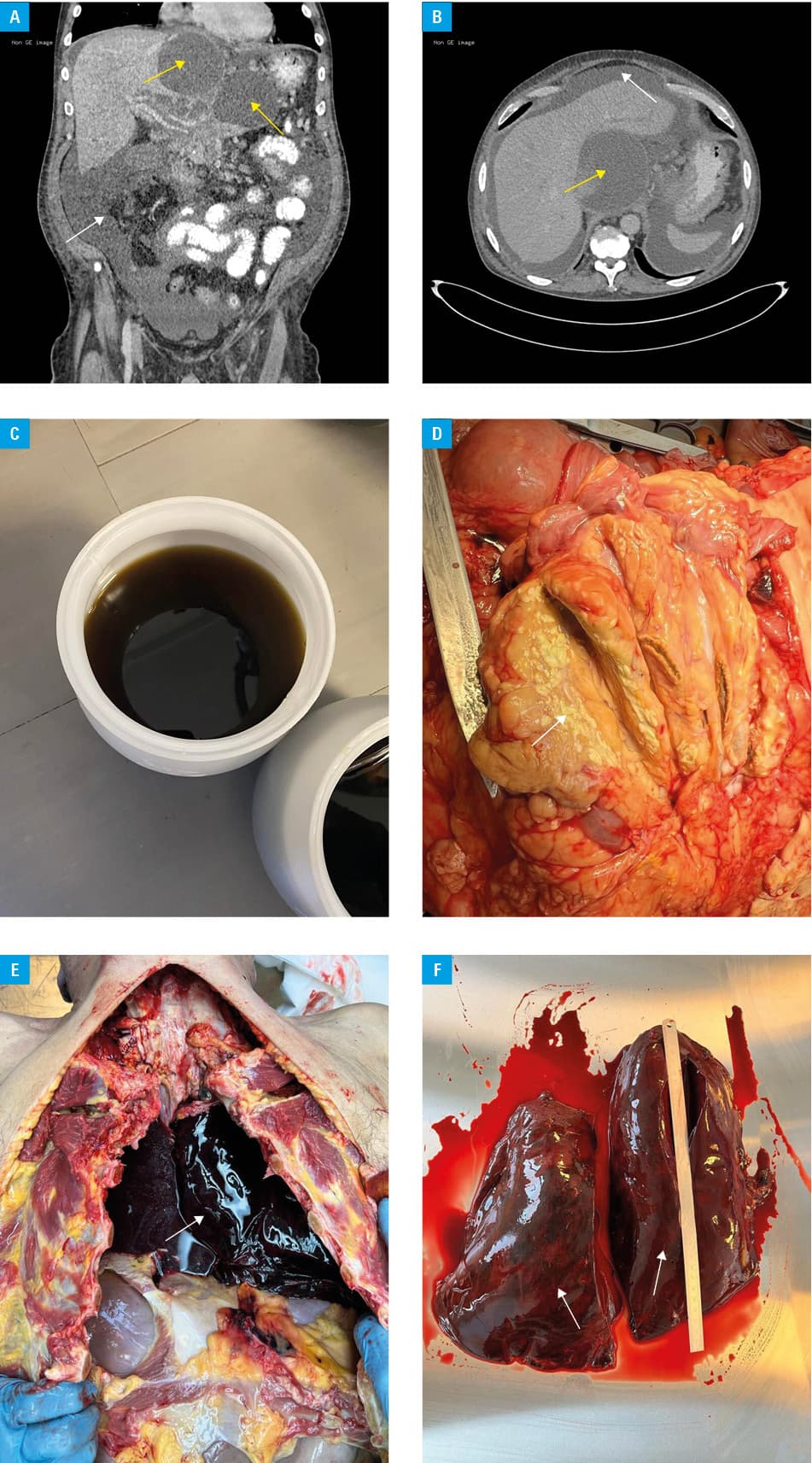
A 51‑year‑old man with type 2 diabetes presented with a 3‑day history of moderate abdominal pain and a notable enlargement of abdominal circumference. He reported a significant weight loss without any other alarming symptoms. His medical history was positive for alcohol abuse and negative for pancreatitis or abdominal trauma. Physical examination revealed sarcopenia, massive ascites, peripheral edema, and minor tenderness in the epigastric region. Laboratory workup revealed anemia (hemoglobin level, 10.9 g/dl; reference range [RR], 13.5–16.5 g/dl), leukocytosis (10.41 × 103/µl; RR, 4–10 × 103/µl), elevated serum level of C‑reactive protein (79 mg/l; RR <5 mg/l), as well as a significantly elevated activity of serum lipase (1216 U/I; RR, 13–60 U/l) and amylase (1233 U/l; RR, 28–100 U/l). Cancer antigen 19–9 and carcinoembryonic antigen levels were normal. Contrast‑enhanced computed tomography (CT) of the thorax, abdomen, and pelvis showed segmental pulmonary embolism, portal vein thrombosis with massive collateral veins, gross ascites, a large multicystic mass with hyperenhancing walls and multiple septations in the pancreatic head (50 mm × 70 mm)—a possible neoplasm, as well as large, thin‑walled fluid collections in the peripancreatic region (80 mm × 95 mm × 80 mm and 100 mm × 125 mm × 95 mm), recognized as pseudocysts in the course of pancreatitis (Figure 1A and 1B). There was no lymphadenopathy or metastases to the solid viscera. The results of ascitic fluid (Figure 1C) analysis were consistent with exudative effusion, with elevated amylase activity and leukocyte count greater than 500 cells/μl (RR <250 cells/μl). Blood and ascitic fluid cultures were negative. The presence of pancreatic ascites complicated by spontaneous bacterial peritonitis, as well as unfavorable features of the cystic lesions, were considered contraindications to invasive treatment by consulting surgeons and an endoscopist. The patient was therefore managed conservatively with the intention to reconsider subsequent treatment options. A second CT, carried out because of exacerbation of the epigastric pain, showed no significant differences, as compared with