Nonsteroidal anti-inflammatory drug–exacerbated respiratory disease: diagnosis and current management
Key words: aspirin, asthma, chronic rhinosinusitis with nasal polyposis, nonsteroidal anti-inflammatory drug–exacerbated respiratory disease, nonsteroidal anti-inflammatory drugs



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Nonsteroidal anti-inflammatory drug–exacerbated respiratory disease: diagnosis and current management
Nonsteroidal anti‑inflammatory drug–exacerbated respiratory disease (N‑ERD) is a unique and often clinically severe disease affecting a subgroup of adults with asthma, chronic rhinosinusitis with nasal polyposis, and respiratory reactions with exposure to all cyclooxygenase 1–inhibiting nonsteroidal anti‑inflammatory drugs. N‑ERD has a high disease burden and is estimated to affect 7% of adults with asthma and 30% of patients who have both asthma and nasal polyps. The disease is underdiagnosed and underrecognized by physicians on a routine basis, which leads to a delay in appropriate management. The goal of this review is to focus on the disease recognition, diagnosis, and different modes of up‑to‑date therapies, including medical management, surgical intervention, aspirin desensitization, and biologic therapy.
Introduction
Nonsteroidal anti‑inflammatory drug–exacerbated respiratory disease (N‑ERD) is a unique and often clinically severe disease affecting a subgroup of adults with asthma, chronic rhinosinusitis with nasal polyposis (CRSwNP), and respiratory reactions with exposure to all cyclooxygenase 1 (COX‑1)-inhibiting nonsteroidal anti‑inflammatory drugs (NSAIDs).1 Soon after the discovery of aspirin by Felix Hoffmann in 1897, reports surfaced of adverse reactions to acetylsalicylic acid (ASA). Widal et al2 first described the symptoms of N‑ERD in 1922. In the United States (US), it is more commonly referred to as aspirin‑exacerbated respiratory disease, which more accurately reflects a key difference between ASA and other NSAIDs, namely that aspirin therapy after desensitization (ATAD) can control the disease, whereas treatment with other NSAIDs is not disease modifying. N‑ERD is estimated to affect 7% of adults with asthma and up to 30% of patients with concurrent diagnoses of asthma and nasal polyps.3 It is very likely that the disease is underdiagnosed and underrecognized by physicians.4 This has real implications in clinical outcomes for these patients. This paper will focus on the disease recognition and management.
Nonsteroidal anti‑inflammatory drug–exacerbated respiratory disease: demographics and comorbidities
Patients with N‑ERD commonly present in the third or fourth decade of life with chronic nasal obstruction, nasal polyps, and anosmia that begin after what they perceive as a head cold.5 Women are slightly more predisposed to N‑ERD than men.6 Although the genetics of the disease has not been firmly established, a Finnish study7 indicated there may be a component of genetic susceptibility. Similarly, a potential link between N‑ERD and the HLA-DRB1 locus was found across cohorts with different ethnic backgrounds, but a true genetic association has not been conclusively proven.8-11 The exceedingly variable phenotype of N‑ERD makes this task a difficult endeavor.12
Regarding atopy, a clear association between nasal allergies and N‑ERD has not been established despite elevated rates of N‑ERD patients with immunoglobulin E (IgE)-mediated aeroallergen sensitivity.13 Similarly, N‑ERD is associated with only modest eosinophilia, which is explained by trafficking of eosinophils out of the vasculature and to the site of inflammation.14 More recently, Sanak et al15 have found that blood eosinophil counts are not a precise surrogate marker of sputum eosinophilia, proposing a consideration that N‑ERD is more of a heterogenous condition, rather than purely a type 2 inflammation–associated ailment. We will discuss these recent findings below, as this shift in concepts regarding N‑ERD may alter potential therapy modalities.
