Breast implant–associated anaplastic large cell lymphoma as a late complication of breast implant placement: a report of 3 Polish cases



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Breast implant–associated anaplastic large cell lymphoma as a late complication of breast implant placement: a report of 3 Polish cases
We present 3 cases of women who developed breast implant–associated anaplastic large cell lymphoma (BIA‑ALCL) following breast augmentation (2 patients) or implant reconstruction surgery (1 patient). The time between the implant surgery and the occurrence of symptoms was 5 to 7 years (range, 58–84 months; median, 84 months; mean, 75.33 months). All patients complained of breast edema. No other symptoms were present and no infection signs were observed. Ultrasound examination revealed seroma in all 3 patients, and reactive axillary lymph nodes and a single lymph node with decreased echogenicity in 1 patient. Postoperative positron emission tomography–computed tomography (PET‑CT) scans of Patient 2 showed metabolically active foci in both breasts suggesting reactive changes or lymphoma infiltrations. The scans showed changes exclusively in the breasts, with no other organs involved (Figure 1A–1D).
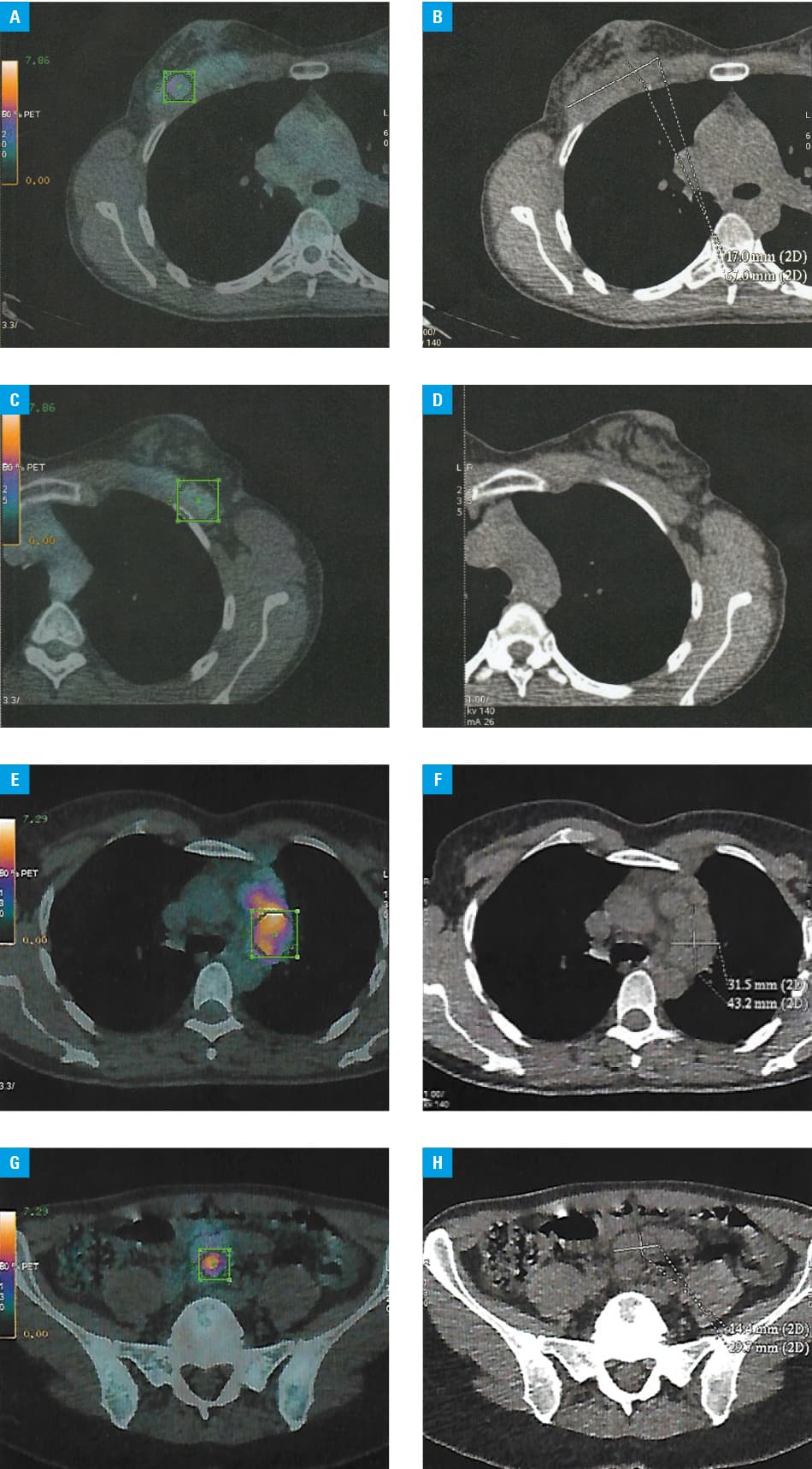
Both implants were removed in all patients. Histopathologic assessment of the resected material, along with CD30 positivity and ALK1 negativity found in immunohistochemical staining, confirmed the diagnosis of BIA‑ALCL. In the 2‑year follow‑up, 2 women remained in complete response after implant removal and 1 (Patient 1) developed a relapse of BIA‑ALCL in the lymph nodes on both sides of the diaphragm (Figure 1E–1H; Supplementary material, Figure S1I and S1J). She received 6 cycles of chemotherapy with the CHOEP regimen and achieved complete metabolic response. All the women are under the care of the hematology clinic and remain in good general condition. Their detailed characteristics are presented in Supplementary material, Table S1.
