A 42‑year‑old woman without chronic diseases or a history of surgical procedures reported for a diagnosis of nonspecific abdominal and pelvic pain lasting for several weeks (score 6–7 on the visual analog scale). The pain was not related to the phase of the menstrual cycle, and the patient denied any diarrhea or constipation. Laboratory workup and gynecological examination showed no abnormalities. A computed tomography (CT) scan of the pelvis showed a contrast‑enhanced, homogenous, nodular lesion of the colorectal wall at the level of the rectosigmoid junction, approximately 20 mm × 13 mm in size (Figure 1A and 1B). Magnetic resonance imaging (MRI) scans confirmed the presence of a soft‑tissue tumor within the muscular layer of the anterolateral sigmoid wall, widely protruding toward the intestinal lumen, without features of penetrating the intestinal wall (Figure 1C and 1D) or contrast enhancement, and with restricted diffusion (Figure 1E). Due to the suspicion of malignancy, the patient was referred for urgent endoscopy, which showed protrusion of the intestinal wall covered with a slightly uneven mucosa within the rectosigmoid junction, with no visible tumor. Specimens were taken for histopathologic examination, which indicated no abnormalities. 18F‑fluorodeoxyglucose positron emission tomography–CT showed an increased accumulation of the radiotracer within thickened right wall of the sigmoid (Figure 1F).
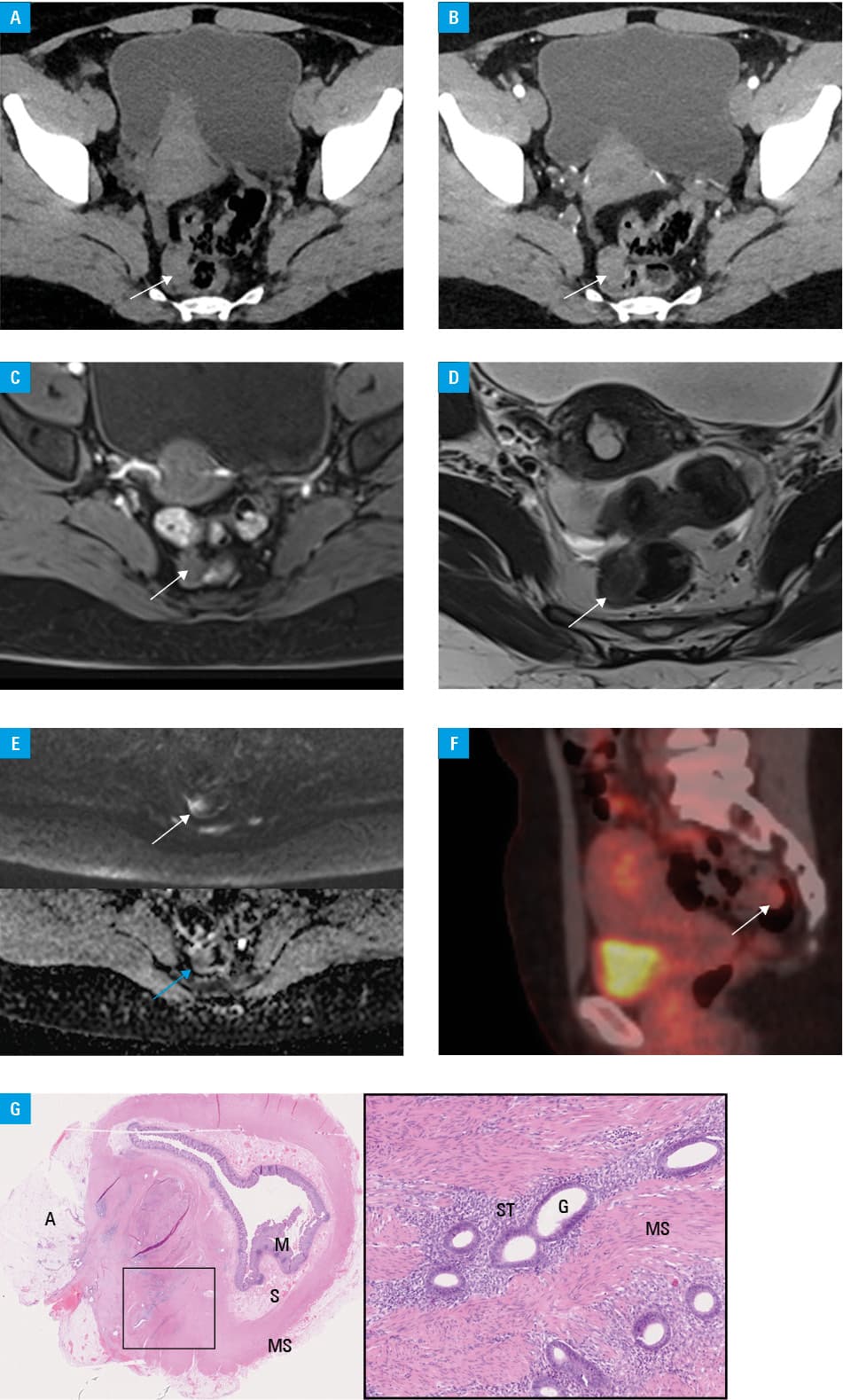
Finally, due to the suspicion of malignancy and taking the patient’s preferences into consideration, an anterior‑middle rectum resection was chosen as the method of treatment. The course of the surgery and the postoperative period were uneventful. After a few days of hospitalization, the patient was discharged in a good general condition with a properly healing wound. Histopathologic examination of the resected colorectal segment showed endometriosis in the muscle and adipose tissue with reactive hypertrophy of the muscle fibers (Figure 1G).
Endometriosis is a chronic disease that affects up to 10% of women of reproductive age. It is defined as the presence of ectopic endometrial glands and stroma outside the uterine cavity.1 The most common symptoms of endometriosis are pelvic pain and infertility.2 Deep infiltrating endometriosis (DIE) refers to involvement of the muscular layer of the intestinal wall or penetration more than 5 mm in depth under the peritoneal surface.3,4 More than one‑third of DIE cases are located within the colorectum. Transvaginal / transrectal ultrasonography (US) and MRI are the most important imaging tools to visualize DIE in this location. US is frequently the first examination performed, but the detection rate largely depends on the experience of the examiner. On MRI, the typical image of DIE is a T2‑hypointense hemispherical nodule that shows an increased signal on T1‑weighted images, which is characteristic of methemoglobin.3 However, in more advanced phases of hemoglobin degradation the signal may be lower. For both US and MRI, the sensitivity and specificity of the diagnosis of rectosigmoid endometriosis are above 90%.5 Nevertheless, endometriosis may still be misdiagnosed as a neoplastic process before surgery.3,4 In our patient, abdominal pain was not related to the phase of the menstrual cycle, and the intensity of the signal on T1‑weighted images was low; therefore, endometriosis was not primarily considered in the differential diagnosis. The use of a combination of imaging methods (mainly MRI and US) and a cooperation between radiologists and surgeons seem to be crucial in establishing the correct diagnosis and choosing the optimal method of DIE treatment.
- Vercellini P, Viganò P, Somigliana E, Fedele L. Endometriosis: pathogenesis and treatment. Nat Rev Endocrinol. 2014; 10: 261‑275. | Crossref
- Burney RO, Giudice LC. Pathogenesis and pathophysiology of endometriosis. Fertil Steril. 2012; 98: 511‑519. | Crossref
- Jaramillo‑Cardoso A, Shenoy‑Bhangle AS, VanBuren WM, et al. Imaging of gastrointestinal endometriosis: what the radiologist should know. Abdom Radiol (NY). 2020; 45: 1694‑1710. | Crossref
- Abrão MS, Petraglia F, Falcone T, et al. Deep endometriosis infiltrating the recto‑sigmoid: critical factors to consider before management. Hum Reprod Update. 2015; 21: 329‑339. | Crossref
- Moura APC, Ribeiro HSAA, Bernardo WM, et al. Accuracy of transvaginal sonography versus magnetic resonance imaging in the diagnosis of rectosigmoid endometriosis: systematic review and meta‑analysis. PLoS One. 2019; 14: e0214842. | Crossref
ARTICLE INFORMATION