Presentation of nonsteroidal anti‑inflammatory drug–exacerbated respiratory disease
Sensitivity to COX‑1 inhibitors can occur at any time point in the disease course and has a variable symptom onset.16 Upon exposure to NSAIDs, severe respiratory symptoms develop within 30 minutes to 3 hours from ingestion. To make the diagnosis, chronic sinusitis has to be present in addition to the sensitivity to COX‑1 inhibitors. N‑ERD is overrepresented in patients with severe asthma, leading to significant morbidity—increased rates of intubation, need for systemic corticosteroids, and lower lung function.17 There is higher morbidity associated with the sinus disease as well as with increased need for sinus surgery, aggressive regrowth of polyps after surgery, and impact on quality of life due to anosmia.18
The pathophysiology of N‑ERD is still being unraveled. From a macro perspective, it is characterized by dysregulation of the arachidonic acid pathway, leading to overproduction of proinflammatory cysteinyl leukotrienes and a prostanoid prostaglandin (PG) D2, as well as by lower levels of the anti‑inflammatory prostanoid PGE2, among other abnormalities. Ingestion of a COX‑1–inhibiting NSAID abruptly blocks the limited production of PGE2, leading to the stereotypical reaction mediated by leukotrienes and mast cell mediators, which can include nasal congestion, rhinorrhea, ocular chemosis, cough, chest tightness, along with an abrupt drop in forced expiratory volume during the first second of expiration (FEV1). These reactions can be potentially fatal if the patient is unaware of the diagnosis.6 Understanding the pathomechanisms of N‑ERD can allow for specific interventions to control the severe eosinophilic airway disease. Patients can also experience an increased sensitivity to ingestion of alcohol, leading to respiratory tract symptoms.19 This can be used as a clinical clue that the patient has N‑ERD.
Diagnosis
Making the diagnosis of N‑ERD requires detailed history‑taking, confirmation of chronic rhinosinusitis with / without nasal polyposis via imaging or direct visualization, and a history of acute respiratory symptoms 30 minutes to 2 hours after exposure to COX‑1 inhibitors in a patient with a history of adult‑onset asthma.16 Relying purely on medical history may not lead to accurate diagnosis, and an oral challenge with aspirin remains the gold standard diagnostic test.20 Having said that, we do recognize that not all patients have access to, and not all providers have the capabilities of conducting oral aspirin challenges. In those instances, a clinical diagnosis is sufficient. Table 1 illustrates the checklist to diagnose N‑ERD.21-23
Abbreviations: ASA, acetylsalicylic acid; EU, Europe; NSAID, nonsteroidal anti‑inflammatory drug, N‑ERD, nonsteroidal anti‑inflammatory drug–exacerbated respiratory disease; US, United States |
|
Multiple protocols for diagnostic ASA/NSAID challenges have been published. There is a lack of consensus between the US and European approaches to oral aspirin provocation from a logistic standpoint. No matter the approach, oral aspirin is the gold standard for diagnosing hypersensitivity to all NSAIDs. We highlight both the US and European (European Academy of Allergy and Clinical Immunology [EAACI]) methods in Tables 2 and 3, respectively. Alternatively, intranasal challenges (with lysine‑aspirin [Europe] or intranasal ketorolac [US]), highlighted in Table 4, are less sensitive than the oral ones, but they are safer and can be used in a patient with contraindications to an oral challenge.21,24
Time | Day 1abc | Day 2 | Day 3 |
a Placebo can be skipped if the patient’s baseline forced expiratory volume during the first second of expiration is the same as their previous best with the absence of albuterol use in the previous week.
b Controller inhalers, such as inhaled corticosteroid (ICS) or ICS / long‑acting β-agonists, should be continued to minimize the risk of bronchospasm.
c Leukotriene receptor antagonists should be continued 2–4 weeks prior to the challenge to minimize the risk of bronchospasm.
d If a patient does not react to 325 mg of ASA over a span of 3 hours, the the challenge is considered negative. | |||
8 AM | Placebo | 20–40 mg | 100–160 mg |
11 AM | Placebo | 40–60 mg | 160–325 mg |
2 PM | Placebo | 60–100 mg | 325 mgd |
Time | Day 1abc | Day 2 |
a If the forced expiratory volume during the first second of expiration varies by >15% from the baseline value during the placebo challenge, the patient is deemed unstable and cannot proceed with the challenge.
b Controller inhalers, such as inhaled corticosteroid (ICS) or ICS / long‑acting β-agonists, should be discontinued for at least 24 hours prior to the challenge.
c Leukotriene receptor antagonists should be discontinued 1 week prior to the challenge.
d In a patient with a high index of suspicion for aspirin hypersensitivity, 500 mg is an optional extra dose if no reaction is elicited. | ||
0 | Placebo | 10 mg |
+1.5–2 h | Placebo | 27 mg |
+1.5–2 h | Placebo | 44 mg |
+1.5–2 h | Placebo (optional) | 117 mg |
+1.5–2 h | – | 312 mg |
+1.5–2 h | – | 500 mgd |
Step | Instructions | Positive reaction? |
0 | To prepare intranasal lysine‑aspirin dissolve 1 sachet of lysine‑aspirin 500 mg in 10 ml of normal saline. | – |
1 | Administer normal saline (80 µl to each nostril). Baseline readings should be repeated 3 times at 10‑minute intervals. |
|
2 | Administer L‑ASA (80 µl to each nostril; equivalent to 16 mg of aspirin) for 1 minute. Readings should be repeated every 10 minutes for 2 hours. |
|
3 | Postchallenge instructions | |
| ||
Optimizing challenges
Challenges should be performed in a specialized clinical setting (either outpatient or inpatient) by experienced physicians and nurses. Spirometry must be done to confirm the current respiratory status of the patient (FEV1 >70% in the patients with a baseline FEV1 >70%, or stable FEV1 in the patients with baseline FEV1 <70%). There are also certain contraindications to an oral challenge. The most significant one is uncontrolled asthma. According to the 2023 Global Initiative for Asthma (GINA) guidelines,25 uncontrolled asthma is defined using the Asthma Control Test (ACT) questionnaire. The ACT score ranges from 5 to 25, with higher scores (ie, ≥15 points) defining better‑controlled asthma, and lower scores (ie, <15 points) indicating uncontrolled asthma. Other contraindications include pregnancy, recent viral illness or exacerbation of asthma within 4 weeks of the challenge, current use of a β-blocker, and / or a history of a bleeding disorder. Contraindications to a nasal challenge include an upper respiratory viral illness within 4 weeks of the challenge and / or a nasal pathology that precludes a nasal challenge.22
The nasal challenge involves the administration of intranasal medications in increasing doses until achieving the desired effect. A major difference between the US and European methods involves whether or not to pretreat the patient with specific medications. This applies to both nasal and oral challenges. In the US, pretreatment with leukotriene modifiers 2 to 4 weeks prior to the challenge has been shown to decrease the asthmatic response, and is considered potentially beneficial to maximize safety.26 Similarly, another safety measure to prevent bronchospasm is to continue controller inhalers, such as inhaled corticosteroids with or without long‑acting bronchodilators. These recommendations are highlighted by the 2021 Work Group Report from the Rhinitis, Rhinosinusitis and Ocular Allergy Committee of the American Academy of Allergy, Asthma and Immunology.24 As discussed earlier, not all patients with N‑ERD may have asthma at baseline, and challenges may provoke a significant respiratory response. These interventions are performed to shift the provocative response away from the lower airway and maximize the safety of aspirin challenges.26 On the other hand, the EAACI guidelines recommend withdrawal of drugs such as bronchodilators and leukotriene modifiers prior to the provocation challenge to remove any potential of a blunted response to aspirin.16 The recent 2022 Drug Allergy Practice Parameter update27 highlights other factors to keep in mind prior to initiating an aspirin challenge, such as recent nasal polypectomy and concurrent omalizumab therapy, which may lead to negative challenges in a selected number of patients.