Breast implants, alongside other methods, are used for breast reconstruction following mastectomy and for breast augmentation. Breast implant insertion is a common and developing procedure, with high demand worldwide.1 BIA‑ALCL is an uncommon complication of breast implant surgery using textured devices, with an estimated overall prevalence of 1:13 745 in 28 European countries.2
BIA‑ALCL is a rare primary non‑Hodgkin T‑cell lymphoma that can be distinguished from anaplastic lymphoma kinase (ALK)-negative ALCLs by CD30 positivity.3 However, ALCLs might be ALK‑positive as well.4 Theories on the etiopathogenesis include a complex immune stimulation on the surface of a textured implant, as well as chronic inflammation leading to lymphoproliferation and lymphomagenesis. The innate and adaptive immunity factors, such as interleukin (IL)-4 and IL‑13 secretion, affect the activity of macrophages. Furthermore, IL‑1 secretion and production of other ILs lead to the formation of a specific microenvironment. The Janus kinase / signal transducers and activators of transcription signaling pathway may be involved in cell proliferation and ALCL. BIA‑ALCL is characterized by triple‑negativity for ALK, dual specificity phosphatase‑22, and tumor protein p63.2,5
Persistent seroma (a localized accumulation of clear fluid that may cause swelling and discomfort) is the most common clinical presentation.4 The symptoms usually occur over 1‑year postoperation, with an average of 7 to 10 years. Other symptoms include erythema or skin ulceration, swelling, or asymmetry.1 The diagnosis must be confirmed by ultrasound imaging, followed by fine‑needle fluid aspiration, which enables cytology, immunohistochemistry, and flow cytometry or core biopsy.2,3
Ultrasound is the primary tool used in breast imaging and the BIA‑ALCL diagnostic process. PET‑CT is recommended to assess the stage of the disease and surgical planning. Surgical treatment with en bloc excision including healthy tissue margins is recommended in localized disease. Prophylactic contralateral implant removal should also be considered.2,3 In advanced stages, lymphadenectomy is required.5 Recommendations regarding adjuvant treatment in patients with positive residual disease have not been established yet; however, a positive impact of systemic ALCL treatment regimens or brentuximab vedotin has been observed.2,3,5
The risk of BIA‑ALCL relapse is the lowest following complete surgical excision, provided the disease is limited to the capsule, which directly reflects on good / excellent prognosis, with up to 93% of cases achieving complete remission at the 2‑year follow‑up due to indolent clinical features of the disease.1,5
In conclusion, the problem of BIA‑ALCL is underestimated. It is necessary to increase awareness both among patients and primary care physicians, gynecologists, and radiologists of the possibility of BIA‑ALCL development. Further research with respect to methods of early detection, prevention, and treatment is highly warranted.
- Turton P, El‐Sharkawi D, Lyburn I, et al. UK Guidelines on the diagnosis and treatment of breast implant‐associated anaplastic large cell lymphoma on behalf of the Medicines and Healthcare products Regulatory Agency Plastic, Reconstructive and Aesthetic Surgery Expert Advisory Group. Br J Haematol. 2021; 192: 444‑458. | Crossref
- Santanelli di Pompeo F, Clemens MW, Atlan M, et al. 2022 Practice recommendation updates from the World Consensus Conference on BIA‑ALCL. Aesthet Surg J. 2022; 42: 1262‑1278. | Crossref
- Clemens MW, Jacobsen ED, Horwitz SM. 2019 NCCN consensus guidelines on the diagnosis and treatment of breast implant‑associated anaplastic large cell lymphoma (BIA‑ALCL). Aesthet Surg J. 2019; 39: S3‑S13. | Crossref
- Mrowiec S, Jabłońska B, Rozłucka L, et al. Atypical course of anaplastic large cell lymphoma with positive anaplastic lymphoma kinase. Pol Arch Intern Med. 2021; 131: 381‑383. | Crossref
- Zhang X‑R, Chien P‑N, Nam S‑Y, Heo C‑Y. Anaplastic large cell lymphoma: molecular pathogenesis and treatment. Cancers. 2022; 14: 1650. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION