Coronary sinus reducer implantation in a patient after previous CABG, PCI, TAVI, MitraClip, and CRT-D



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Coronary sinus reducer implantation in a patient after previous CABG, PCI, TAVI, MitraClip, and CRT-D
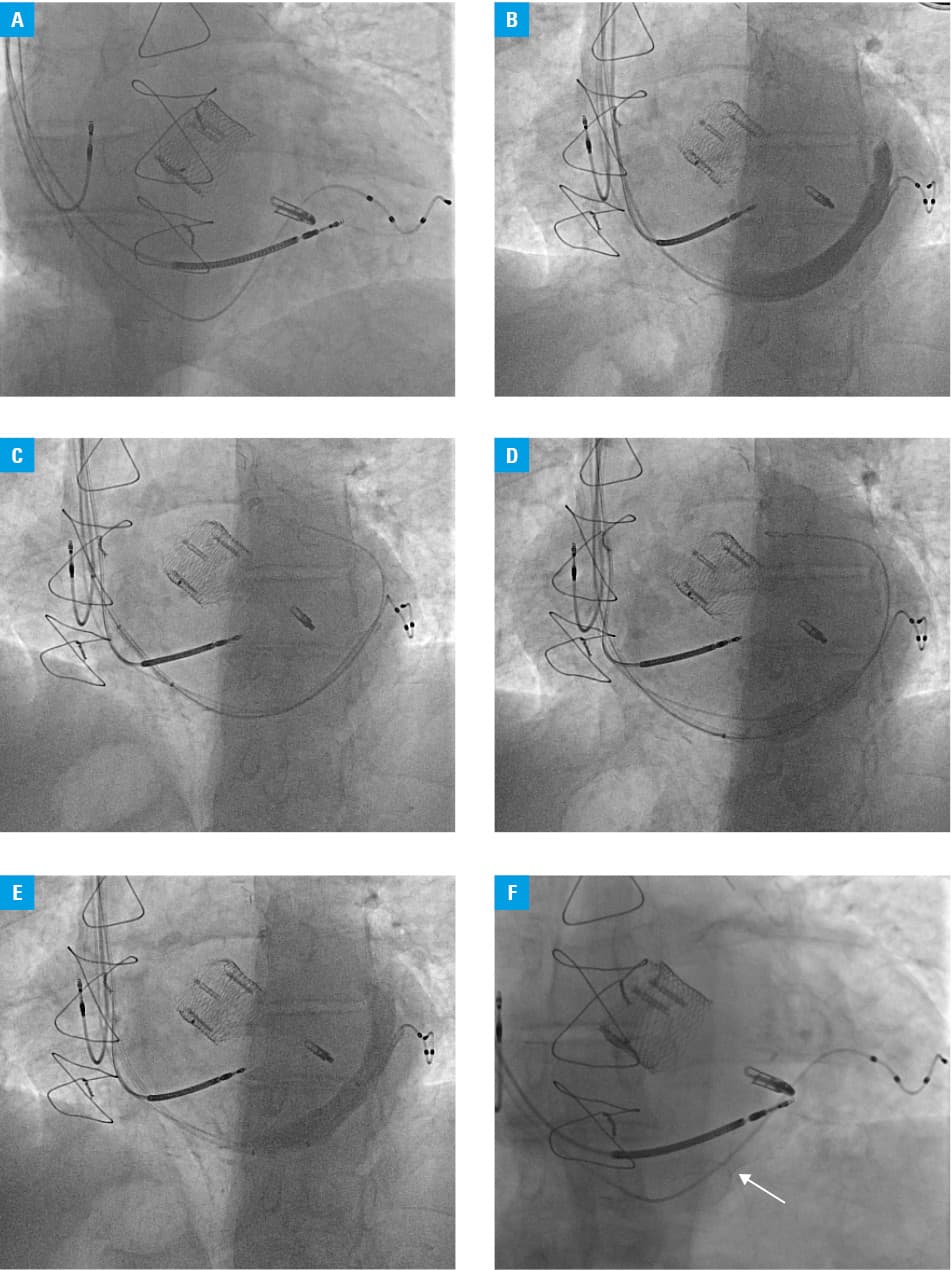
An 81‑year‑old man with multiple comorbidities including advanced coronary artery disease (CAD) with a history of myocardial infarction, hypertension, hyperlipidemia, paroxysmal atrial fibrillation, left bundle branch block, history of aortic stenosis treated with transcatheter aortic valve implantation, and severe mitral regurgitation treated with MitraClip implantation, with prior cardioverter‑defibrillator implantation and subsequent device upgrade to cardiac resynchronization therapy (CRT‑D), presented with advanced stable angina (Canadian Cardiovascular Society [CCS] grade 3). The patient had a complex history of coronary revascularization, including coronary artery bypass grafting and multiple percutaneous coronary interventions with drug‑eluting stent implantation in both the graft and native arteries with no revascularization target. This was confirmed by recent coronary angiography, which showed patency of all grafts and no significant lesion in the last remaining nongrafted circumflex artery (Supplementary material, Figure S1). Considering the intensity of symptoms despite optimal medical therapy (5 antianginal medications at maximum tolerated doses) resulting in a poor quality of life, the patient was qualified for implantation of the coronary sinus reducer after objectifying indications on stress echocardiography (confirmation of inducible wall motion abnormalities in the anterior segments of the left ventricle along with exclusion of significant dysfunction of the previously treated heart valve). The procedure was performed under local anesthesia. Vascular access was achieved through a 9F sheath inserted via the internal jugular vein with echocardiographic guidance. After an initial evaluation of the right atrium (Figure 1A), the mean pressure was recorded below 15 mm Hg, and the ostium of the coronary sinus was intubated with an MP 2A guide catheter supported by a standard 0.035‑inch J‑tip guidewire. Using an angiogram supported by quantitative coronary angiography, the target implantation place was properly sized (Figure 1B). Afterward, the guide catheter was changed to a 9F VISTA BRITE TIP guiding catheter with the support of the 0.035‑inch J‑tip guidewire, which enabled the delivery of the Neovasc Reducer system (Neovasc, Minneapolis, Minnesota, United States) into the designated part of the coronary sinus (Figure 1C) and successful deployment with 6 atm pressure inflation of the delivery system (Figure 1D) (determined by previous angiographic measurements). After balloon catheter insertion, deflation, and retraction, follow‑up angiography was performed to exclude possible complications (Figure 1E and 1F). In the postprocedural evaluation (3‑month follow‑up) significant reduction of angina symptoms (to CCS class 2) was observed. This report was objectified by the increase in the 6‑minute walking distance test, which raised from the baseline of 150 meters to 240 meters. Additionally, the patient claimed to have noticed improvement in his quality of life, angina frequency, and physical limitations, as assessed by the Seattle Angina‑7‑Questionnaire.
Despite the availability of a broad armamentarium of pharmacological and procedural therapies, chronic resistant angina affects up to 10% of patients with CAD.1,2 There is an urgent need to develop new treatment options to improve the quality of life and prognosis in this challenging patient population. Implantation of a coronary sinus reducer appears to be a safe and effective treatment option for the vast majority of these patients,3-5 even those, as in the presented case, with extremely advanced multifactorial cardiac dysfunction, who have undergone multiple sophisticated cardiac and cardiosurgical interventions. Although there are no clear guidelines regarding the implantation of a coronary sinus reducer in patients with the presence of a CRT‑D lead in the coronary sinus, the presented case suggests good feasibility and safety of such a procedure with unimpaired CRT‑D function. Noteworthy, previous complete revascularization of all hemodynamically significant lesions and adjunctive optimal medical therapy were insufficient to control chronic angina. However, in this challenging clinical subset, the coronary sinus reducer provided adequate angina control.
- Povsic TJ, Henry TD, Ohman EM, et al. Therapeutic approaches for the no‑option refractory angina patient. Circ Cardiovasc Interv. 2021; 14: e009002. | Crossref
- Trzeciak P, Desperak P, Duda‑Pyszny D, et al. Long‑term outcomes of 11 021 patients with chronic coronary syndromes and after coronary angiography: the PRESAGE registry. Pol Arch Intern Med. 2020; 130: 1043‑1052. | Crossref
- Verheye S, Jolicœur EM, Behan MW, et al. Efficacy of a device to narrow the coronary sinus in refractory angina. N Engl J Med. 2015; 372: 519‑527. | Crossref
- Włodarczak S, Rola P, Jastrzębski A, et al. Coronary sinus reducer implantation in refractory angina. Short‑term outcome of Lower Silesia Sinus Reducer Registry (LSSRR). Kardiol Pol. 2023; 81: 508‑511. | Crossref
- Wojciech Z, Kuliczkowski W, Reczuch K. Coronary sinus reducer implantation in patients with refractory angina: first experience in Poland. Kardiol Pol. 2021; 79: 471‑472. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION