Gastric mucormycosis presenting as fever of unknown origin in an immunocompetent host after heatstroke



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Gastric mucormycosis presenting as fever of unknown origin in an immunocompetent host after heatstroke
Mucormycosis is an infectious disease caused by fungi of the order Mucorales, class of Zygomycetes. These are environmental fungi isolated from agricultural or forest soils and from decaying organic matter. They are fast‑growing molds, characterized by large, ribbon‑like hyphae with right‑angle ramification, and with no or few septa.1
Spore inhalation is the primary route of infection; however, other routes of infection have also been described, such as penetration via injured skin or ingestion of spore‑contaminated foods. The disease is then classified according to the site of the fungal invasion into rhino‑orbital‑cerebral mucormycosis, gastrointestinal, pulmonary, cutaneous, or renal mucormycosis, isolated central nervous system involvement, or, eventually, disseminated disease. The rhino‑orbital‑cerebral disease manifestation is, by far, the most frequent, and thus easier to identify. Among the gastrointestinal presentations, the most commonly involved organ is the intestine (64.2%), followed by the stomach (33%). Rhizopus spp. is the principal isolated species, regardless of the site of infection.1,2
Mucormycosis affects patients of all ages, and its incidence is increased in immunocompromised individuals. The most common risk factors for the disease are hematological malignancies (44%), diabetes mellitus (17%), and trauma (17%). The incidence varies between regions, with hematological causes predominating in developed countries, and diabetes and trauma in developing countries.2 Of note, no risk factors are observed in 10% to 19% of cases.2
Treatment is based on a combination of pharmacological and surgical interventions. Amphotericin B is the most commonly used drug, followed by new generation azoles, which are preferred when long‑term treatment is required. Despite increasing awareness and improvement in early diagnosis over the last years, the mortality rate remains greater than 50%. The combination of pharmacological and surgical treatments decreases the mortality rate to 37.3%, as compared with the pharmacological intervention alone, but there is still some reluctance to favor the surgical approach in this clinical setting.3 Particularly in the subset of patients with rhino‑orbital‑cerebral mucormycosis, surgeries tend to have destructive consequences, and usually more than 1 surgical intervention is required to complete the debridement.
In contrast with the rhino‑orbital‑cerebral presentation, the remaining disease types (eg, gastrointestinal) pose a great diagnostic challenge, as they are not typically suspected until microbiological evidence of the infection arises, which usually occurs too late to allow for the initiation of early treatment. In brief, extracranial manifestation of the disease represents a dangerous combination of a very aggressive infection and a delay in effective treatment, usually taking place in a debilitated host. This combination accounts for the poor survival rate and the high number of postmortem diagnoses of mucormycosis in case series.
Here, we present a case of a 53‑year‑old man who was admitted to the intensive care unit (ICU) following a sudden loss of consciousness and hyperthermia. His medical history included only well‑controlled schizophrenia treated with low‑dose quetiapine. He had been found at his workplace (a warehouse) with symptoms of increasing dizziness and stupor; finally, he fainted and did not regain consciousness. Upon arrival of the emergency medical services, he was found to be comatose (Glasgow Coma Scale 8), hypotensive, and tachycardic, with an axillary temperature of 41 ºC. He was intubated and transferred to the hospital. In the emergency room, he was diagnosed with an exertional heatstroke with neurologic injury, circulatory collapse, and multiorgan failure comprising rhabdomyolysis, acute kidney failure with profound metabolic acidosis, pancreatitis, and disseminated intravascular coagulation.
Active cooling was started immediately, along with vasoactive support including high‑dose noradrenaline (0.4 μg/kg/min) and hydrocortisone at stress doses. Also, empiric antibiotic therapy was initiated after blood samples had been collected. Despite the applied treatment, during the following days, the patient needed mechanical ventilation, renal replacement therapy, and enteral nutrition through a nasogastric tube as soon as he reached hemodynamic stability. Finally, at the end of the first week of hospitalization, his condition improved and he started the weaning phase.
On day 12 of hospitalization, the patient developed continuous fever. No pathogenic organisms were isolated in any of the culture tests (blood cultures, urine cultures, tracheal aspirates, and stool samples). Despite increaseing the spectrum of antibiotic therapy and catheter replacements, fever and elevation of acute‑phase reactant concentrations persisted, without an evident reason. Test results for both galactomannan and 1,3-β-d‑glucan biomarkers were negative. Drug fever was also considered as a potential cause of the fever of unknown origin. Thus, antidopaminergics, among other nonessential drugs, were stopped, without apparent improvement.
After 1 week of persistent fever, stomach content of coffee‑ground appearance was found in the nasogastric tube. Gastroscopy showed an extensive ulcerous lesion in the greater curvature of the stomach, covered with fibro‑necrotic material; several samples of the lesion were taken during the procedure (Figure 1A). Thoracoabdominal computed tomography (CT) was performed, confirming gastric wall necrosis, without evidence of other lesions (Figure 1B). Histopathologic examination revealed an abundance of hyphae (Figure 1C), and preliminary microbiologic cultures isolated a fungus of the family Mucoraceae (Figure 1D and 1E).
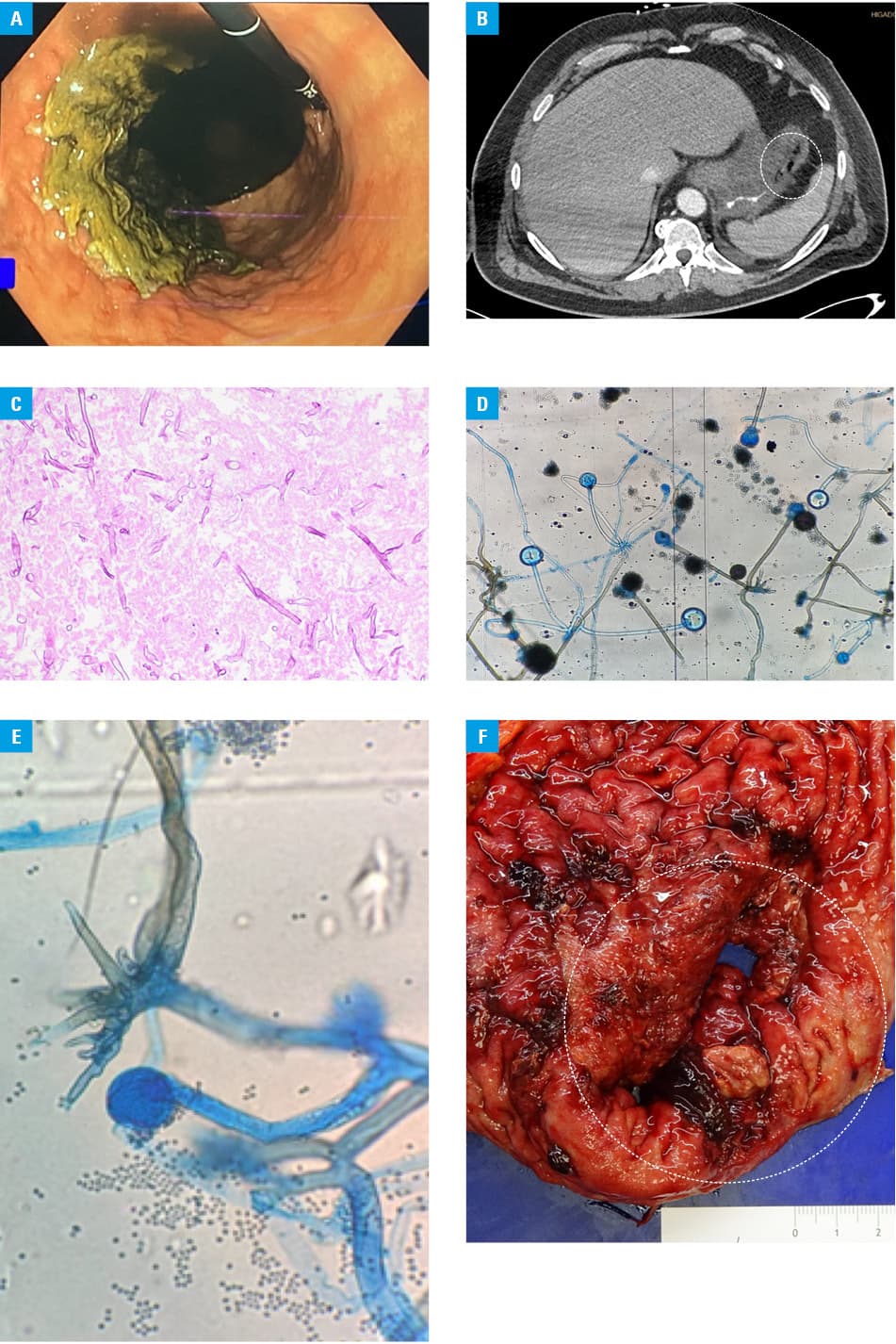
Antifungal therapy with isavuconazole and liposomal amphotericin B was initiated as soon as the suspicion of a fungal infection was raised, and a decision to attempt laparoscopic radical gastrectomy was made by a multidisciplinary team including also surgeons and microbiologists, assuming that the infection could still be localized. Rhizopus microsporus was identified in the isolate. During the procedure, a contained gastric perforation requiring extensive lavage of the necrotic material was revealed, leading to conversion to a long open surgery (Figure 1F). Finally, an esophago‑intestinal anastomosis was performed, the patient was extubated, and parenteral nutrition was maintained. A culture of the surgical samples confirmed the presence of R. microsporus. Histopathologic examination did not show angioinvasion of the surgical borders.
