Ectopic, CRH-responsive Cushing syndrome with negative 68Ga-DOTATATE and 18F-FDG PET/CT imaging findings and pituitary microadenoma: a challenging case with a successful outcome



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Ectopic, CRH-responsive Cushing syndrome with negative 68Ga-DOTATATE and 18F-FDG PET/CT imaging findings and pituitary microadenoma: a challenging case with a successful outcome
Ectopic Cushing syndrome (ECS) is responsible for 9% to 18% of Cushing syndrome cases, and its clinical manifestation ranges from undetectable benign lesions to metastatic malignancies, very often presenting with severe, life‑threatening hypercortisolemia.1 The differential diagnosis of ECS can be extremely challenging and requires careful clinical, biochemical, and radiological investigation.1,2
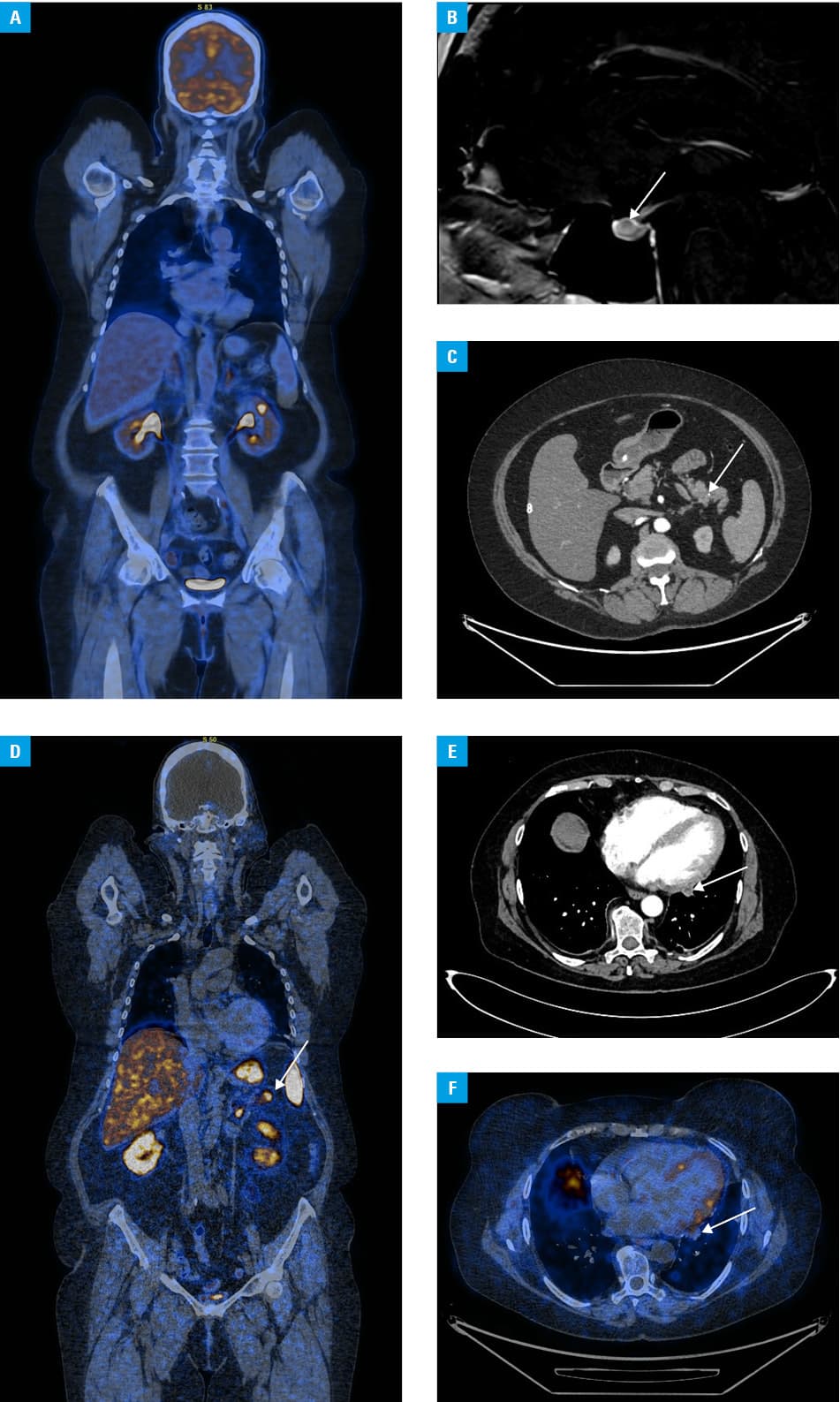
We present a very rare case of a woman with ECS and pituitary incidentaloma caused by a lung carcinoid, who responded to the corticotropin‑releasing hormone (CRH) stimulation test mimicking Cushing disease (CD), and whose lung carcinoid did not show pathological tracer uptake on repeated 68Ga‑DOTA‑0‑Tyr3‑Octreotate (DOTATATE) and 18F‑fluorodeoxyglucose positron emission tomography / computed tomography (PET/CT) imaging (Figure 1A). She had been diagnosed with adrenocorticotropic hormone (ACTH)-dependent hypercortisolemia (ACTH, 408.4 pg/ml; reference range [RR], 7.2–63.3 pg/ml; cortisol in 24‑h urine collection, 466.8 μg/24 h; RR, 4.3–176 μg/24 h; high nocturnal cortisol, 15.7 μg/dl; RR <1.8 μg/dl) in 2019. The CRH test showed an increase in ACTH and cortisol levels by 31% and 23%, respectively; however, there was no suppression of the serum cortisol level (17.4 μg/dl) in the 8‑mg dexamethasone test, which is characteristic of CD. Pituitary magnetic resonance imaging (MRI), thoracic and abdominal CT, colonoscopy, bronchoscopy, as well as 68Ga‑DOTATATE and 18F‑FDG PET/CT findings were unremarkable. Since 2019, the patient has been treated with ketoconazole, followed by osilodrostat (4 mg daily). Multiple diagnostic procedures were repeated in 2022. Again, in the CRH test, the cortisol and ACTH levels rose by 31% and 38%, respectively. Pituitary MRI revealed a microadenoma (8 mm × 2.5 mm × 2.5 mm) (Figure 1B). However, bilateral inferior petrosal sinus sampling (BIPSS) was not suggestive of CD. On CT, calcification of the pancreas was found (Figure 1C), whereas 68Ga‑DOTATATE PET/CT revealed a pathologic expression of somatostatin receptors in the uncinate process of the pancreas (Figure 1D). A distal pancreatectomy was performed (June 2022), revealing intraductal papillary mucinous neoplasms. Hypercortisolemia persisted after the surgery. Finally, after repeated radiological consultations of the CT scans, a peripleural lung tumor (13 mm × 10 mm × 8 mm) drew attention as suspicious. The tumor has been present since 2019 (Figure 1E). It did not progress over time, and showed no pathological tracer uptake on either 68Ga‑DOTATATE (Figure 1F) or 18F‑FDG PET/CT; therefore, it was initially considered clinically irrelevant. A multidisciplinary tumor board found the patient eligible for wedge‑peripheral resection of the lower lobe of the left lung. A typical carcinoid was found (neuroendocrine tumor [NET] grade 1; Ki67, 2.5%). After the surgery, hydrocortisone supplementation was started.
Carcinoids and well‑differentiated NETs in the bronchi are the most common causes of ECS. However, the localization of the lesion remains occult in up to 20% of ECS cases, and requires multiple repetitions of the diagnostic procedures.3,4 Distinguishing between CD and ECS is often challenging. Results of some dynamic hormonal tests in the patients with ECS, especially those with small lung NETs, can mimic the results observed in patients with CD due to the expression of vasopressin V2, V1b (V3), and CRH receptors.1 As nearly 10% of the population can have a nonfunctional microadenoma,1 its presence is not equivalent to CD. BIPSS has the highest sensitivity and specificity (approximately 94%) for ruling out CD.2 Our case also shows that osilodrostat seems to be an effective and convenient treatment for severe hypercortisolism in ECS.3,5 To understand the natural history of ECS and to set the standards of care, further multicenter studies are warranted.
- Young J, Haissaguerre M, Viera Pinto O, et al. Management of endocrine disease: Cushing syndrome due to ectopic ACTH secretion: an expert operational opinion. Eur J Endocrinol. 2020; 182: R29‑R58. | Crossref
- Ilias I, Torpy DJ, Pacak K, et al. Cushing’s syndrome due to ectopic corticotropin secretion: twenty years’ experience at the National Institutes of Health. J Clin Endocrinol Metab. 2005; 90: 4955‑4962. | Crossref
- Hayes AR, Grossman AB. Distinguishing Cushing’s disease from the ectopic ACTH syndrome: needles in a haystack or hiding in plain sight? J Neuroendocrinol. 2022; 34: e13137. | Crossref
- Minasyan M, Bryk‑Wiązania AH, Rzepka E, et al. Saddle pulmonary embolism as a fatal complication of Cushing syndrome: a call for standardized anticoagulation regimen in hypercortisolism. Pol Arch Intern Med. 2023; 133: 16382. | Crossref
- Fleseriu M, Biller BMK. Treatment of Cushing syndrome with osilodrostat: practical applications of recent studies with case examples. Pituitary. 2022; 25: 795‑809. | Crossref
ARTICLE INFORMATION