When standard cardiac diagnostics fail: the key role of the Apple Watch in confirming the diagnosis of pacemaker ventricular lead damage



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
When standard cardiac diagnostics fail: the key role of the Apple Watch in confirming the diagnosis of pacemaker ventricular lead damage
A 63‑year‑old woman was admitted to the cardiology department due to a suspected malfunction of the right ventricular (RV) lead of a dual‑chamber pacemaker, which had been implanted 10 years ago for a paroxysmal Mobitz type 2 second‑degree atrioventricular block. Over the past several months, the patient has been experiencing gradually increasing weakness and dizziness. No features of pacemaker malfunction were found during the scheduled follow‑ups. The patient was also admitted to the emergency department following an episode of syncope while sitting. A follow‑up examination of the pacemaker again revealed no abnormalities. Electrocardiography (ECG) showed a sinus rhythm with a proper VAT mode of pacing (Figure 1A). Transthoracic echocardiography ruled out RV lead perforation (Figure 1B). Chest X‑ray confirmed no signs of mechanical damage (Figure 1C). The patient was discharged, as no evident cardiologic cause of her symptoms was found. A few days later, she returned to the emergency department after another episode of syncope. At that time, she was wearing an Apple Watch Series 6 (purchased as part of the syncope diagnostics), which allowed her to perform a single‑lead ECG. The recording made immediately before the syncopal episode showed ineffective ventricular pacing without an escape rhythm (Figure 1D). The patient was urgently admitted to the cardiology department.
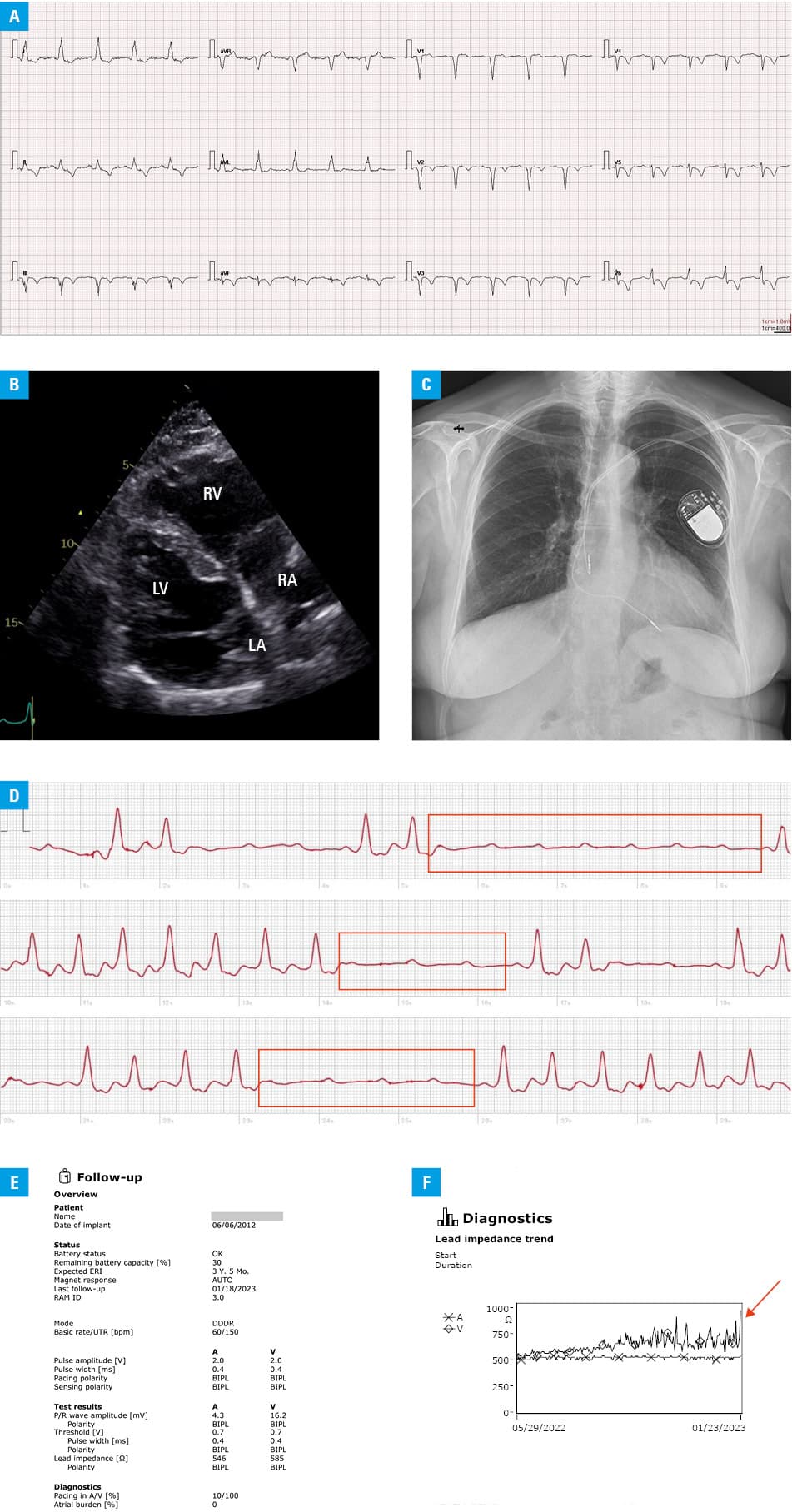
Abbreviations: LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle
An examination of the pacemaker confirmed that the lead impedance, pacing thresholds, and sensing values were again within normal ranges; however, a noticeable increase in RV lead impedance, with spikes up to approximately 1000 ohms (Figure 1E and 1F) was also documented. No sensing or pacing disturbances were found during the provocative maneuvers. The patient had a ventricular pacing rate of 100% due to pacemaker dependency. Finally, transvenous extraction of the damaged ventricular lead and simultaneous implantation of a new one were performed. During the 5‑month follow‑up, the patient did not complain of the previously reported symptoms.
To the best of our knowledge, the presented case is the first one to report the use of the Apple Watch to diagnose pacemaker lead dysfunction. The role of mobile health (mHealth) devices, including the Apple Watch with an ECG recording function, in diagnosing arrhythmias is well documented.1,2 mHealth solutions enable recognition of atrial fibrillation as well as other paroxysmal arrhythmias, which are often difficult to capture with regular ECG Holter monitoring.3 The European Society of Cardiology has even underlined the diagnostic value of mHealth solutions in the recent guidelines on atrial fibrillation.4 Our case demonstrates the potential usefulness of mHealth solutions for patients with cardiac implantable electronic devices (CIEDs). A telemonitoring program allowing for remote CIED checking, such as the one initiated recently,5 seems to be an ideal solution, particularly for pacemaker‑dependent patients. However, due to related financial restrictions in many countries, mHealth solutions could provide an interesting alternative. It is worth stressing that each recording made by an mHealth device has to be verified by a qualified physician. However, based on the growing popularity of such devices among patients, they could serve as a valuable complement to standard clinical diagnosis.
- Sana F, Isselbacher EM, Singh JP, et al. Wearable devices for ambulatory cardiac monitoring: JACC state‑of‑the‑art review. J Am Coll Cardiol. 2020; 75: 1582‑1592. | Crossref
- Chow CK, Ariyarathna N, Islam SM, et al. mHealth in cardiovascular health care. Heart Lung Circ. 2016; 25: 802‑807. | Crossref
- Hawryszko M, Sławiński G, Kozłowski D, Lewicka E. Apple Watch‑guided diagnosis of AVNRT in a pregnant woman – a case report and literature review. Front Cardiovasc Med. 2022; 9: 985421. | Crossref
- Hindricks G, Potpara T, Dagres N, et al; ESC Scientific Document Group. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio‑Thoracic Surgery (EACTS): the Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021; 42: 373‑498. | Crossref
- Kempa M, Sławiński G, Zieleniewicz P, et al. Implementation of remote monitoring in patients implanted with T‑ICD and S‑ICD involved in a recall campaign: an excellent tool with insufficient availability. Kardiol Pol. 2023; 81: 612‑615. | Crossref
ARTICLE INFORMATION