the previous scan. The patient’s clinical condition was stable with no further pain episodes. On day 10 of hospitalization, the patient collapsed after defecation; his vital signs were indicative of hypotension and tachycardia, followed by cardiac arrest with ineffective cardiopulmonary resuscitation. Autopsy revealed the pancreatic pseudocyst rupture with massive subphrenic hematoma extending to the mediastinum and the left thoracic cavity (Figure 1D–1F). Histopathologic examination of the cystic lesions was negative for malignancy, with the presence of focal necrosis and inflammatory tissue.
Pancreatic pseudocyst is defined as a localized collection of amylase‑rich fluid surrounded by a nonepithelialized wall made up of fibrous and granulation tissue, forming as a result of pancreatitis or pancreatic trauma. Its natural history ranges from spontaneous resolution, which is relatively common, to serious complications. In the cases of large cysts, local complications, or acute symptoms, invasive treatment should be applied.1 Forms of therapy include percutaneous catheter drainage, transendoscopic approach, or surgery. The choice of treatment depends on a number of factors, including the general condition of the patient, clinical features of the lesion(s) (size, number, and location), presence of infection, and suspicion of malignancy.2-4 We present the case of a fatal course of pseudocyst rupture to underline the importance of identification of possible complications and implementation of suitable management to minimize the associated morbidity and mortality.
- Mujer MT, Rai MP, Atti V, et al. Spontaneous rupture of a pancreatic pseudocyst. Case Reports. 2018; 2018: bcr‑2018‑226296. | Crossref
- Agalianos C, Passas I, Sideris I, et al. Review of management options for pancreatic pseudocysts. Transl Gastroenterol Hepatol. 2018; 3: 1‑8. | Crossref
- Rocha R, Marinho R, Gomes A, et al. Spontaneous rupture of pancreatic pseudocyst: report of two cases. Case Rep Surg. 2016; 2016: 1‑3. | Crossref
- Misra D, Sood T. Pancreatic pseudocyst. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023-. https://www.ncbi.nlm.nih.gov/books/NBK557594/. February 2023.
ARTICLE INFORMATION