Endovascular management of iatrogenic aortic dissection using a minimally invasive method



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Endovascular management of iatrogenic aortic dissection using a minimally invasive method
Iatrogenic aortic dissection (IAD) constitutes 1% to 5% of acute type A aortic dissection cases. IAD is found in approximately 0.01% of patients during diagnostic coronary angiography, 0.19% of patients with acute myocardial infarction, 1.8% of individuals with chronic total occlusion, and in 0.5% of cases when the axillary or subclavian arteries are cannulated. Procedures such as transcatheter aortic valve implantation, thoracic endovascular aortic repair, and cross‑clamping during cardiac surgery may also cause IAD.1,2
A 65‑year‑old woman with a history of tobacco smoking (20 pack‑years), hypercholesterolemia, and hypertension with pronounced atherosclerotic alterations in the arterial branches emerging from the aortic arch was admitted to a vascular surgery department due to symptoms of impaired cerebral blood supply, particularly in the posterior cerebral circulation. The patient presented with a significant stenosis of the left subclavian artery, brachiocephalic trunk, and left common carotid artery, as well as a complete blockage of the right vertebral artery.
During the initial intervention (Figure 1A), the patient underwent angioplasty complemented by a stent (7 mm × 39 mm, Omnilink Elite, Abbott, Abbott Park, Illinois, United States) placement within the left subclavian artery. This procedure involved balloon angioplasty, which effectively mitigated the stenosis in the target left vertebral artery. Following successful intervention, the patient was discharged with a prescribed regimen of dual antiplatelet therapy (DAPT) (acetylsalicylic acid 1 × 75 mg once daily and clopidogrel 1 × 75 mg once daily), and a scheduled appointment for brachiocephalic trunk revascularization. Approximately 6 weeks later, a second intervention to remove the critical stenosis of the brachiocephalic trunk was undertaken. The procedure was initiated by predilatation via balloon catheters (Figure 1B and 1C), followed by a stent (7 mm × 39 mm, Omnilink Elite) insertion. However, subsequent angiography revealed the presence of retrograde flow in the ascending aorta, thus raising the suspicion of aortic dissection (Figure 1D). Further computed tomography angiography (CTA) confirmed the dissection with the entry point within the brachiocephalic trunk (Figure 1E). After an extensive consultation with a cardiac surgeon, interventional radiologist, and vascular surgeon, it was decided that due to DAPT, the patient’s comorbidities, and the location of the dissection entry, endovascular treatment was the optimal course of action. The dissection was finally treated by introducing a covered stent (8 mm × 37 mm, BeGraft Peripheral, Bentley InnoMed, Hechingen, Germany) through the right axillary artery. This technique effectively excluded the false lumen of the ascending aorta from the circulatory system (Figure 1F and 1G).
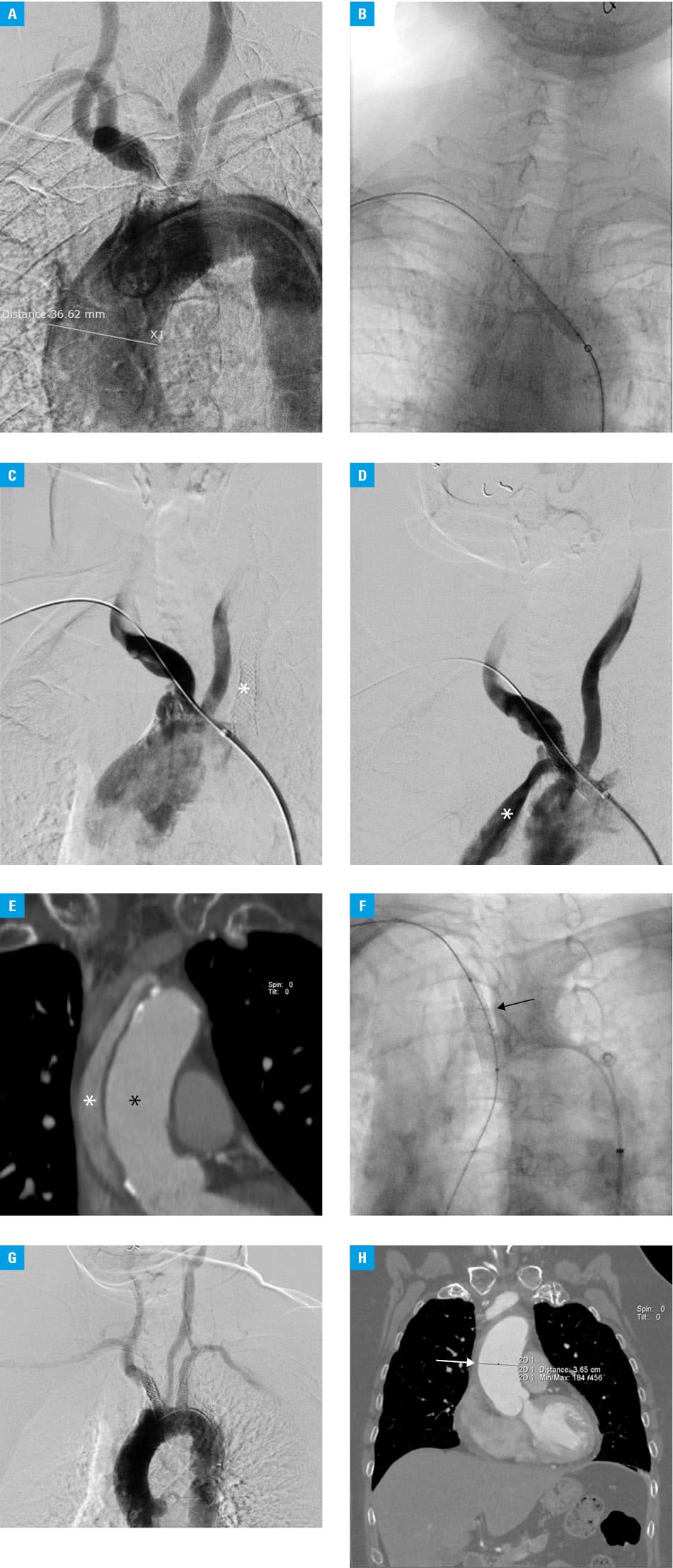
The follow‑up CTA on the fourth postoperative day (Figure 1H) confirmed successful resolution of the dissection, with only a small resorbing intramural hematoma present in the ascending aorta. An echocardiogram before discharge showed no abnormalities in the aortic valve. The patient was discharged on DAPT (acetylsalicylic acid 1 × 75 mg and clopidogrel 1 × 75 mg) on the eighth postprocedural day without any complaints. A follow‑up echocardiogram 3 months later showed that the intramural hematoma in the ascending artery was fully absorbed and abnormalities were visible.
IAD may present either without any symptoms or with pain, nausea and vomiting, hemodynamic deterioration or collapse, pericardial effusion and / or tamponade, cardiac arrhythmias, and even death during or after a procedure.1,2 Early diagnosis is essential for effective treatment as it enables a prompt preventive response before the consequences of aortic dissection occur.3,4
- Gudbjartsson T, Ahlsson A, Geirsson A, et al. Acute type A aortic dissection ‑ a review. Scand Cardiovasc J. 2020; 54: 1‑13. | Crossref
- Barış VÖ, Asil S, Çelik M, et al. Iatrogenic type A aortic dissection during percutaneous coronary intervention: a single‑center experience. Turk Kardiyol Dern Ars. 2021; 49: 108‑119.
- Ram H, Dwarakanath S, Green AE, et al. Iatrogenic aortic dissection associated with cardiac surgery: a narrative review. J Cardiothorac Vasc Anesth. 2021; 35: 3050‑3066. | Crossref
- De Viti D, Dambruoso P, Izzo P, et al. Iatrogenic acute aortic dissection in the era of minimally invasive cardiac surgery ‑ experience of a center and review of literature. Braz J Cardiovasc Surg. 2021; 36: 691‑699. | Crossref
ARTICLE INFORMATION