Prevalence and assessment of risk factors among Polish adults with post–COVID-19 syndrome: a 12-month follow-up study
Key words: long COVID, long-term sequelae, post-COVID syndrome, risk factors, SARS-CoV-2



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Prevalence and assessment of risk factors among Polish adults with post–COVID-19 syndrome: a 12-month follow-up study
Introduction: Previous studies have indicated that COVID‑19 symptoms may persist for up to 12 months after recovery; however, data on this phenomenon are still limited.
Objectives: The aim of this study was to assess the prevalence, the most common symptoms, and the risk factors for development of post‑COVID syndrome in hospitalized and nonhospitalized patients during a 12‑month follow‑up after recovery from COVID‑19.
Patients and methods: This longitudinal study was based on medical data collected at follow‑up visits at 3 and 12 months post–COVID‑19. Sociodemographic data, chronic conditions, and the most common clinical symptoms were assessed. A total of 643 patients were enrolled in the final analysis.
Results: A majority of the study group were women (63.1%), and the median age of the entire group was 52 years (interquartile range [IQR], 43–63). After 12 months, a median of 65.7% (IQR, 62.1%–69.6%) of the patients declared the presence of at least 1 clinical symptom of post‑COVID syndrome. The most common complaints were asthenia (median, 45.7% [IQR, 41.9%–49.6%]) and neurocognitive symptoms (median, 40% [IQR, 36%–40.1%]). In a multivariable analysis, female sex (odds ratio [OR], 1.49; P = 0.01) and severe COVID‑19 course (OR, 3.05; P <0.001) were associated with persistence of clinical symptoms for up to 12 months after recovery.
Conclusions: After 12 months, persistent symptoms were declared by 65.7% of the patients. The most common symptoms 3 and 12 months after the infection were worse tolerance to exercise, fatigue, palpitations, and memory or concentration problems. Women are at a higher risk of experiencing persistent symptoms, and COVID‑19 severity was a predictor of persistent post–COVID‑19 symptoms.
What's new?
Post–COVID‑19 syndrome is a condition that is not fully understood. Our work is the largest Polish longitudinal study assessing the presence of symptoms 3 and 12 months after recovery from SARS‑CoV‑2 infection in hospitalized patients and patients treated for COVID‑19 at home. Our results indicate that a significant percentage of patients have persistent symptoms in various organs and systems 12 months after the infection. Treatment of post–COVID‑19 complications should be handled by a multispecialty team. This study also shows that the nonhospitalized patients may still experience symptoms 3 and 12 months after recovery from COVID‑19, especially in the cases of a severe course of the disease.
Introduction
According to data from the World Health Organization (WHO), by January 2023, 672 million confirmed cases of COVID‑19 and 6.9 million of COVID‑19–related deaths had been reported worldwide.1 In Poland, the disease has affected over 6.4 million people, and caused at least 125 000 deaths.2 Many patients who contracted COVID‑19 have fully recovered; however, some people have experienced persistent symptoms of variable intensity and duration.3
Available data show that around a quarter of people who contracted COVID‑19 experienced persistent symptoms that lasted for at least 4 weeks, while 10%–20% of the patients experienced symptoms that lasted for more than 12 weeks.4,5 A Polish observational study of post–COVID‑19 patients confirmed persistent symptoms in over 30% of hospitalized and nonhospitalized individuals.6 In response to this, new disease entities have been introduced in medicine, namely long COVID and post–COVID‑19 syndrome. According to the WHO definition, symptoms of SARS‑CoV‑2 infection lasting for more than 4 weeks are called long COVID, and the post–COVID‑19 syndrome is defined as a constellation of long‑term symptoms (lasting for at least 2 months) that occur within 3 months from the onset of COVID‑19 and cannot be explained by another disease.7 Post–COVID‑19 syndrome can manifest in approximately 200 different and overlapping symptoms, such as fatigue, as well as sensory, neurologic, musculoskeletal, dermatologic, respiratory, and cardiovascular symptoms.8 Persistent ailments have a negative impact on patient cognitive functions, daily functioning, quality of life, and return to work, which, in the future, may have serious economic consequences for the society.9,10
As the COVID‑19 pandemic progresses, awareness of the disease’s long‑term effects grows steadily.10 The literature data are inconclusive and the range of reported symptoms varies from 10% to 80% of patients.4,5,9 Some authors suggest that after 12 months of observation, as many as 77.1% of patients report persistent symptoms, including reduced physical tolerance (56.3%), fatigue (53.1%), dyspnea (37.5%), concentration problems (39.6%), and sleep disturbances (26%). On the other hand, in a 12‑month follow‑up study by Comelli et al,11 persistent symptoms were found in 91.7% of the respondents, with the most common being exercise dyspnea, fatigue, and gastrointestinal symptoms. Likewise, a recent systematic review and meta‑analysis12 found that many physical and mental health problems, as well as problems with cognitive functions, persist for at least a year in a significant proportion of those with confirmed COVID‑19.
