Bland embolization hits the target: endovascular method for treating liver neuroendocrine tumor metastases



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Bland embolization hits the target: endovascular method for treating liver neuroendocrine tumor metastases
We present a case of a 51‑year‑old man, former smoker, who underwent abdominal ultrasound due to fever and nausea. The examination revealed heterogeneous echogenicity of the liver with 4–5 lesions. A diagnosis of a well‑differentiated, intermediate grade, metastatic neuroendocrine tumor (NET) (Ki67 of 20%) was made based on core biopsy of one of the lesions. The examination was expanded to a positron emission tomography (PET) scan with 68gallium‑labeled somatostatin analogue that visualized peripherally increased expression of somatostatin receptors within the liver lesions and in the topography of the gastric fundus. Computed tomography (CT) scan confirmed metastases of the diameter ranging from 30 mm to 70 mm. Endoscopic ultrasound (EUS) and cytology of the tissue sample obtained from the gastric wall focal lesion confirmed a neuroendocrine neoplasm with Ki67 of 10%–15% (G2) with the primary source in the stomach.
According to current guidelines,1 treatment with a long‑acting somatostatin analogue, lanreotide, was started at 60 mg, and eventually the patient received a daily dose of 120 mg. Due to persistent diarrhea occurring directly after lanreotide administration, the analogue was replaced with ocreotide. After 3 months of treatment, an abdominal CT scan revealed progression of the disease. The patient was qualified for chemotherapy (capecitabine and temozolomide), but he refused the treatment.
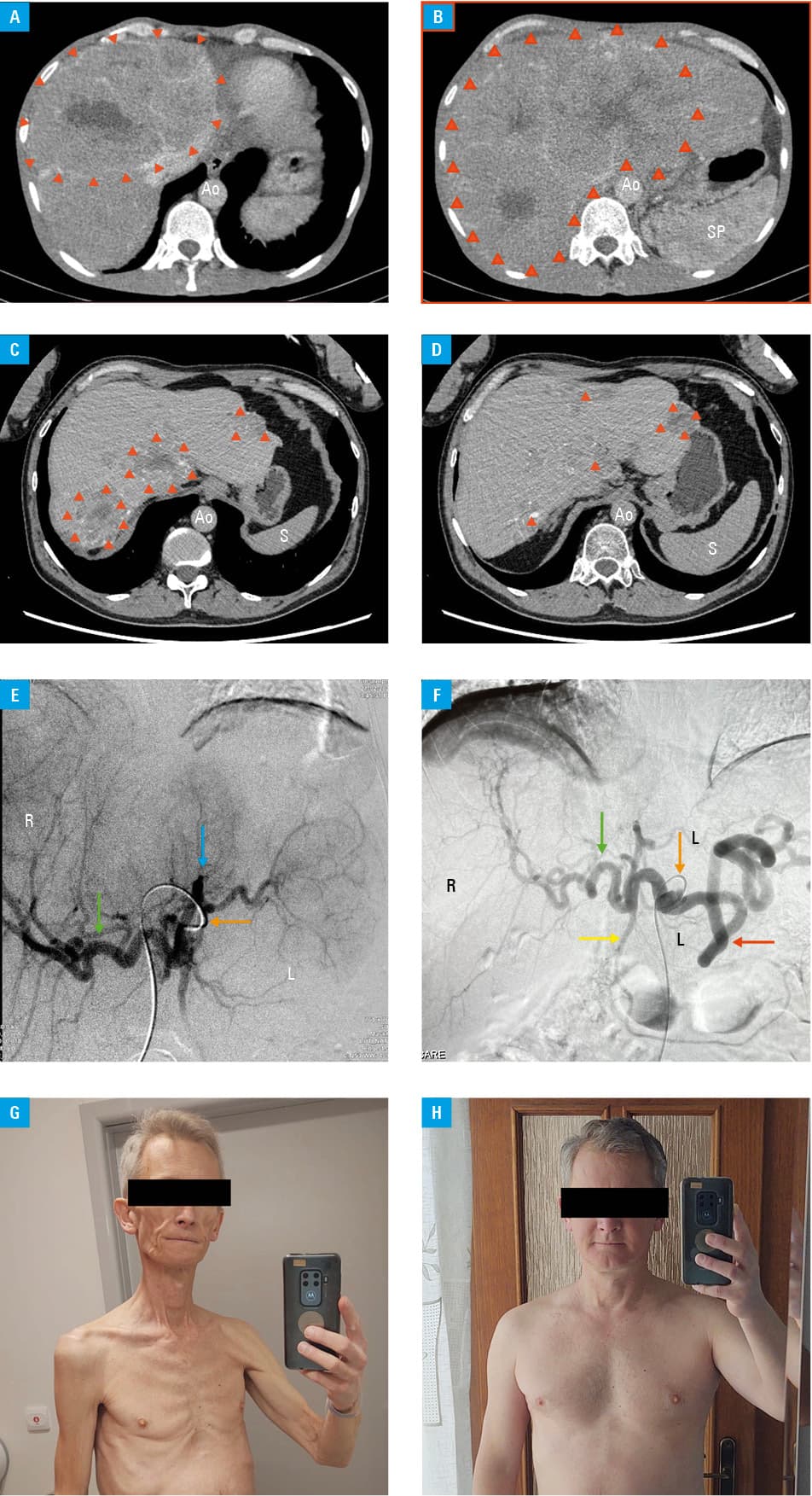
After consultation with physicians specializing in interventional radiology, the patient was qualified for embolization of the metastatic lesions in the liver. This approach is reported in the literature,2 but it is not a standard treatment used at Polish oncology centers. The abdominal CT scan performed immediately before embolization showed the enlarged liver, and an increase in the size of the liver lesions since the previous scan 7 months ago, with the largest lesion measuring 130 mm × 95 mm × 120 mm (Figure 1A and 1B). Due to the extent of the lesions, embolization procedures were performed in 3 stages at 4‑week intervals. The procedures were performed by puncturing the right femoral artery under local anesthesia, using Embozene microspheres of 500 to 700 µm in size. On the control CT and PET scans performed after the procedures, a significant reduction in the size of the metastatic lesions was disclosed (they were up to 78 mm × 79 mm × 80 mm, a reduction of approximately one‑third in volume). The lesions were more heterogeneous, with visible central disintegration and presence of atrophic calcifications (Figure 1C and 1D). Follow‑up angiography showed an effective reduction in the lesion vascularization (Figure 1E and 1F). The patient reported a significant improvement in his condition, apart from avoiding intense exercise that causes abdominal pressure, he has returned to his predisease state. He currently reports no abdominal pain and has presented a return of appetite with a significant increase in body weight (Figure 1G and 1H). He remains under surveillance due to hypothyroidism.
NETs are a rare, heterogeneous group of neoplasms with a considerable malignant potential. They usually become symptomatic and are diagnosed after the appearance of liver metastases (LMs). As many as 27% of patients diagnosed with NETs are expected to develop LMs.3 The presence of LMs strongly influences the prognosis,4 and can cause severe, debilitating symptoms that negatively affect the quality of life. By stabilizing the tumor growth, liver embolization provides adequate symptom relief for patients with NETs.
- Shah MH, Goldner WS, Benson AB, et al. Neuroendocrine and adrenal tumors, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2021; 19: 839‑868.
- Kulke MH, Shah MH, Benson AB 3rd, et al. Neuroendocrine tumors, version 1.2015. J Natl Compr Cancer Netw. 2015; 13: 78‑108. | Crossref
- Yao JC, Hassan M, Phan A, et al. One hundred years after “carcinoid”: epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J Clin Oncol. 2008; 26: 3063‑3072. | Crossref
- Pavel M, Baudin E, Couvelard A, et al. ENETS Consensus Guidelines for the management of patients with liver and other distant metastases from neuroendocrine neoplasms of foregut, midgut, hindgut, and unknown primary. Neuroendocrinology. 2012; 95: 157‑176. | Crossref
ARTICLE INFORMATION