The diagnosis of N‑ERD is confirmed if aspirin provocation induces upper and / or lower respiratory tract symptoms (laryngospasm, bronchospasm, decrease in the nasal flow rate by 20% and / or decrease in FEV1 by 15%), conjunctivitis, and / or rhinitis. A patient’s FEV1 should be measured every 60 minutes (US) or every 90 to 120 minutes (Europe).21,24 Treatment of the symptoms provoked and careful postprocedural monitoring must also be implemented, depending on the severity of the reaction. A drug challenge can be followed by aspirin desensitization with a target dose of 325 to 1300 mg. This is one of the methods to manage N‑ERD that we will discuss in more detail below.24
Management
The management of N‑ERD can vary from case to case. There are more treatment options now, with the advent of monoclonal antibody therapy for severe asthma and CRSwNP. Treatment is determined by disease severity, patient preference, and logistic considerations, such as accessibility and cost.
Treatment for all individuals with N‑ERD includes NSAID avoidance, and for the patients who are sensitive, avoidance of alcohol. Patients should be provided with a list of commonly encountered NSAIDs, including both topical and ingested agents. Standard of care for CRSwNP and asthma comprises the use of topical steroids, long‑acting β-agonists, leukotriene modifiers, and short courses of oral corticosteroids when indicated. In patients who continue to have worsening symptoms, poor quality of life, and require treatment with systemic corticosteroids, options such as sinus surgery, debulking polyp surgery followed by aspirin desensitization, and biologic therapy (with or without surgery) can be considered.
All patients with diagnosed or suspected N‑ERD should practice strict avoidance of COX‑1–inhibiting medications. The likelihood of a cross‑reaction is directly proportional to their COX‑1 inhibition potency. Highly selective COX‑2 inhibitors, such as celecoxib, are generally well tolerated by N‑ERD patients.28 Some NSAIDs, such as meloxicam and nimesulide, are selective COX‑2 inhibitors at lower doses, but can have modest COX‑1 inhibitory effects at higher doses.29,30 These are further illustrated in Table 5. Additionally, individuals who experience exacerbations after exposure to alcohol should practice alcohol avoidance. Medical management of both respiratory and nasal symptoms should be optimized.
Highly selective COX‑1 inhibitors | Weakly selective COX‑1 inhibitors | Highly selective COX‑2 inhibitors | COX‑2 inhibitors with COX‑1 inhibition at high doses |
Acetylsalicylic acid, antipyrine / benzocaine, benoxaprofen, flurbiprofen, ibuprofen, indomethacin, metamizole, mefanamic acid, diclofenac, ketoprofen, fenoprofen, naproxen, piroxicam, oxaprozin, tolmetin, meclofenamate, etodolac, ketorolac | Acetaminophen, choline magnesium trisalicylate, salsalate, diflunisal | Celecoxib, etoricoxib, parecoxib, lumiracoxib | Meloxicam, nimesulide, nabumetone |
Asthma should be managed in a stepwise fashion following the GINA guidelines.24 Topical therapy with an inhaled corticosteroid in addition to a long‑acting bronchodilator is sufficient in a majority of N‑ERD patients.16 CRSwNP can be more challenging to control. Topical mometasone 2 sprays twice a day is the approved treatment for nasal polyposis. If this is not effective, topical budesonide in the form of lavage or nebulization can be used to control polyp growth, but this treatment is off‑label and often difficult to access. Nasal saline irrigation may also help alleviate symptoms by washing away irritants, and should be used daily prior to the delivery of medicated sprays.
Fluticasone in the form of exhaled delivery system–fluticasone (EDS‑Flu) is indicated for nasal polyps and is more effective than the regular nasal steroid sprays. In the randomized, double‑blinded NAVIGATE I and II trials,31 it was shown that EDS‑Flu provided a clinically and statistically significant improvement in disease symptoms, polyp grade, and quality of life, as compared with placebo, in patients with CRSwNP. Oral corticosteroids may be necessary in short courses (2–3 weeks) to control severe nasal and potential concomitant respiratory symptoms. The rationale is to reduce the size of the polyps and allow better delivery of topical steroids.
Decades ago, Sladek and Szczeklik32 reported an overproduction of cysteinyl leukotrienes in N‑ERD patients, as well as a positive correlation between the production of cysteinyl leukotrienes (measured by urinary leukotriene E4 [LTE4]) and symptoms of bronchoconstriction, increased vascular permeability, bronchial secretions, and increased proliferation and attraction of inflammatory cells. Because of this, leukotriene modifiers have been used in conjunction with topical steroids.26 Ta and White19 found cysteinyl leukotriene receptor 1 blockers, such as montelukast and zafirlukast, as well as a 5‑lipoxygenase inhibitor zileuton, to be an effective add‑on therapy in a majority of analyzed patients with N‑ERD. On the other hand, some studies have shown no difference in the clinical response between aspirin‑intolerant and aspirin‑tolerant patients treated with montelukast.33 For this reason, 5‑lipoxygenase inhibitors were explored as a potential add‑on treatment. Zileuton inhibits the synthesis of cysteinyl leukotrienes and has been shown to reduce the frequency of surgical intervention, but has not shown a significant benefit with respect to rhinological quality of life symptoms.34 Moreover, another study suggested that adding on zileuton could lead to better control of asthma, as compared with increasing the doses of corticosteroids alone. Because zileuton does not completely inhibit the synthesis of leukotrienes, it should be combined with montelukast / zafirlukast for greater impact. Clinicians who prescribe zileuton should be aware of the potential for transient transaminitis, and liver enzymes must be monitored at the onset of the therapy and every 3 months for the first year.35
When medical management fails to control the disease, further options are sinonasal surgery with continued pharmacotherapy, sinonasal surgery followed by ATAD, or biologic therapy. Indications for these treatment alternatives depend on the patient preference, comorbidities, and logistics, such as cost.
Sinonasal surgery involving polypectomy, functional endoscopic sinus surgery, ethmoidectomy, and bilateral frontal sinusotomy (via the Draf IIa, IIb, or III procedure36) is indicated in patients with uncontrolled symptoms or inadequate control of the disease despite maximum‑dose intranasal and oral corticosteroid therapy.37 Patients should be informed about the high risk of polyp regrowth after the surgery. A 2011 study18 showed that 90% of N‑ERD patients had polyp regrowth 5 years after the sinus surgery. Subsequent ATAD and biologic therapy helped with prevention of polyp regrowth.
It has been shown that sinus surgery followed by ATAD leads to improvement of quality of life via symptom scores, decreased regrowth of the polyps, lower reliance on systemic corticosteroids, prevention of subsequent sinus surgeries, and a reduction in asthma exacerbations.38 Debulking of polyps is necessary prior to ATAD, since aspirin therapy prevents polyp regrowth but does not resolve the polyps that are already present. Stopping aspirin therapy at any point after successful desensitization leads to a worsening of symptom scores and polyp recurrence.39
ATAD was first reported by White and Stevenson,40 who observed that prolonged aspirin courses led to an improvement of chronic rhinosinusitis and asthma in N‑ERD patients.40 A 2021 report from the Rhinitis, Rhinosinusitis, and Ocular Allergy Committee of the American Academy of Allergy, Asthma and Immunology24 highlights the role of aspirin desensitization in the management of N‑ERD and summarizes the supporting double‑blind, placebo‑controlled studies. ATAD is indicated when there is a lack of response to conservative topical treatments and high recurrence of nasal polyps, especially in the setting of surgical intervention, uncontrolled asthma despite maximal therapy, increased dependency on oral corticosteroids for either nasal or respiratory symptoms, need for antiplatelet therapy, or prevention of cardiovascular disease or stroke.
Factors predicting a positive response to ADAT can be explored prior to the treatment initiation. Examples include female sex, higher Sinonasal Outcome Test 22 scores at baseline, higher serum eosinophilic count, lower neutrophilic presence in sputum, higher sputum cell expression of the hydroxyprostaglandin dehydrogenase gene, lower sputum expression of the proteoglycan 2 gene, and higher plasma 15‑hydoxyeicosatetraenoic acid levels.41-43
Established protocols for region‑specific ADAT are illustrated in Tables 2 and 3. Once a positive response is elicited, the symptoms are treated. The same dose is then repeated once, with subsequent dose escalation until the maximum dose of 325 mg is reached. The final effective dosage is variable and can range from 650 to 1300 mg daily.24 Concomitant treatment with proton pump inhibitors and H2 blockers may be necessary to prevent and reduce adverse effects of aspirin therapy.44-46
Biologics / monoclonal antibody therapies are the most recent development in N‑ERD management. Since N‑ERD is mostly considered a type 2 inflammatory disease (ie, involving elevated blood and tissue eosinophils and elevated levels of interleukin [IL]-4, IL‑5, and IL‑13 leading to trafficking of eosinophils, lymphocytes, basophils, and mast cells to the sinonasal and pulmonary mucosa), type 2–targeted systemic therapy has been shown to lead to a much‑needed reduction of corticosteroid dependency. Since science is ever‑evolving, we continue to unearth more details that underlie N‑ERD. For example, macrophages have been implicated as possible culprit cells in N‑ERD, as they have been shown to produce higher levels of proinflammatory metabolites and upregulated cytokines after being challenged.47 Not only does our understanding of the disease from a type 2 inflammatory view continues to evolve—recent works have also uncovered an overall heterogenous inflammatory picture, with some patients exhibiting type 1 and type 3 inflammatory processes.48-51 Furthermore, it has been found that a number of effector cells may be involved in the N‑ERD process, including epithelial barrier dysfunction leading to the release of alarmins, such as thymic stromal lymphopoietin (TSLP), IL‑25, and IL‑33, as well as mast cells, resulting in the release of inflammatory eicosanoids.50-52 Future findings such, as those mentioned above, may allow for additional options for targeted therapy based on the patient’s biologic profile, and potentially the ability to predict the response to a particular therapeutic agent.
Currently, there are 3 approved biologics for the treatment of CRSwNP—omalizumab, which targets the fragment crystallizable region of IgE (dose, 74–600 mg subcutaneously every 2–4 weeks, based on IgE levels and body weight), dupilumab, which targets the α subunit of the IL‑4 receptor that modulates both the IL‑4 and IL‑13 pathways (dose, 300 mg subcutaneously every week), and mepolizumab, which targets IL‑5 (dose, 100 mg subcutaneously every 4 weeks). All of them are also approved for asthma treatment. These biologics and their targets are illustrated in Figure 1.
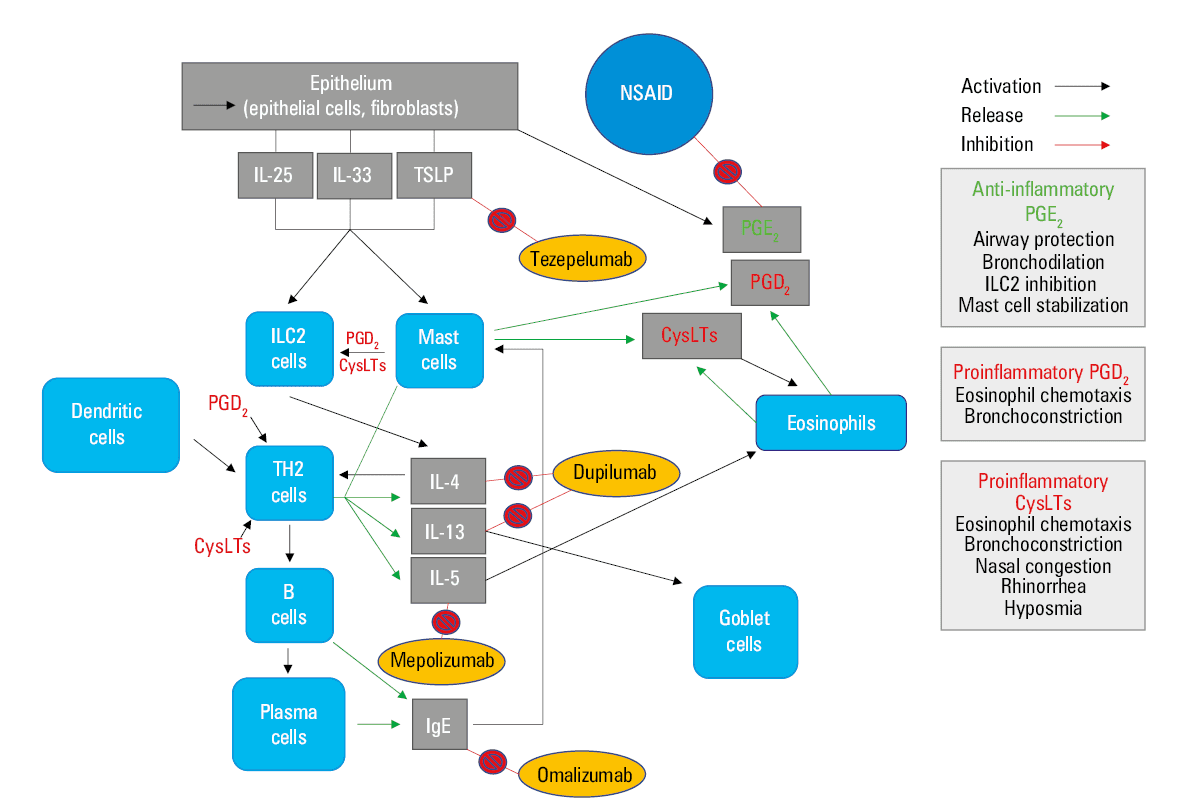
Abbreviations: CysLT, cysteinyl leukotriene; Ig, immunoglobulin; IL, interleukin; PG, prostaglandin; TSLP, thymic stromal lymphopoietin; others, see Table 1
With respect to omalizumab, the POLYP1 and POLYP2 clinical trials showed improved patient‑reported clinical symptoms as well as endoscopic findings, as compared with placebo, in the patients with CRSwNP.53 The limitation of this study when concerning N‑ERD patients was the small N‑ERD subgroup (n = 40). Additionally, another study showed inhibition of LE4 overproduction in patients treated with omalizumab 3 months prior to aspirin desensitization.54
Observations in a small cohort of N‑ERD patients enrolled in a phase 3 trial comparing the efficacy of dupilumab 300 mg every week with placebo in nasal polyposis have shown that this biologic improves both nasal polyp burden and asthma control in this specific group of patients.55 A recent retrospective study conducted at Scripps Clinic56 found that patients on dupilumab had a significantly improved rate of response to the therapy than those receiving omalizumab or mepolizumab. Another study on dupilumab showed rapid response with regard to sinonasal symptoms, sense of smell, and lung function. This was highlighted by improved epithelial barrier function evidenced by increased nasal PGE2, decreased nasal albumin, decreased urinary and nasal LTE4, and decreased nasal and serum IgE.57 Once again, it is worth repeating that all of these studies involved CRSwNP patients, and not individuals with N‑ERD specifically.
With respect to clinical trials on mepolizumab and anti–IL‑5 agents, there is weak efficacy in CRSwNP and, by extension, even weaker evidence for N‑ERD patients. This lack of response to anti–IL‑5 therapy comes to light given the recent novel findings regarding a multifactorial inflammatory process in N‑ERD as opposed to one mainly driven by type 2 inflammation.58
The European Forum for Research and Education in Allergy and Airway Diseases (EUFOREA) has released a consensus on how to approach this novel form of therapy.59 There are 5 criteria that EUFOREA has put forward when biologics are considered. Certain criteria must be met prior to initiating the biologic therapy, such as a history of surgery or lack thereof, as shown in Table 6.
|
History of surgery: 3 criteria required prior to therapy initiation |
No history of surgery: 4 criteria required prior to therapy initiation |
Once treatment is initiated, there is a variability with regard to what is defined as therapeutic response. EUFOREA defined measures of response as a reduction of nasal polyp size, reduced need for systemic corticosteroids, improved quality of life, improved sense of smell, and reduction of impact of comorbidities. There is a range of no response, poor response, moderate response, and excellent response when 0, 1–2, 3–4, and 5 criteria are met, respectively. When biologics are used as the therapy, patients should be evaluated after 16 weeks and 1 year of treatment.59 If none of the response criteria are met at either time point, the treatment should be discontinued. In the case of an excellent response to the therapy, less is known. There are no guidelines on when to discontinue the treatment after a positive response to biologic therapy, and more research on this topic is required.
Conclusions
N‑ERD is an acquired disease that we have known about for 100 years, but it is still not completely understood. Allergists, otolaryngologists, and pulmonologists have come together to find a way to manage patients with N‑ERD in the most safe and effective manner. For general practitioners, the lack of recognition of this disease is the emphasis of this paper. Sufficient knowledge of the pathophysiology and presentation of N‑ERD can prevent a delay in diagnosis, lead to appropriate specialist referral, and consequently, alleviate the disease burden. Practitioners must keep in mind the constellation of symptoms—the relationship between CRSwNP and asthma in addition to the exacerbation of symptoms with NSAID and alcohol use. Another consideration is rapid polyp regrowth after surgical polypectomies. If a patient presents in any manner described above, N‑ERD must be ruled out.
As for the management of the disease, treatment options have expanded in the last decade, with the advent of highly targeted biologic therapy focusing on type 2 inflammation. However, none of the biologics are approved specifically for N‑ERD. Other implicated immune pathways, such as IL‑25, IL‑33, and TSLP, are currently being studied for diseases driven by type 2 inflammation, and could lead to additional treatment options for N‑ERD in the future. For example, the PATHWAY study,60 a phase 2b clinical trial, showed decreased T2 markers in patients with severe uncontrolled asthma and comorbid CRSwNP, who were treated with an anti‑TSLP biologic tezepelumab.60 In light of the recent findings regarding the heterogenous nature of N‑ERD and non–type 2 inflammatory N‑ERD subtypes, the future may bring about targeted therapy outside the realm of type 2 inflammation. Further aspects of N‑ERD are being continuously explored, and future research will provide more clarity on the disease process, diagnosis, and management.
- Stevens WW, Cahill KN. Mechanistic and clinical updates in AERD: 2021‑2022. J Allergy Clin Immunol. 2023; 151: 1448‑1456. | Crossref
- Widal F, Abrami P, Lermoyez J. First complete description of the aspirin idiosyncrasy‑asthma‑nasal polyposis syndrome (plus urticaria)—1922 (with a note on aspirin desensitization). J Asthma. 1987; 24: 297‑300.
- Rajan JP, Wineinger NE, Stevenson DD, White AA, Prevalence of aspirin‑exacerbated respiratory disease among asthmatic patients: a meta‑analysis of the literature. J Allergy Clin Immunol. 2015; 135: 676‑681. | Crossref
- Dominas C, Gadkaree S, Maxfield AZ, et al. Aspirin‑exacerbated respiratory disease: a review. Laryngoscope Investig Otolaryngol. 2020; 5: 360‑367. | Crossref
- Stevenson DD, Szczeklik A. Clinical and pathologic perspectives on aspirin sensitivity and asthma. J Allergy Clin Immunol. 2006; 118: 773‑786. | Crossref
ARTICLE INFORMATION