To date, little is known about risk factors for long‑term persistence of COVID‑19 symptoms. The studies conducted so far show that persistence of long‑term symptoms is often associated with their exacerbation in an acute phase of the disease; however, long‑term symptoms may affect patients with both mild and severe COVID‑19, and may occur in all age groups.13-16 A worrying sign are the data collected over a 2‑year follow‑up, with one‑third of mostly nonhospitalized COVID‑19 patients still experiencing persistent symptoms after an acute infection, despite a relatively mild disease course in the initial stage.17 Therefore, the aim of this study was to assess the prevalence, most common symptoms, and risk factors for development of post–COVID‑19 syndrome in hospitalized and nonhospitalized COVID‑19 patients during 12‑month follow‑up after recovery from SARS‑CoV‑2 infection.
Patients and methods
Research methodology
This is a longitudinal study based on the analysis of data collected at face‑to‑face medical visits from patients registered in the Polish STOP‑COVID registry (ClinicalTrials.gov: NCT05018052). This registry includes patients with confirmed COVID‑19, followed by a physician to carefully evaluate their health status after the disease. As part of the study, each patient attended 3 medical appointments: during the infection, and 3 and 12 months after recovery.
The study inclusion criteria comprised confirmed diagnosis of COVID‑19 (positive polymerase chain reaction test and / or antigen test according to the European case definition of COVID‑19,18 age of at least 18 years, written consent to participate in the study, and 2 follow‑up visits at 3 and 12 months after COVID‑19.
Before taking part in the study, the patients received comprehensive information on its objectives and methodology, and gave their written informed consent to participate. The study was conducted according to the guidelines of the Declaration of Helsinki and was approved by the Bioethics Committee of the Wroclaw Medical University, Poland (232/2022).
At the medical visits, the patients provided their sociodemographic data, including age and sex. Anthropometric measurements (weight and height) were used to calculate their body mass index (BMI). In addition, the interview was supplemented with information about chronic diseases, such as hypertension, diabetes, hyperlipidemia, heart failure, asthma, and chronic obstructive pulmonary disease (COPD). At the first visit, data on the place of isolation, clinical symptoms during COVID‑19, and their duration were collected. The patients were selected to participate in the study between March 13, 2020 and May 15, 2021. None of the participants had been vaccinated against COVID‑19 before contracting the disease.
Based on the above data, the patients were divided into 5 groups. Group 0 included individuals without clinical symptoms or with symptoms lasting up to 3 days; group 1 comprised patients treated at home with symptoms lasting up to 7 days; group 2 were patients treated at home with symptoms lasting from 7 to 14 days; group 3 incorporated patients treated at home with symptoms lasting for at least 14 days and a fever above 38 °C, dyspnea, and saturation below 94% for at least 3 days, and group 4 included hospitalized patients.
At the follow‑up visits at 3 and 12 months, the patients completed health questionnaires. They reported sustained clinical symptoms 3 and 12 months after the infection. Their ailments were divided into 7 main groups: asthenia (fatigue, worse tolerance to exercise), sensory symptoms (changes in the sense of smell and / or taste), dermatologic symptoms (hair loss, persistent skin changes after illness, excessive sweating), neurocognitive symptoms (headache, impaired concentration and memory), musculoskeletal symptoms (arthralgia, myalgia), respiratory symptoms (shortness of breath, persistent, chronic cough, recurrent chest pain), and cardiovascular symptoms (palpitations / arrhythmias, anginal symptoms, venous thromboembolism, peripheral edema, newly diagnosed arterial hypertension, fainting / unconsciousness).
Categorization decisions were made based on a previous study.19
Statistical analysis
Due to non‑normal distribution, the quantitative variables are presented as medians with interquartile ranges (IQRs). For qualitative variables, the results are presented as numbers (percentage). We estimated 95% CI for the occurrence of symptoms at 3 and 12 months postinfection using the bootstrap method (1000 iterations). Multivariable logistic regression analysis was used to assess the risk factors for persistence of clinical symptoms after the acute phase of COVID‑19 at 12 months. The independent variables included age, sex, BMI, chronic conditions such as hypertension, diabetes, ischemic disease, asthma, and COPD, presence of at least 1 chronic disease, and severity of COVID‑19. Similar models were built for the symptoms most common after 12 months, that is, fatigue and neurologic symptoms. Statistica 13.0 package by StatSoft (Tulsa, Oklahoma, United States) was used for calculations. All tests assumed a statistical significance level of P below 0.05.
Results
Description of the study group
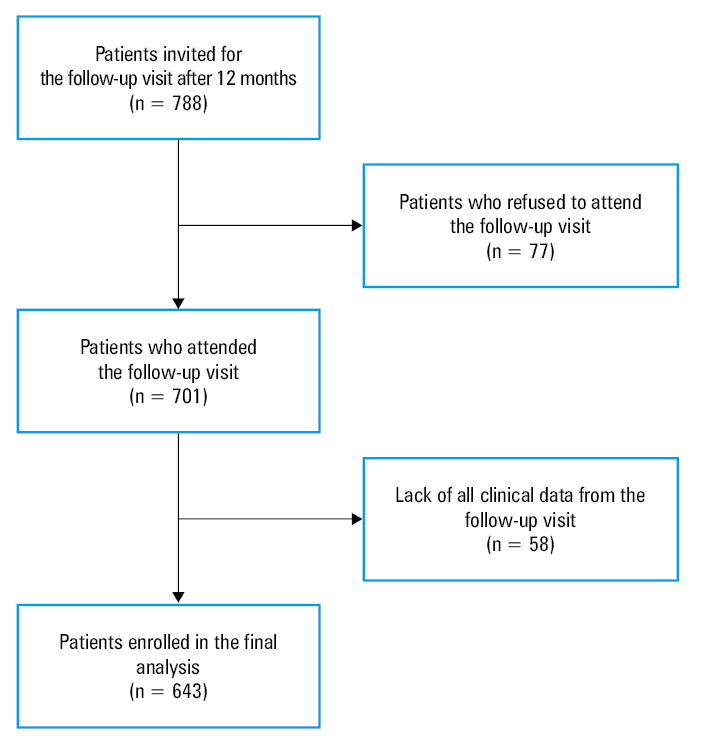
In total, 788 patients were invited for the follow‑up visit after 12 months, of whom 701 (88.9%) agreed to participate. Due to missing data, the final analysis included 643 patients (91.7%). The study flowchart is shown in Figure 1. The study group comprised mostly women (63.1%). Median age of the participants was 52 years (IQR, 43–63). As many as 67.3% of the patients suffered from at least 1 chronic disease, with the most common being hypertension (39.3%), hyperlipidemia (20.5%), and asthma (10.6%). Home was the most frequent place of isolation (83.7%). One hundred and five (16.3%) patients were hospitalized, of whom 88 were diagnosed with pneumonia, and 1 patient was admitted to an intensive care unit. A detailed patient characteristics is presented in Table 1.
