AF or AVB was usually delayed until the pacemaker battery end of life. However, publications analyzing the results from DANPACE study raised an important issue stating that changing the pacing mode accounts for only one‑third of the reasons for reoperation.7 Therefore, operators usually use the time before the battery replacement to reconsider indications—atrial high rhythms in the device memory or AV disturbances found on Holter monitoring immediately after ventricular lead implantation.
In retrospect, however, upgrading to a dual‑chamber pacemaker in such circumstances appears inappropriate, considering the present guidance for AF ablation.11 While treatment of AVB requires ventricular stimulation, preventing AF and de‑escalating β-blocker therapy might have prevented many of these cases from pacing upgrade. When the atrial high rate episodes appeared in the memory of the pacemaker, pharmacologic treatment was escalated, and the antiarrhythmic drugs were introduced, which also often affected AV conduction.12 Also, evaluating the necessity of initiating oral anticoagulant therapy was desirable.13
The percentage of ventricular stimulation after an upgrade procedure shows that the pacing burden ranges from 0% to 100% with a median of 42.3% (IQR, 0%–96.5%). Almost 30% of the patients had minimal (<10%) ventricular stimulation, while 27.3% had a high burden of ventricular pacing. In other cases, an insightful evaluation of Holter monitoring after the pacing improvement revealed that ventricular stimulation mainly occurred at night, and the patients generally did not report any differences after the mode modification. Interestingly, the number of patients with a high percentage of ventricular stimulation (>50%) almost doubled—from 19 symptomatic individuals before the upgrade to 34 in follow‑up. One local infection was observed, however, during such an extended time of observation and substantial loss of patients to the follow‑up this may be underestimated.
It is also worth mentioning that 3 patients from the upgraded group (n = 77) underwent an interventional procedure for ventricular lead complications. One patient experienced ventricular perforation, the second developed severe tricuspid valve regurgitation due to device‑related endocarditis, and the third suffered from ventricular lead failure.
During the observation period, 11 atrial leads (5.3%) failed to meet the criteria. The risk of lead failure in single‑lead pacing was found to be about 50% lower than in dual‑chamber pacing, since only 1 lead is implanted.14 In a previous study on DDD pacing from our center, lead‑related complications occurred in 11.3% of implanted leads in a similar follow‑up period.10 The median time to atrial lead failure was estimated to be 6.2 (IQR, 4.8–8.4) years, which was similar to another study (80.1 months).15
Lead failure mostly occurs before the first reimplantation, and younger patients have a significantly higher likelihood of this complication. The main technique‑dependent predictor affecting lead failure was the subclavian puncture, which was also observed in a previous study.14 Subclavian vein occlusion was found in 9 upgrade procedures (11.4%), and occurred in older patients, while the patients with paroxysmal AF and on oral anticoagulants experienced this condition significantly less often than those with AVB. The reported incidence of stenosis in AAI systems differs considerably from multielectrode cardiac devices, where the average incidence is 27%.16-19Only 1 case of infection was observed in more than 12 years of observation, which is significantly different from the infection rates in dual‑chamber pacemakers or ICD devices.
Depending on how we look at AAI stimulation, either from the perspective of reducing lead‑related complications or the high risk of an upgrade to dual pacing, the AAI mode may have supporters and critics. Historically, the AAI mode was mainly chosen in younger patients to treat SSS, but this study shows that young age at implantation is the strongest indicator of an upgrade procedure during observation. The results suggest that the AAI mode could benefit older patients, especially octogenarians without a history of paroxysmal AF and AV disturbances. Therefore, the indications for AAI in SSS should be reconsidered in the era of widely available AF ablation.
Study limitations
The main limitation of this study is its retrospective design, which may have influenced the results due to selection bias. The lack of information on the effect of drugs on the patients over the long observation period is another limitation. Also, such a long observation period and substantial loss of patients during follow‑up may lead to bias in the final results. Despite these limitations, the large sample size and long follow‑up period of the study make the results generalizable.
Conclusions
Extended follow‑up in AAI mode demonstrates the age‑related necessity for upgrading pacing systems. AAI reliability was diminished after 10 years from implantation. A decision to upgrade to dual‑chamber pacing should be made with caution based on the presence of paroxysmal AF or weakening AV conduction. While development of persistent AF with slow ventricular rate and higher grade AVB showed similar incidence over the study observation time, we hypothesize that AF ablation may reduce the need for AAI upgrade procedures.
- Haywood GA, Ward J, Ward DE, Camm AJ. Atrioventricular Wenckebach point and progression to atrioventricular block in sinoatrial disease. Pacing Clin Electrophysiol. 1990; 13: 2054‑2058. | Crossref
- Nielsen JC, Thomsen PE, Højberg S, et al. A comparison of single‑lead atrial pacing with dual‑chamber pacing in sick sinus syndrome. Eur Heart J. 2011; 32: 686‑696. | Crossref
- Brignole M, Auricchio A, Baron‑Esquivias G, et al. 2013 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: the Task Force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA). Eur Heart J. 2013; 34: 2281‑2329. | Crossref
- Kristensen L, Nielsen JC, Mortensen PT, et al. Incidence of atrial fibrillation and thromboembolism in a randomized trial of atrial versus dual chamber pacing in 177 patients with sick sinus syndrome. Heart. 2004; 90: 661‑666. | Crossref
- Kuniewicz M, Rydlewska A, Karkowski G, et al. Effectiveness of atrial versus atrioventricular pacing for sick sinus syndrome during long‑term follow‑up. Kardiol Pol. 2015; 73: 7‑16. | Crossref
ARTICLE INFORMATION