Acute necrotizing pancreatitis in a patient with severe falciparum malaria and SARS-CoV-2 coinfection



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Acute necrotizing pancreatitis in a patient with severe falciparum malaria and SARS-CoV-2 coinfection
We present a case of a 35‑year‑old Polish seaman employed at a ship in Gabon, who experienced an unexpected 2‑day stay on land in Africa due to COVID‑19 pandemic–related flight cancellation on his way back to Poland. During the transfer he did not use antimalarial prophylaxis or mosquito bite precautions. In the second week following his return to Poland, he presented with fever, chills, and muscle aches. The nasal swab real‑time polymerase chain reaction (RT‑PCR) test confirmed SARS‑CoV‑2 infection, and the patient was recommended symptomatic treatment with home isolation. On the 6th day of persistent fever with chills, after telemedical reconsultation, antibiotic therapy was initiated with no improvement. After being informed of a diagnosis of malaria in the coworker whom he had travelled with, the patient was referred to a hospital for tropical diseases.
Upon admission, the patient was in a poor general condition, presented with fever, altered consciousness, hepatosplenomegaly, and jaundice. Lung auscultation showed no abnormalities. Laboratory workup demonstrated metabolic acidosis, neutrophilic leukocytosis at 36.66 × 109/l, (reference range [RR], 4–11 × 109/l), procalcitonin above 100 µg/l (RR, <0.5 µg/l), and C‑reactive protein level of 1781 nmol/l (RR, 47.5 nmol/l). In addition, renal failure (serum creatinine, 293.5 µmol/l; RR, 63.6–110.5 µmol/l; urea, 44.6 mmol/l; RR, 2.9–9.1 mmol/l), coagulopathy (D‑dimer, 22 070 ng/ml; RR, <500 ng/ml; international normalized ratio, 1.66; RR, 0.8–1.2; activated partial thromboplastin time, 41 s; RR, 22–34 s; fibrinogen, 1.15 g/l; RR, 2–4 g/l), thrombocytopenia (21 × 109/l; RR, 150–400 × 109/l), and anemia (hemoglobin, 71 g/l; RR, 130–180 g/l) were observed.
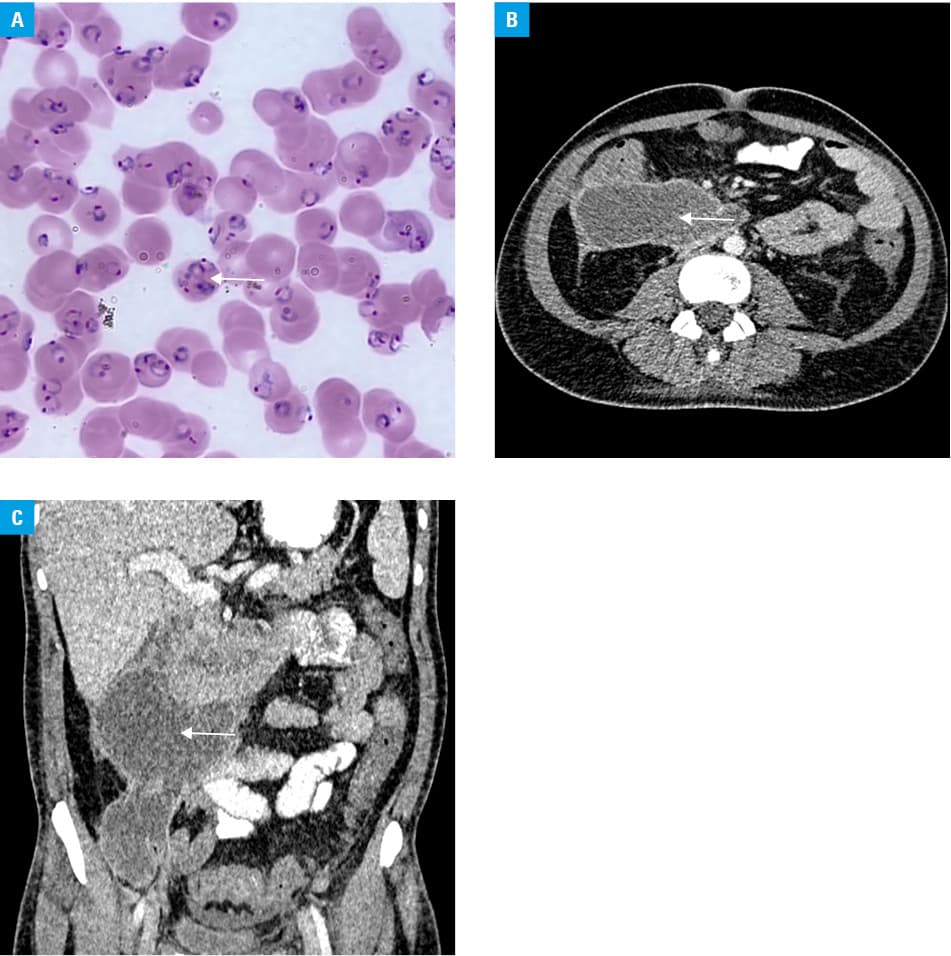
Rapid diagnostic test OptiMAL‑IT (DiaMed, Cressier, Switzerland) was positive for Plasmodium spp. Peripheral blood smear demonstrated Plasmodium falciparum ring stage with parasite density of 44% (Figure 1A). RT‑PCR assay confirmed monoinfection with P. falciparum. Severe falciparum malaria was diagnosed and treatment was initiated with intravenous artesunate. Due to consciousness impairment (Glasgow Coma Scale, 7) and progressive respiratory failure, the patient was admitted to the intensive care unit and required mechanical ventilation. Antimalarial treatment resulted in parasite clearance within a few days. Blood pressure was temporarily stabilized with noradrenaline. Broad‑spectrum antibiotics, parenteral nutrition, and industrial enteral feeding were initiated. The patient required renal replacement therapy (continuous veno‑venous hemodiafiltration) and blood transfusion. No typical COVID‑19 pneumonia lesions were found on chest computed tomography. Antiviral treatment was not used. On the 5th day of hospitalization, distended belly and lazy bowel movements were found together with elevated inflammatory markers and lipase activity exceeding 3 times the upper RR. Based on imaging studies, acute necrotizing pancreatitis with fluid collection was suspected. There was no history of any chronic alcohol consumption and no evidence of gallstones on abdominal imaging. The patient was referred for a surgery in order to perform percutaneous catheter drainage of the walled‑off pancreatic necrosis (Figure 1B and 1C). Subsequently, he required surgical drainage and appendectomy before he recovered.
Acute pancreatitis is a very rare complication of malaria with only 32 cases reported so far.1-3 Vascular changes caused by infected red blood cells cytoadherence to the endothelium, sequestration, and rosetting leading to ischemia are implicated in the pathogenesis of malarial pancreatitis.4 These result in activation of pancreatic enzymes. SARS‑CoV‑2 infection in the reported patient caused substantial delay in the diagnosis of malaria, which, together with a lack of antimalarial chemoprophylaxis, finally resulted in an extremely high parasite load and severe life‑threatening multiorgan dysfunction that included acute pancreatitis.
- Roy S, Parchani A, Sharma S, et al. Falciparum malaria‑induced acute pancreatitis. IDCases. 2020; 21: e00911. | Crossref
- Abhilash KP, Ahmed AS, Sathyendra S, Abraham OC. Acute pancreatitis due to malaria: a case report of five patients and review of literature. J Family Med Prim Care. 2016; 5: 691‑694. | Crossref
- Sehgal IS, Agarwal R, Behera D, Dhooria S. Malarial pancreatitis: case report and systematic review of the literature. Indian J Crit Care Med. 2015; 19: 743‑746. | Crossref
- Druml W, Laggner AN, Lenz K, et al. Pancreatitis in acute hemolysis. Ann Hematol. 1991; 63: 39‑41. | Crossref
ARTICLE INFORMATION