Variable | Whole group (n = 643) | Home isolation (n = 538) | Hospitalization (n = 105) | |
Data are presented as number (percentage) or median (interquartile range).
a COVID‑19 severity: 0 – patients without clinical symptoms or with symptoms lasting up to 3 days; 1 – patients treated at home with symptoms lasting up to 7 days; 2 – patients treated at home with symptoms lasting from 7 to 14 days; 3 – patients treated at home with symptoms lasting at least 14 days and fever greater than 38 °C, dyspnea, and saturation <94% for at least 3 days; 4 – hospitalized patients
Abbreviations: BMI; body mass index; COPD, chronic obstructive pulmonary disease | ||||
Sex | Women | 406 (63.1) | 351 (65.2) | 55 (52.4) |
Men | 237 (36.9) | 187 (34.8) | 50 (47.6) | |
Age, y | 52 (43–63) | 52 (43–61) | 62 (51–66) | |
Weight, kg | 80 (67–90.5) | 78 (67–90) | 83 (73–95) | |
Height, cm | 168 (164–176) | 168 (164–176) | 170 (160–170) | |
BMI, kg/m2 | 27.3 (24.2–31.2) | 26.7 (23.9–30.9) | 29.2 (25.7–31.7) | |
Chronic diseases | Hypertension | 253 (39.3) | 198 (36.8) | 55 (52.4) |
Diabetes | 66 (10.3) | 48 (8.9) | 18 (17.1) | |
Coronary artery disease | 31 (4.8) | 24 (4.5) | 7 (6.7) | |
Hyperlipidemia | 132 (20.5) | 106 (19.7) | 26 (24.8) | |
Asthma | 68 (10.6) | 55 (10.2) | 13 (12.4) | |
COPD | 11 (1.7) | 9 (1.7) | 2 (1.9) | |
Any chronic disease | 433 (67.3) | 351 (65.2) | 82 (78.1) | |
COVID‑19 severitya | 0 | 40 (6.3) | 40 (7.4) | – |
1 | 188 (29.2) | 188 (34.9) | – | |
2 | 171 (26.6) | 171 (31.9) | – | |
3 | 139 (21.6) | 139 (25.8) | – | |
4 | 105 (16.3) | – | 105 (100) | |
Clinical picture at 3 and 12 months postinfection
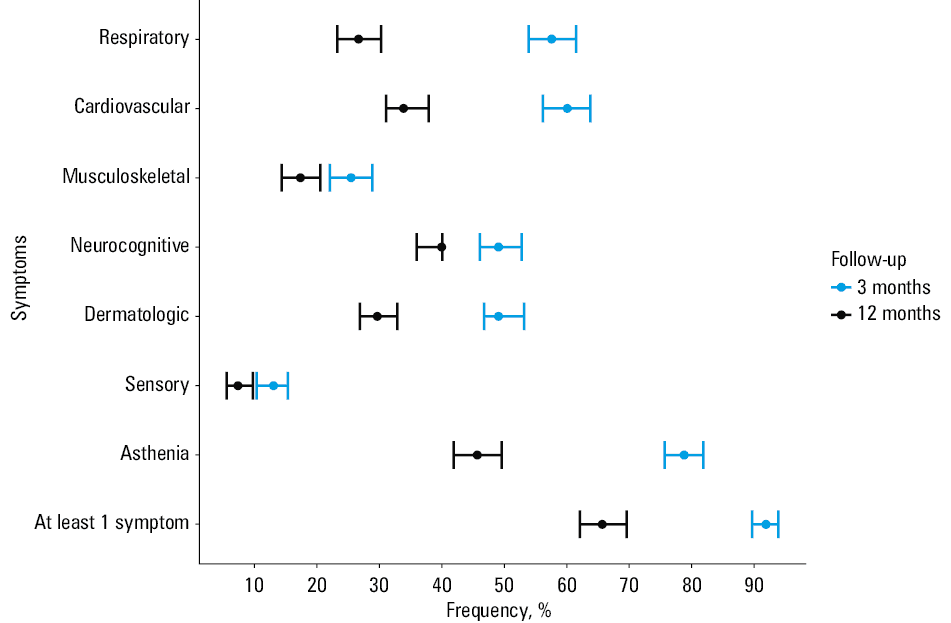
At 3 months after the infection, a high percentage of patients declared the presence of at least 1 clinical symptom (median, 91.9% [IQR, 89.7%–93.9%]), and met the post–COVID‑19 syndrome criteria. This percentage decreased with the duration of follow‑up, and reached a median of 65.7% [IQR, 62%–69.6%] at the 12‑month visit. The most common complaints were related to excessive weakness (median, 45.7% [IQR, 41.9%–49.6%]). At the 12‑month follow‑up visit, as many as 40% of patients (IQR, 36%–40.1%) reported persistent neurologic symptoms, while 33.9% (IQR, 31.1%–37.9%) reported symptoms related to the cardiovascular system. Among individual symptoms, the most common complaints at 3 and 12 months included fatigue (69.2% vs 34.2%), worse tolerance of exercise (62.1% vs 35.7%), palpitations (49.3% vs 23.3%), and memory or concentration problems (44.8% vs 35.7%). Details are presented in Figure 2 and Table 2. The extension of Table 2 is summarized in Supplementary material, Table S1.
Symptoms | Presence of symptoms at 3 months, % (95% CI)a | Presence of symptoms at 12 months, % (95% CI)a |
a Estimated 95% CIs calculated using the bootstrapping method | ||
At least 1 symptom | 91.9 (89.7–93.9) | 65.7 (62.1–69.6) |
Asthenia | 78.8 (75.7–81.9) | 45.7 (41.9–49.6) |
Sensory symptoms | 13.1 (10.4–15.4) | 7.4 (5.6–9.8) |
Dermatologic symptoms | 49.1 (46.8–53.2) | 29.7 (26.9–32.9) |
Neurocognitive symptoms | 49.1 (46.1–52.8) | 40 (36–40.1) |
Musculoskeletal symptoms | 25.5 (22.1–28.9) | 17.4 (14.4–20.6) |
Cardiovascular symptoms | 60.1 (56.2–63.8) | 33.9 (31.1–37.9) |
Respiratory symptoms | 57.6 (53.9–61.5) | 26.7 (23.3–30.3) |
Risk factors of post–COVID‑19 syndrome
The multivariable model of logistic regression analysis showed that female sex and COVID‑19 severity were related to the persistence of clinical symptoms up to 12 months after recovery. In the case of fatigue and impaired exercise tolerance, severe home course of the disease was the leading risk factor. A similar situation was observed for neurologic symptoms, where a severe course of COVID‑19 resulted in a 2‑fold increase in the risk of the symptom persistence. Hospitalization for COVID‑19 did not increase the risk of developing long COVID, fatigue, or brain fog. A detailed summary of the results of the logistic regression analysis is presented in Table 3.
