Unsuspected large cyanoacrylic mass in the right atrium in a patient scheduled for liver transplantation



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Unsuspected large cyanoacrylic mass in the right atrium in a patient scheduled for liver transplantation
A 61‑year‑old man with alcoholic liver cirrhosis was admitted for coronary angiography (CA) as part of an organ transplant qualification procedure. While awaiting CA, the patient experienced gastric variceal bleeding, successfully obliterated endoscopically with cyanoacrylate. CA was performed 2 months later and showed no significant lesions. However, during the procedure, an unusual opacity moving within the right heart chambers was noticed (Figure 1A and 1B). Transthoracic echocardiography (TTE) revealed an additional hyperechogenic, mobile mass in the right atrium (RA), 50 mm × 10 mm in size, related to the Eustachian valve (Figure 1C and 1D). No signs of pulmonary hypertension were detected. Subsequent computed tomography pulmonary angiography showed a linear hyperdense structure in the RA and several hyperdense lesions in the pulmonary arteries. Material with a similar density was present in the obliterated varices which connected via collaterals to the left renal veins (Figure 1E and 1F). Eventually, cyanoacrylic pulmonary embolism with the presence of embolic material in the RA was diagnosed. Due to radiological artifacts, it was not possible to assess the burden of the thrombotic component. Anticoagulant treatment with enoxaparin was initiated at a dose adjusted to anti‑Xa activity, due to high bleeding risk caused by advanced liver cirrhosis complicated with coagulopathy and thrombocytopenia. After 1 week of anticoagulation, a control TTE showed the same findings in the RA. It was impossible to remove the pathological mass with percutaneous techniques because of its diameter (32 French) and the potential risk of atrial wall or tricuspid valve damage. Cardiac surgery under extracorporeal circulation was considered by a multidisciplinary team. However, in view of the existing comorbidities, especially liver cirrhosis, periprocedural risk was considered too high.
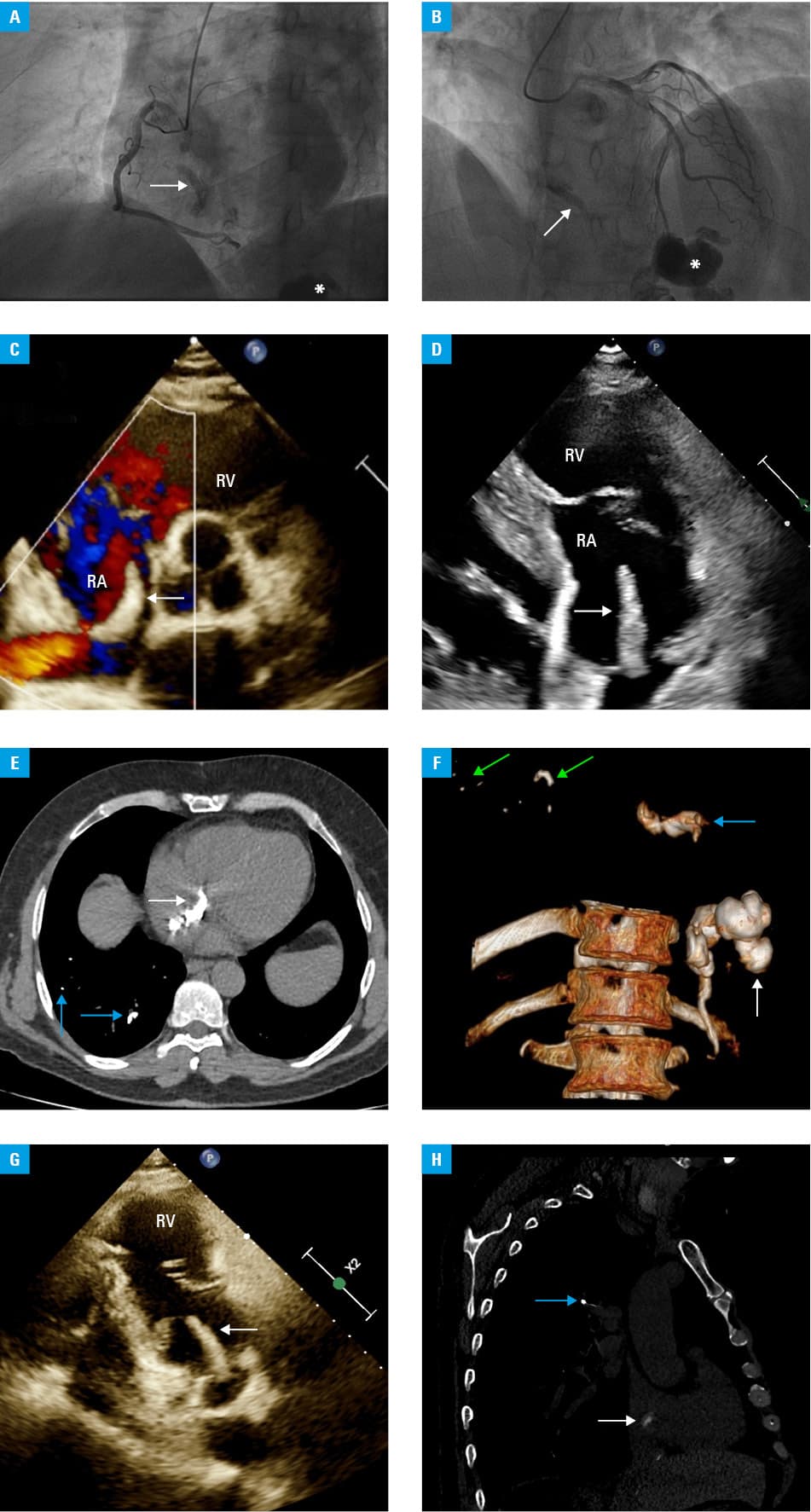
Abbreviations: RA, right atrium; RV, right ventricle
