Pulmonary embolism after delivery as the first manifestation of Cushing disease in pregnancy



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Pulmonary embolism after delivery as the first manifestation of Cushing disease in pregnancy
Endogenous Cushing syndrome (CS) is an extremely rare condition in pregnancy, with adrenal etiology being the most common.1 Diagnosis and management of CS among pregnant women are challenging.1,2 Difficulties are not only caused by physiologic overactivity of the hypothalamic–pituitary–adrenal axis during pregnancy, but also by the overlapping clinical features of a healthy pregnancy and CS.
We present a case of a 37‑year‑old woman with hypertension, obesity, and gestational diabetes, who was diagnosed with CS in the course of pulmonary embolism (PE) after delivery. The weight gain during pregnancy was 40 kg. The pregnancy was terminated in the 28th week by cesarean section due to pre‑eclampsia. The child developed bronchopulmonary dysplasia, grade 2 intraventricular bleeding, and retinopathy, and was later diagnosed with mild mental retardation. On the second day of the postpartum period, the patient presented with dyspnea. Computed tomography pulmonary angiography revealed segmental PE (Figure 1A). Anticoagulant treatment with low‑molecular‑weight heparin was initiated in the intensive care unit and continued with acenocoumarol, with no bleeding complications. Inherited and acquired thrombophilia were excluded, and the patient was referred to an endocrinologist.
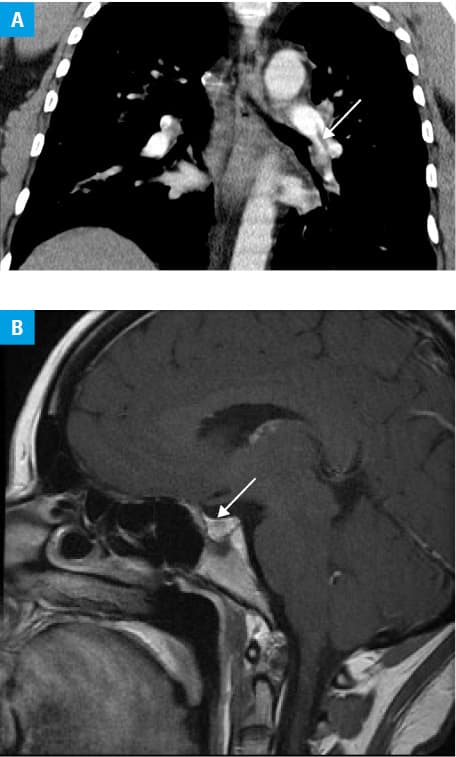
On admission to the Department of Endocrinology, the patient presented with obesity (body mass index of 46 kg/m2) and hypertension (grade 3 according to the European Society of Hypertension) persisting after the postpartum period despite 3‑drug therapy. The patient’s complaints had begun about 4 years earlier, and included elevated blood pressure and a weight gain of 20 kg. The endocrine evaluation indicated adrenocorticotropic hormone–dependent CS (Supplementary material, Table S1). Magnetic resonance imaging of the pituitary gland revealed a microadenoma (3 mm × 2 mm) (Figure 1B). She underwent a successful trans‑sphenoidal surgery, followed by an initiation of hydrocortisone supplementation. Gradual normalization of blood pressure allowed for discontinuance of antihypertensive drugs within 1 year. The hypothalamic–pituitary–adrenal axis returned to its normal function 16 months after the neurosurgery. Anticoagulation was discontinued after 9 years, following D‑dimer level testing (244.6 ng/ml; upper limit of normal, 500 ng/ml). During the 10‑year follow‑up, no signs of CS recurrence were observed (Supplementary material, Table S1).
It is extremely rare to conceive in an active phase of CS,1,2 with only slightly over 200 cases of such pregnancies described in the literature.3 Our case shows that PE may be the first life‑threatening presentation of CS that leads to the diagnosis. Previously, we reported a case of venous thromboembolism (VTE) in a patient with CS who had been taking a combined oral contraceptive containing estrogen.4 Since the risk of VTE is increased 10‑fold in the postpartum period and 18‑fold in CS,5 thromboprophylaxis is advised in pregnant women with CS.2 It is unclear whether the risks are additive or multiplicative, especially if they coexist with other risk factors for VTE (age, obesity, pre‑eclampsia, pre‑term birth, cesarean section). In the presence of a minor transient factor (puerperium), the anticoagulation could be stopped after 3 to 6 months; however, the guidelines on the duration of secondary prevention of recurrent VTE in patients with CS are currently missing. Considering the high risk of thrombosis, further studies are needed to investigate hypercoagulability in pregnant women with CS to set the standards of diagnosis and treatment.
- Kyriakos G, Farmaki P, Voutyritsa E, et al. Cushing’s syndrome in pregnancy: a review of reported cases. Endokrynol Pol. 2021; 72: 64‑72. | Crossref
- Luger A, Broersen LHA, Biermasz NR, et al. ESE Clinical Practice Guideline on functioning and nonfunctioning pituitary adenomas in pregnancy. Eur J Endocrinol. 2021; 185: G1‑G33. | Crossref
- Brue T, Amodru V, Castinetti F. Management of endocrine disease: management of Cushing’s syndrome during pregnancy: solved and unsolved questions. Eur J Endocrinol. 2018; 178: R259‑R266. | Crossref
- Minasyan M, Bryk‑Wiązania A, Hubalewska‑Dydejczyk A, Gilis‑Januszewska A. Pulmonary embolism as the first manifestation of Cushing syndrome in a young woman. Endokrynol Pol. 2022; 73: 990‑991. | Crossref
- Wagner J, Langlois F, Lim DST, et al. Hypercoagulability and risk of venous thromboembolic events in endogenous Cushing’s syndrome: a systematic meta‑analysis. Front Endocrinol (Lausanne). 2019; 9: 805. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION