Unexpected malignancy: resection of a large thoracic solitary fibrous tumor of the pleura with preoperative arterial embolization



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Unexpected malignancy: resection of a large thoracic solitary fibrous tumor of the pleura with preoperative arterial embolization
Solitary fibrous tumors of the pleura (SFTP) are rare mesenchymal neoplasms with fibroblastic differentiation that account for less than 5% of pleural tumors.1 They are usually benign but occasionally a malignant component arises from the dedifferentiation of benign cells.2 We present a clinical picture of a giant SFTP with a malignant component and abundant vascular supply that was treated with preoperative arterial embolization followed by a surgical resection.
A previously healthy, 62‑year‑old woman was admitted to the hospital due to dyspnea, dry cough, and a low‑grade fever persisting for 3 months. She had no history of tobacco use, and her family medical history was unremarkable. During the examination, her oxygen saturation was 94% and decreased breath sounds were detected in the lower right chest. The rest of the physical examination was unremarkable. Laboratory test results, including a complete blood count, serum electrolytes, coagulation tests, and liver and kidney function tests, were within normal range.
A contrast‑enhanced computed tomography (CT) scan was performed, which revealed a 17.5 cm × 12 cm × 9 cm mass in the lower part of the right hemithorax that was in contact with both the lung and the diaphragm (Figure 1A and 1B). The mass was pressing the right basal lung and heart. The involvement of adjacent organs was unclear. Results of ultrasound‑guided core needle biopsy showed bundles of spindle‑shaped cells with moderate polymorphism and moderate mitotic activity, suggestive of SFTP.
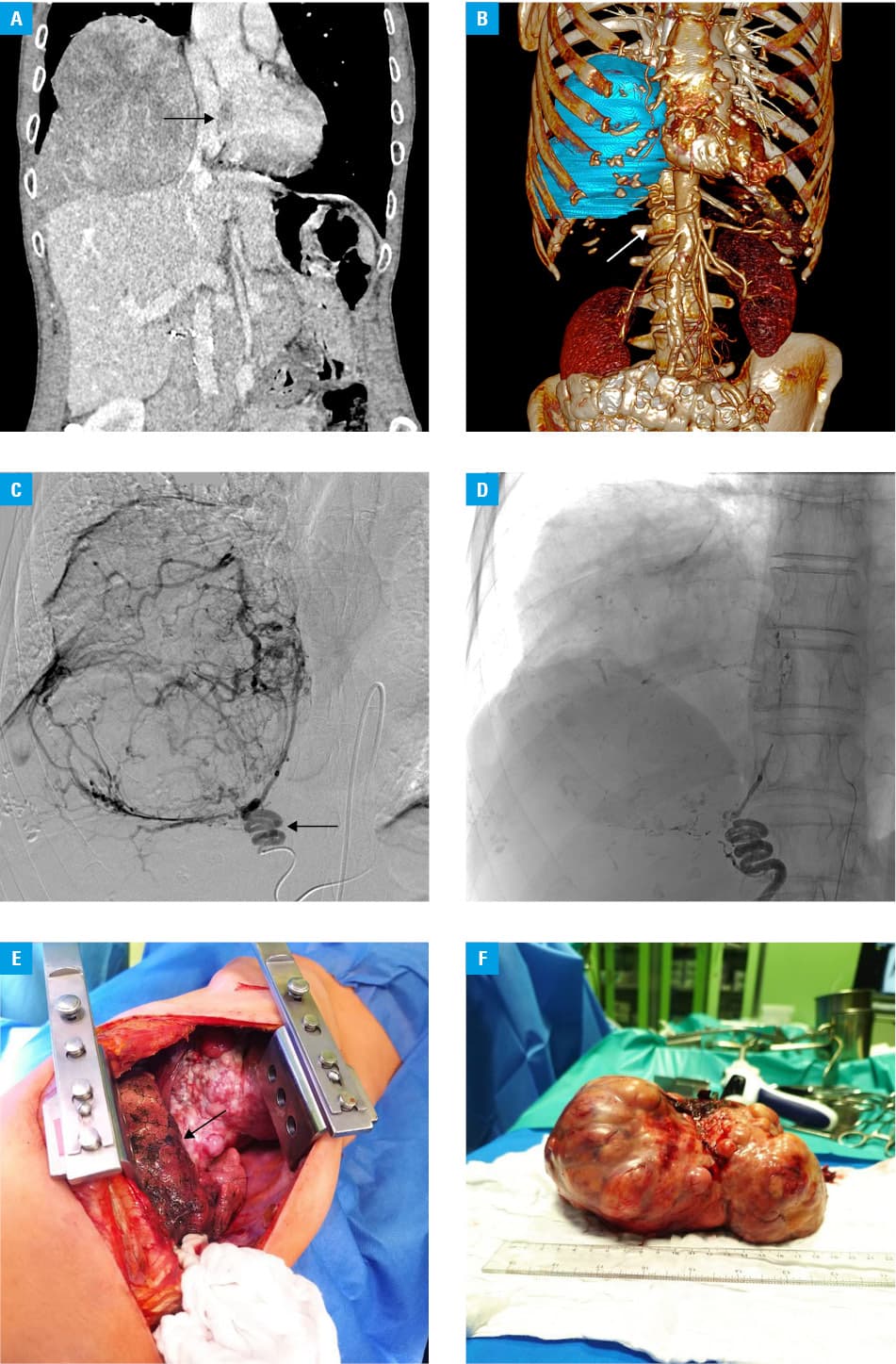
Because of the extensive vascularization of the tumor, the patient was referred for preoperative arterial embolization. Angiography showed the involvement of the right inferior phrenic artery that supplied the tumor with blood (Figure 1C). A mixture of cyanoacrylate glue and lipiodol (15%) was used to embolize this vessel. Postoperative angiography confirmed the reduction of blood flow to the tumor (Figure 1D).
A right posterolateral thoracotomy via the 6th intercostal space was performed on the following day to remove the tumor. Thoracotomy revealed an encapsulated massive tumor growing from the right diaphragmatic parietal pleura (Figure 1E). The right lung compressed and adhered to the mass. The tumor was completely resected en bloc, together with the pedicle connected to the diaphragm. Chest radiography performed on the postoperative day 4 revealed an expanded right lung and no evidence of pneumothorax. Subsequently, the patient was discharged from the hospital in a stable condition.
The tumor had a smooth, lobulated surface that was well‑demarcated macroscopically (Figure 1F). Histologically, it consisted of fibroblast‑like cells with limited mitotic activity. Immunohistochemical evaluation revealed positive staining for CD34, CD39, and STAT6, typical of SFTP. However, a dedifferentiated malignant component consistent with small cell sarcoma (G3) was also found.
As the surgical access to the inferior phrenic artery was considered difficult, preoperative arterial occlusion was performed. This facilitated the tumor resection and prevented intraoperative bleeding.3 The biopsy and macroscopic appearance suggested benign SFTP but histopathologic examination revealed malignancy. Our patient did not receive adjuvant treatment due to uncertain benefit.4 After 3 months of follow‑up, no pleural effusion or neoplasm was found on CT.
- Fiore F, Stoia V, Somma F. Surgical recurrence of solitary fibrous tumor of the pleura treated with microwave (MW) thermoablation: a case report. Thorac Cancer. 2020; 11: 443‑446. | Crossref
- Yokoi T, Tsuzuki T, Yatabe Y, et al. Solitary fibrous tumour: significance of p53 and CD34 immunoreactivity in its malignant transformation. Histopathology. 1998; 32: 423‑432. | Crossref
- Cox J, Leesley H, DeAnda A, et al. Resection of a giant thoracic solitary fibrous tumor treated with preoperative arterial coiling followed by a double‑level thoracotomy. J Surg Case Rep. 2023; 2023: rjad008. | Crossref
- Robinson LA. Solitary fibrous tumor of the pleura. Cancer Control. 2006; 13: 264‑269. | Crossref
ARTICLE INFORMATION