After the surgical intervention, the patient remained afebrile, and the levels of acute‑phase reactants decreased. Liposomal amphotericin B was maintained at a dose of 10 mg/kg/day and posaconazole was titrated to a target plasma concentration of 2–3 mg/l. Treatment with wide‑spectrum antibiotics was maintained for 2 weeks due to the evidence of a gastric perforation. A week after the surgery, CT was repeated, and no new lesions were found. Thus, a nasojejunal tube was introduced under gastroscopic guidance, and enteral nutrition was started with adequate tolerance. Also, positron emission tomography–CT was performed to monitor the effectiveness of treatment, without evidence of relapse. The patient was finally discharged after 2 months in the ICU, on well‑tolerated oral nutrition and having completed 6 weeks of double antifungal therapy, with no signs of persistent infection.
The diagnosis of gastrointestinal mucormycosis is complicated due to unspecific symptoms and the need to use invasive for microbiological sample collection. The majority of cases are diagnosed postmortem, although in the last years the number of premortem diagnoses has increased drastically, probably due to increasing awareness (eg, the emergence of COVID‑19–associated mucormycosis). Among the cases diagnosed in vivo, the most frequent scenario is sudden visceral perforation or gastrointestinal bleeding,4 leading to urgent surgery and a delayed etiologic diagnosis based on pathologic examination.
We present a unique case of in vivo diagnosis that was made based on the analysis of biopsy samples collected during endoscopy, before the subsequent gastric perforation. The sequence of events was crucial, as it enabled the multidisciplinary team to decide on the surgery, which was subsequently performed by experienced surgeons. In fact, the patient had received antifungal treatment for at least 5 days before the surgery. Considering this, it is difficult to conclude whether the antifungal treatment prevented dissemination of the fungus to the other organs while the surgery was being planned or whether it was responsible for the gastric perforation.
Another significant aspect of the present case is the condition predisposing to the invasive fungal infection: heatstroke. Intestinal ischemia plays a central role in the multiorgan failure occurring during heatstroke, with major gut wall damage and increased permeability. As a result, gram‑negative sepsis (translocation) is a major complication of heatstroke and empiric antibiotic therapy is the mainstay of treatment.5 Recent studies also point to uremia, previous malnutrition, complement depletion in the cases of disseminated coagulopathy, and altered immune response as other risk factors for infections in this clinical setting.5 Therefore, it seems reasonable to assume that these factors can also predispose to invasive fungal infections. Moreover, the use of broad‑spectrum antibiotics can, in fact, favor the eventual fungal proliferation, along with the metabolic abnormalities and internal derangement. In this context, blood tests of the patient were analyzed retrospectively, showing the concurrence of mild hyperglycemia and severe metabolic acidosis during the first 24 hours of shock. Hyperglycemia was attributed to the use of hydrocortisone at a dose of 50 mg every 6 hours (stress dosage) and intravenous glucose solutions. These features resemble the classic picture of diabetic ketoacidosis, in which proliferation of Mucorales can be expected.
- Skiada A, Pavleas I, Drogari‑Apiranthitou M. Epidemiology and diagnosis of mucormycosis: an update. J Fungi (Basel). 2020; 6: 265. | Crossref
- Cornely OA, Alastruey‑Izquierdo A, Arenz D, et al. Global guideline for the diagnosis and management of mucormycosis: an initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium. Lancet Infect Dis. 2019; 19: e405‑e421.
- Skiada A, Lass‑Floerl C, Klimko N, et al. Challenges in the diagnosis and treatment of mucormycosis. Med Mycol. 2018; 56 (Suppl 1): 93‑101. | Crossref
- Didehdar M, Chegini Z, Moradabadi A, et al. Gastrointestinal mucormycosis: a periodic systematic review of case reports from 2015 to 2021. Microb Pathog. 2022; 163: 105388. | Crossref
- Graber CD, Reinhold RB, Breman JG, et al. Fatal heat stroke. Circulating endotoxin and gram‑negative sepsis as complications. JAMA. 1971; 216: 1195‑1196. | Crossref
ARTICLE INFORMATION