Abdominal manifestations of SARS-CoV-2 infection in a patient with acute-on-chronic hepatitis



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Abdominal manifestations of SARS-CoV-2 infection in a patient with acute-on-chronic hepatitis
COVID‑19–associated liver injury is defined as any liver damage that occurs during the disease progression in patients with or without pre‑existing liver disease. Further studies are needed to better understand the hepatic manifestations of COVID‑19 in patients with pre‑existing liver diseases and those with poor liver reserve.
A 44‑year‑old man with hepatitis B virus (HBV)-induced cirrhosis (Child–Pugh score A) required hospitalization for febrile diarrhea, abdominal pain, increased levels of inflammatory parameters, pancytopenia, and ascites. On admission, the polymerase chain reaction test of a nasopharyngeal swab sample was positive for SARS‑CoV‑2. There was no radiologic evidence of pneumonia; however, cirrhotic hepatic dysmorphia, portal hypertension with hypertrophy of the left liver lobe (segment I), and mild ascites were found. Thoracic angiography excluded pulmonary embolism. Serologic tests were performed, and the results were negative for the other types of hepatitis, as well as cytomegalovirus, HIV, and Epstein–Barr virus infections. The patient was immunocompetent, reported no excessive alcohol consumption, and his outpatient pharmacotherapy comprised β-blockers and tenofovir. 18F‑fluorodeoxyglucose positron emission tomography / computed tomography (18F‑FDG‑PET/CT) showed an unusual heterogeneous uptake in the right lobe of the liver (segment IV), with a maximum standard uptake value of 4.8, mild uptake in the right subcarinal lymph node, moderate splenomegaly with very mild uptake, diffuse and mild bone marrow uptake, and no 18F‑FDG uptake in the ascitic fluid (Figure 1A–1C). In line with these findings, liver biopsy revealed cirrhosis, increased inflammatory infiltrate consisting of numerous polynuclear cells (mainly neutrophils), and acute suppurative cholangitis. Classic serial sections stained with hematein‑eosin‑saffron did not show viral inclusion. No HBV reactivation was found, and other causes of hepatitis were excluded. Later, a contrast‑enhanced CT scan showed terminal ileocolitis. SARS‑CoV‑2 viral particles were found in the stool and ascitic fluid. The level of C‑reactive protein was elevated to 253 mg/l (reference range <5 mg/l) (Figure 1D), and alanine aminotransferase as well as conjugated bilirubin levels were increased up to 3‑fold within 2 weeks of admission (Figure 1E). Alkaline phosphatase activity was increased 9‑fold and γ-glutamyl transferase level was increased 15‑fold 2 weeks post the 18F‑FDG‑PET/CT scan, suggesting hepatic cholestasis (Figure 1D). The patient received steroids and tocilizumab along with intensive symptomatic treatment. He made a full recovery and was discharged home 1 month after admission. A 10‑month follow‑up 18F‑FDG‑PET/CT was unremarkable (Figure 1F).
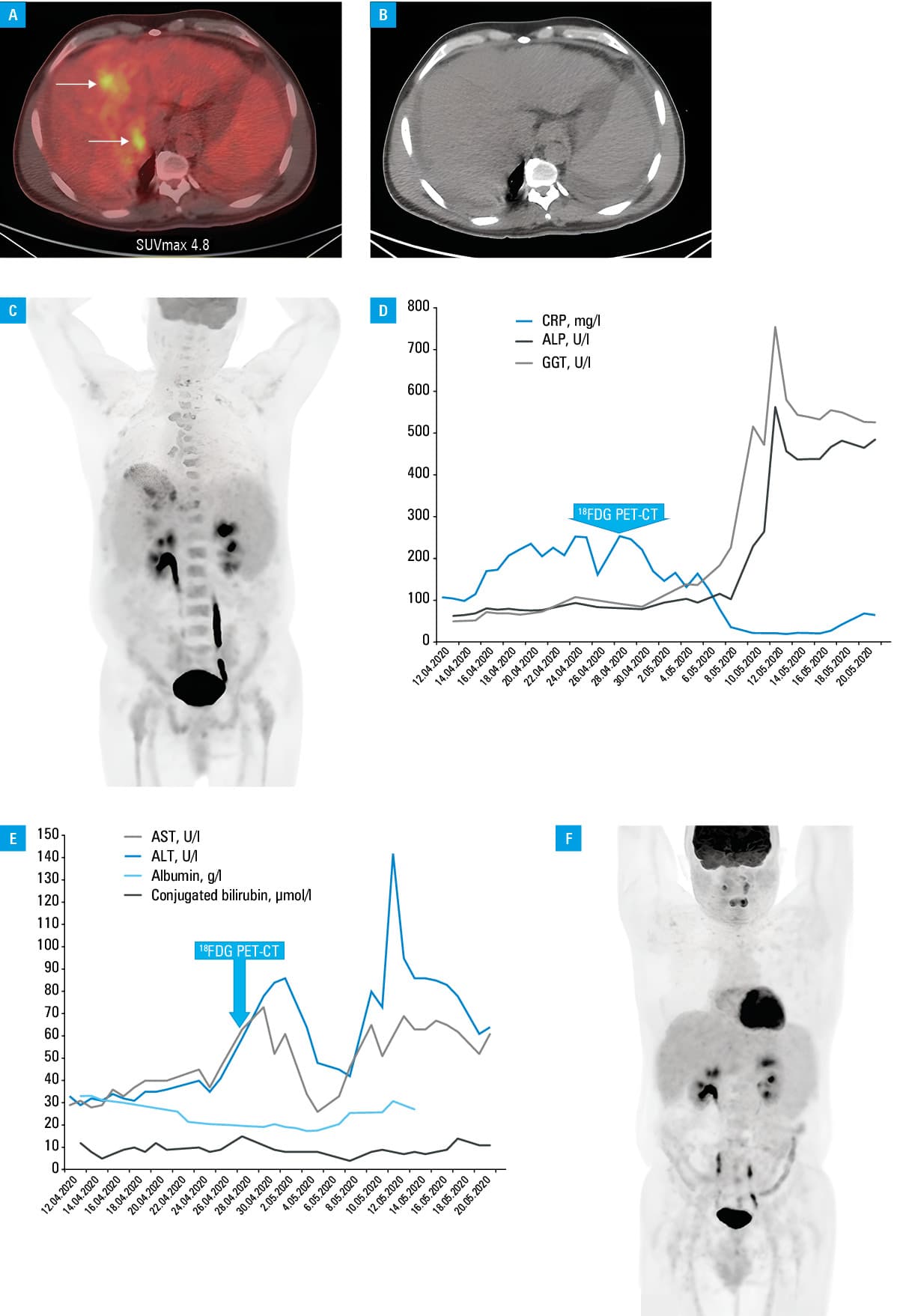
Abbreviations: ALT, alanine aminotransferase; ALP, alkaline phosphatase; AST, aspartate aminotransferase; CRP, C‑reactive protein; GGT, γ-glutamyl transferase
We report a new case of severe COVID‑19–associated liver injury.1 The novelty of this case is the unusual 18F‑FDG uptake in the liver, which may be related to infection of the liver with SARS‑CoV‑2. The absence of viral inclusion or specific liver damage found on liver biopsy does not exclude this diagnosis,2 and more pathological examinations would be needed. SARS‑CoV‑2 might enter the liver through the digestive tract, since angiotensin‑converting enzyme type 2 (ACE2) receptors, to which SARS‑CoV‑2 has an affinity, are found in great abundance on the intestinal epithelial cells.2 The ACE2 receptors are also highly expressed on cholangiocytes, and much less on hepatocytes. In a meta‑analysis by Wong et al,3 fecal SARS‑CoV‑2 was commonly found in infected patients. Alternatively, SARS‑CoV‑2 may enter the liver via the systemic viral circulation, due to viral secretion into the intestinal tract through cholangiocytes.4 Digestive infections tended to be more frequent in patients with severe forms of COVID‑19, particularly in those who required mechanical ventilation or died.5 Our patient developed a purely gastrointestinal and hepatobiliary manifestation of COVID‑19, and this contributed to his positive outcome.5 Isolated extrapulmonary manifestations of COVID‑19 are increasingly common. Our case shows that severe isolated liver decompensation can occur in a previously well‑compensated cirrhotic patient during SARS‑CoV‑2 infection. Intensive symptomatic and etiologic treatment can efficiently restore normal liver function. To our knowledge, this is the first case of 18F‑FDG‑PET/CT liver uptake due to COVID‑19–related hepatic injury with acute‑on‑chronic hepatitis in a patient with HBV‑induced liver cirrhosis who developed abdominal and hepatobiliary COVID‑19 manifestations.
- Li Y, Li C, Wang J, et al. A case series of COVID‑19 patients with chronic hepatitis B virus infection. J Med Virol. 2020; 92: 2785‑2791. | Crossref
- Asselah T, Durantel D, Pasmant E, et al. COVID‑19: discovery, diagnostics and drug development. J Hepatol. 2021; 74: 168‑184. | Crossref
- Wong MC, Huang J, Lai C, et al. Detection of SARS‑CoV‑2 RNA in fecal specimens of patients with confirmed COVID‑19: a meta‑analysis. J Infect. 2020; 81: e31‑e38. | Crossref
- Zhao B, Ni C, Gao R, et al. Recapitulation of SARS‑CoV‑2 infection and cholangiocyte damage with human liver ductal organoids. Protein Cell. 2020; 11: 771‑775. | Crossref
- Gupta A, Madhavan MV, Sehgal K, et al. Extrapulmonary manifestations of COVID‑19. Nat Med. 2020; 26: 1017‑1032. | Crossref
ARTICLE INFORMATION