Variable | Post–COVID‑19 at 12 months | Fatigue | Neurocognitive symptoms | |||||||
OR (95% CI) | P valuea | R2 | OR (95% CI) | P valuea | R2 | OR (95% CI) | P valuea | R2 | ||
a Multivariable logistic regression
b COVID‑19 severity, see Table 1
Abbreviations: OR, odds ratio; R2, Nagelkerke R2; others, see Table 1 | ||||||||||
Women | 1.49 (1.04–2.13) | 0.03 | 0.06 | 1.26 (0.89–1.77) | 0.06 | 0.05 | 1.56 (1.09–2.22) | 0.01 | 0.07 | |
Age, y | 0.99 (0.97–1.01) | 0.48 | 0.99 (0.98–1.01) | 0.92 | 1 (0.98–1.01) | 0.66 | ||||
BMI, kg/m2 | 1.01 (0.97–1.04) | 0.73 | 1.01 (0.98–1.04) | 0.38 | 1 (0.97–1.03) | 0.95 | ||||
Chronic
diseases | Hypertension | 1.18 (0.75–1.88) | 0.46 | 1.26 (0.89–1.76) | 0.41 | 1.15 (0.74–1.78) | 0.53 | |||
Diabetes | 0.97 (0.53–1.79) | 0.93 | 0.67 (0.37–1.22) | 0.19 | 0.95 (0.53–1.72) | 0.87 | ||||
Coronary artery disease | 1.42 (0.61–4.22) | 0.41 | 2.04 (0.90–4.52) | 0.08 | 1.62 (0.74–3.55) | 0.22 | ||||
Hyperlipidemia | 1.03 (0.65–1.79) | 0.89 | 1.03 (0.67–1.59) | 0.46 | 1.34 (0.87–2.07) | 0.18 | ||||
Asthma | 0.92 (0.51–1.66) | 0.78 | 1.22 (0.71–2.12) | 0.46 | 1.19 (0.69–2.06) | 0.53 | ||||
COPD | 5.65 (0.51–40.7) | 0.13 | 1.8 (0.49–6.56) | 0.37 | 0.71 (0.44–2.79) | 0.68 | ||||
Any chronic disease | 1.06 (0.62–1.63) | 0.99 | 0.86 (0.54–1.37) | 0.52 | 0.71 (0.44–1.14) | 0.15 | ||||
COVID‑19
severityb | 0 | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | |||
1 | 1.38 (0.68–2.8) | 0.37 | 1.69 (0.82–3.47) | 0.15 | 1.27 (0.61–2.66) | 0.52 | ||||
2 | 1.16 (0.57–2.38) | 0.67 | 1.2 (0.57–2.49) | 0.63 | 1.51 (0.98–3.16) | 0.28 | ||||
3 | 3.05 (1.42–6.56) | 0.004 | 2.76 (1.31–5.84) | 0.007 | 2.09 (0.98–4.45) | 0.048 | ||||
4 | 1.45 (0.67–3.12) | 0.34 | 1.34 (0.62–2.93) | 0.46 | 1.26 (0.58–2.79) | 0.56 | ||||
Discussion
We aimed to assess the most common symptoms and risk factors for development of post–COVID‑19 syndrome in both hospitalized and nonhospitalized patients during 12‑month follow‑up after recovery from SARS‑CoV‑2 infection. This is currently a hot topic and one of the greatest health care challenges, as symptoms may persist for up to 12 months after the infection in 10% to 77% of patients, depending on the data source.5,11,20 Our study covered the first 2 pandemic waves, and included consecutive Polish patients unvaccinated prior to SARS‑CoV‑2 infection. These were patients listed in the Polish STOP‑COVID registry. Of those, 91.9% reported at least 1 persistent COVID‑19–related symptom 3 months after recovery, and this percentage dropped to 65.7% at the 12‑month visit.
This 2‑step follow‑up study allowed us to pinpoint any changes in the symptom frequency over time. For each group of symptoms, their persistence was clearly lower at 12 than at 3 months. The finding is in line with cohort studies by Pazukhina et al19 and Huang et al,21 where a high rate of symptom prevalence observed at 6 months postinfection was reduced at 12‑month follow‑up. We found the greatest decline in persistence from 3rd to 12th month for asthenia, respiratory, and cardiovascular symptoms, while the symptom types with the lowest cessation rate were sensory, musculoskeletal, and neurocognitive symptoms.19 Insights into specific symptoms revealed that the 4 symptom types showing the greatest decline were fatigue, worse tolerance to exercise, palpitations, and chest pain. This was in accordance with the analysis of the groups of symptoms, with the exception of cardiovascular symptoms (palpitations), which showed a sharper decline than the respiratory symptoms (chest pain) but overall a decrease in incidence was also observed.18 In contrast, the specific symptoms with the lowest level of decrease were arthralgia, venous thromboembolism, and fainting, which represented the less common group of sensory symptoms.16,22 Nevertheless, the presence of arthralgia is representative of musculoskeletal symptoms. The same results can be interpreted from another perspective, namely identifying the symptoms with the greatest percentage proportion at 3 and 12 months after recovery. During the first follow‑up visit, asthenia, cardiovascular, and respiratory symptoms were the most prevalent, and partly matched the specific symptoms, that is, fatigue, worse tolerance to exercise, and palpitations.19 There were no specific symptoms that could confirm respiratory symptoms; instead, we observed a high percentage of memory and concentration problems belonging to the group of neurocognitive symptoms. At the second follow‑up visit, asthenia, neurocognitive, and cardiovascular symptoms seemed to reflect the specific symptoms of memory and concentration problems, worse tolerance to exercise, fatigue, and palpitations.23 It is worth noting that only asthenia retained its original prevalence in the general groups of symptoms, encompassing the most often reported ailments.21 However, in the analysis of specific symptoms, the prevalence of this group was overtaken by neurocognitive symptoms, that is, memory and concentration problems, suggesting that frequently reported weakness is displaced by neurologic ailments over the extended observation period.21 Weakness‑related symptoms were also found to be the most common manifestations in other studies,24,25 while a meta‑analysis by Ceban et al26 confirmed that fatigue and cognitive impairment are the most debilitating symptoms of post–COVID‑19 syndrome.
Moreover, this study evaluated the risk factors for developing post–COVID‑19 syndrome. We found out that women were at a higher risk of having persistent neurocognitive symptoms 12 months postinfection. Female sex was identified as a risk factor associated with both long COVID and post–COVID‑19 syndrome.26-28 Interestingly, a multicenter study by Fernández‑de‑Las‑Peñas et al29 revealed that female sex is a risk factor for long‑term post–COVID‑19 symptoms but not for COVID‑19 symptoms. The presence of more persistent symptoms could partly depend on the fact that women are more likely to report their ailments30; this should not be neglected and requires further verification on a larger scale. Moreover, Rudroff et al31 proposed psychophysiological factors (eg, stress, anxiety, depression, pain) as features increasing central factors (eg, inflammation), resulting in greater perception of post–COVID‑19 fatigue among women. Although other authors showed no significant differences between men and women with regard to specific chronic symptom prevalence, the total number of women who needed access to neurology health services determined by Michelutti et al32 was higher than that of men, suggesting higher prevalence of neuro–long‑COVID among women. Ultimately, Nehme et al33 hypothesized that chronification of symptoms might be driven by neurologic manifestations, which might increase with time. This concurs with our observations of women being at a higher risk of neurocognitive symptoms and post–COVID‑19 syndrome, and the fact that patients with moderate COVID‑19 severity (group 3) were at a greater risk of neurocognitive symptoms than those without clinical symptoms, with symptoms lasting up to 7 days, or those hospitalized. The other results of our study also indicate that greater severity of home‑treated COVID‑19 was related to experiencing fatigue and post–COVID‑19 syndrome. Furthermore, as compared with the group with the mildest disease course, fatigue more frequently affected the patients who were treated at home, not hospitalized, and with symptoms lasting up to 7 days. This suggests that a milder disease course can still be associated with persistent fatigue. Previously, we revealed that the greatest disease severity was a predictor of chronic fatigue,15 and a systematic review by Joli et al34 seems to confirm this observation for post–COVID‑19 syndrome (potential risk factor for post–COVID‑19 fatigue was severe clinical status in the acute phase of the infection). However, not all studies are concordant. For example, Townsend et al35 found no association between the severity of acute‑phase symptoms and prevalence of persistent fatigue following COVID‑19, which supports the need for further research. In our study, the hospitalized patients were compared with those without symptoms or with symptoms lasting for up to 7 days, who showed comparable presence of the post–COVID‑19 symptoms at 12‑month follow‑up. Similar research results were obtained by scientists from Spain36 who checked differences in symptoms between hospitalized and nonhospitalized patients in a cross‑sectional study with 2‑year follow‑up after an acute infection.
Our study has some limitations. First, we analyzed patients who self‑referred to a health center due to persistent symptoms after recovery from COVID‑19, that is, not all types of COVID‑19 survivors were included in the study, and the results cannot be extrapolated to the general population. Furthermore, not all chronic conditions have been analyzed, and comorbidities, such as cancer or chronic kidney disease, could have affected the patient condition. Data are also lacking on the use of pharmacotherapy during the disease. During the pandemic, physicians prescribed various antibiotic therapies and antiviral medications. Even if those were found not to improve the course and severity of COVID‑19,37,38 it is possible that their heterogeneous use had an impact on individual patient outcomes. Moreover, the percentages of declared symptoms are very high, because our patients were evaluated for the clinical picture of the disease after 3 and 12 months; typically, symptomless individuals do not attend follow‑up visits. These symptoms were also subjectively assessed, and objective measurements, such as dedicated scales or clinical tests that assess, for example, fatigue or neurocognitive symptoms, should be performed for clarity. It should also be mentioned that some symptoms cannot be categorized into just 1 of the subgroups, for example, chest pain can be a respiratory, cardiovascular, or muscular symptom. In addition, we used self‑defined criteria to assess the severity of COVID‑19. We realize that the method for assessing the severity of COVID‑19 is not validated, however, it has been used in previous publications.13 Moreover, to the best of our knowledge, there are no tools for assessing the severity of COVID‑19 at home. Available scales use laboratory results, which, due to the nature of the study group, we do not have. In addition, attention should be drawn to the limitations arising from the listing of inpatients. It should be remembered that, especially at the early stages of the pandemic, the decision to hospitalize a patient depended rather on the epidemiologic situation than the patient clinical condition. Consequently, hospitalizations without clinical indications were not uncommon. Therefore, the lack of data on the course of hospitalization should also be regarded as a methodological limitation of the study. However, it should be noted that this breakdown into hospitalized and nonhospitalized patients is commonly used in observational studies worldwide.
Despite the aforementioned limitations, the strengths of this study include its longitudinal character with in‑person clinical visits and the follow‑up data that allow for identification of changes in symptom frequency over time.
To conclude, the most common symptoms 3 and 12 months after the infection are worse tolerance to exercise, fatigue, palpitations, and memory or concentration problems. Women are at a higher risk of experiencing persistent symptoms after 12 months. The greatest COVID‑19 severity in nonhospitalized patients was a predictor of post–COVID‑19 syndrome, neurocognitive symptoms, and fatigue; the latter can also be associated with a milder course of the disease. Additionally, a similar rate of post–COVID‑19 symptoms was seen in the hospitalized and nonhospitalized patients. Based on our results, we conclude that post–COVID‑19 syndrome is a common challenge for every health care system and that it potentially affects over 60% of COVID‑19 survivors. However, numerous inconsistencies in research findings still need to be resolved in further studies.
- Living guidance for clinical management of COVID‑19. World Health Organization Available at: https://www.who.int/publications/i/item/WHO‑2019‑nCoV‑clinical‑2021‑2. Accessed October 21, 2022.
- COVID Live—Coronavirus Statistics. Worldometer available at: https://www.worldometers.info/coronavirus/country/poland. Accessed October, 21 2022.
- Antoniou KM, Vasarmidi E, Russell AM, et al. European Respiratory Society statement on long COVID follow‑up. Eur Respir J. 2022; 60: 2102174. | Crossref
- Ma Y, Deng J, Liu Q, et al. Long‑term consequences of COVID‑19 at 6 months and above: a systematic review and meta‑analysis. Int J Environ Res Public Health. 2022; 19: 6865. | Crossref
- Hallek M, Adorjan K, Behrends U, et al. Post‑COVID syndrome. Dtsch Arztebl Int. 2023; 120: 48‑55. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION