The use of sacubitril / valsartan in Takotsubo syndrome with severe impairment of left ventricular systolic function



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
The use of sacubitril / valsartan in Takotsubo syndrome with severe impairment of left ventricular systolic function
Takotsubo syndrome (TS) is a cardiac entity known for over 30 years, but its treatment remains a major clinical problem. Recommendations for therapy, mainly pharmacologic, based on various research results, are ambiguous.1
A 71‑year‑old woman with obesity, type 2 diabetes mellitus, hypertension, hyperlipidemia, and paroxysmal atrial fibrillation, with suspected acute coronary syndrome, was transferred to our department from a local hospital. The patient had developed a severe resting retrosternal pain on the day before transfer, preceded by a stressful situation.
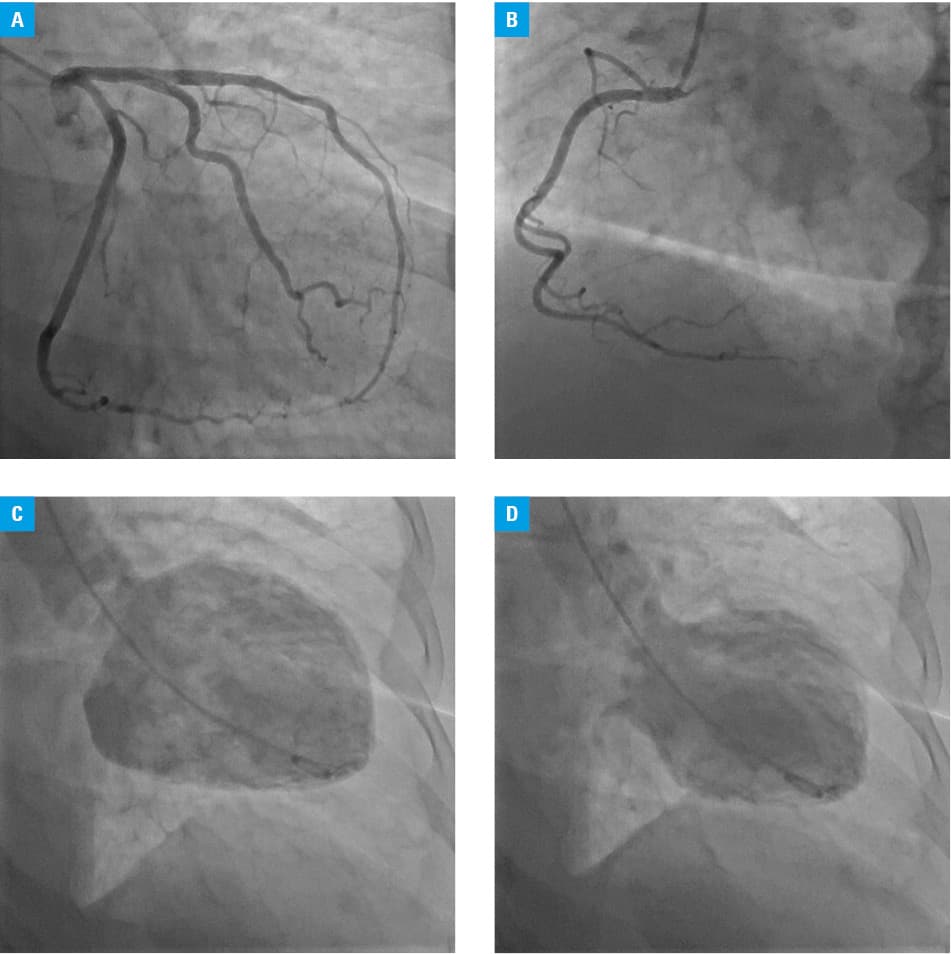
On admission, the patient remained hemodynamically stable and reported ongoing chest discomfort. Physical examination revealed extreme obesity (body mass index, 42 kg/m2) and blood pressure of 118/65 mm Hg. Electrocardiogram demonstrated sinus rhythm of 73/min, negative T wave in leads I, aVL, and V1–V4, and prolonged QTc of 504 ms. Echocardiography showed severely impaired left ventricular (LV) systolic function with ejection fraction (LVEF) of about 20%. The patient underwent coronary angiography, which showed no atherosclerotic lesions in the coronary arteries (Figure 1A and 1B), while ventriculography confirmed contractile dysfunction consistent with the apical variant of TS with the LVEF of 20% (Figure 1C and 1D). The patient was put on heart failure treatment as recommended (bisoprolol, ramipril, furosemide, eplerenone, empagliflozin), statins, and continued dabigatran, and antidiabetic treatment. On the second day of hospitalization, atrial fibrillation occurred and amiodarone was used without resolution of the arrhythmia. Due to probable interruption of anticoagulant therapy and the patient’s lack of consent for transesophageal echocardiography, she was qualified for elective cardioversion.
During hospitalization, the patient had recurrent retrosternal pain. A follow‑up echocardiogram performed on day 7 showed no improvement in LV systolic function, and therefore ramipril was replaced with sacubitril / valsartan. The patient was discharged home.
After 4 weeks, the patient was readmitted to the hospital. Her atrial fibrillation persisted, and electrical cardioversion successfully restored sinus rhythm. A follow‑up echocardiogram showed normal LV systolic function with LVEF of 55%. Due to complete resolution of contractile dysfunction, sacubitril / valsartan was discontinued and ramipril was restarted.
Some patients with TS develop severe damage to LV systolic function that lasts for several months. This increases the risk of serious complications and even death.
The angiotensin receptor antagonist and neprilysin inhibitor (ARNI, sacubitril / valsartan) is now well established in the treatment of severe heart failure; it improves LV contractility and increases patient survival.2
Excessive activation of the sympathetic nervous system is important in the pathophysiology of TS, so the use of sacubitril (a neprilysin inhibitor), which lowers catecholamine levels and reduces sympathetic activity, may be beneficial.3
Our case demonstrates the effectiveness of sacubitril / valsartan in faster recovery of severely impaired LV systolic function in TS. The patient showed no improvement in LV contractility after 1 week of hospitalization, so ARNI was implemented. After 4 weeks of treatment, complete resolution of contractile dysfunction was observed.
So far, the effectiveness of sacubitril / valsartan in the prevention of TS has only been proven in an experimental model,4 so randomized clinical trials on the use of ARNI in patients with severe LV damage in TS are needed.
- Medina de Chazal H, Del Buono MG, Keyser‑Marcus L, et al. Stress cardiomyopathy diagnosis and treatment. J Am Coll Cardiol. 2018; 72: 1955‑1971. | Crossref
- McMurray JJ, Packer M, Desai AS, et al. Angiotensin‑neprilysin inhibition versus enalapril in heart failure. N Engl J Med. 2014; 371: 993‑1004. | Crossref
- Sayer G, Kalantari S, Tayazime S, et al. Reduction of sympathetic innervation following transition to sacubitril / valsartan in the REMODEL (Reverse Remodeling Effects of Entresto) study. J Card Fail. 2018; 24: S32. | Crossref
- Ali A, Redfors B, Alkhoury J, et al. Sacubitril / valsartan decreases mortality in the rat model of the isoprenaline‑induced Takotsubo‑like syndrome. ESC Heart Fail. 2021; 8: 4130‑4138. | Crossref
ARTICLE INFORMATION