Shortly after, liver function deteriorated. The decision to accelerate the qualification for organ transplantation was reached, and urgent liver transplantation was performed in the usual manner shortly after. On control TTEs performed on the 4th and 40th day postsurgery, the additional structure in the RA remained unchanged (Figure 1G). There were no echocardiographic signs suggestive of pulmonary hypertension. Anticoagulation was continued with apixaban at a dose of 2.5 mg orally twice daily. The patient was discharged in a stable condition and is under surveillance in the outpatient setting. Although surgical removal of the RA mass by cardiac surgeons was planned, the patient did not consent to the procedure, and he has remained stable at the 6‑month follow‑up (Figure 1H).
Esophageal and gastric varices are a common complication of liver cirrhosis. In the event of bleeding, endoscopic treatment is required, including obliteration with cyanoacryl.1 Symptomatic pulmonary embolism with cyanoacrylic masses is a rare but well‑known complication.2 Only a few reports describe the presence of embolic material in the RA.3 Although recommendations for severity assessment and risk stratification for pulmonary thromboembolism appear to be applicable,4 there are no defined recommendations for the management of a foreign‑body embolism. Guidelines of the European Society of Cardiology suggest that foreign bodies should be removed due to the risk of thrombosis progression and sepsis.5
The presented case shows that even large emboli in the RA and pulmonary arteries may be asymptomatic. It is necessary to individualize the therapy based on a multidisciplinary council. Despite the extent of the surgery and comorbidities, eventually the acrylic material did not influence the clinical course of the patient.
- Angeli P, Bernardi M, Villanueva C, et al. EASL clinical practice guidelines for the management of patients with decompensated cirrhosis. J Hepatol. 2018; 69: 406‑460. | Crossref
- Pietrasik A, Gąsecka A, Chojecka D, et al. Iatrogenic pulmonary embolism with cyanoacrylate — to remove, or to leave? Kardiol Pol. 2021; 79: 706‑707. | Crossref
- Miyakoda K, Takedatsu H, Emori K, et al. N‑butyl‑2‑cyanoacrylate (histoacryl) glue in the right atrium after endoscopic injection for a ruptured duodenal varix: complication of histoacryl injection. Dig Endosc. 2012; 24: 192. | Crossref
- Pruszczyk P, Skowrońska M, Ciurzyński M, et al. Assessment of pulmonary embolism severity and the risk of early death. Pol Arch Intern Med. 2021; 131: 16134. | Crossref
- Konstantinides SV, Meyer G, Becattini C, et al. The 2019 ESC guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J. 2019; 40: 3453‑3455. | Crossref
ARTICLE INFORMATION