18F-FDG-PET/CT imaging of aseptic abscess syndrome mimicking metastatic disease or granulomatosis



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
18F-FDG-PET/CT imaging of aseptic abscess syndrome mimicking metastatic disease or granulomatosis
Aseptic abscess syndrome (AAS) is a rare autoinflammatory disorder of unknown etiology. Patients typically present with fever, abdominal pain, and high neutrophil counts. There is no identifiable pathogen, and antibiotics are ineffective.1 Differential diagnosis must be performed to rule out infection, inflammation, or malignancy. Immunomodulatory therapies have shown promising results in managing the condition and confirming the diagnosis, although the approach entails some risks, particularly in the cases with suspected infectious abscesses.2
We present a case of a 60‑year‑old man who reported to the emergency department with headache, dyspnea, cervical lymphadenopathy, bicytopenia, and febrile cough. His main relevant antecedent condition was tuberculosis 36 years ago. Computed tomography (CT) scan showed lumbo‑aortic lymph nodes and scars from previous pulmonary tuberculosis. No active deep infectious sites were identified. The main hypotheses included lymph node tuberculosis, lymphoma, or another infection. Microbial culture and histopathologic analysis revealed no causative organisms.
An initial 18F‑fluorodeoxyglucose positron emission tomography / CT (18F‑FDG‑PET/CT) was performed for suspicion of active tuberculosis or lymphoma, and to guide a biopsy. It showed high FDG uptake in supra- and infradiaphragmatic lymph nodes, pulmonary consolidations, and throughout the spleen (Figure 1A). Antibiotics were ineffective and the patient condition did not improve. A second 18F‑FDG‑PET/CT scan (Figure 1B) was performed 2 months after the initiation of antibiotics, and it showed metabolic progression with new FDG uptake in multiple lymph nodes, skin, muscles, peripancreatic infiltrates, and pulmonary consolidations. A small pericardial effusion appeared with low FDG uptake.
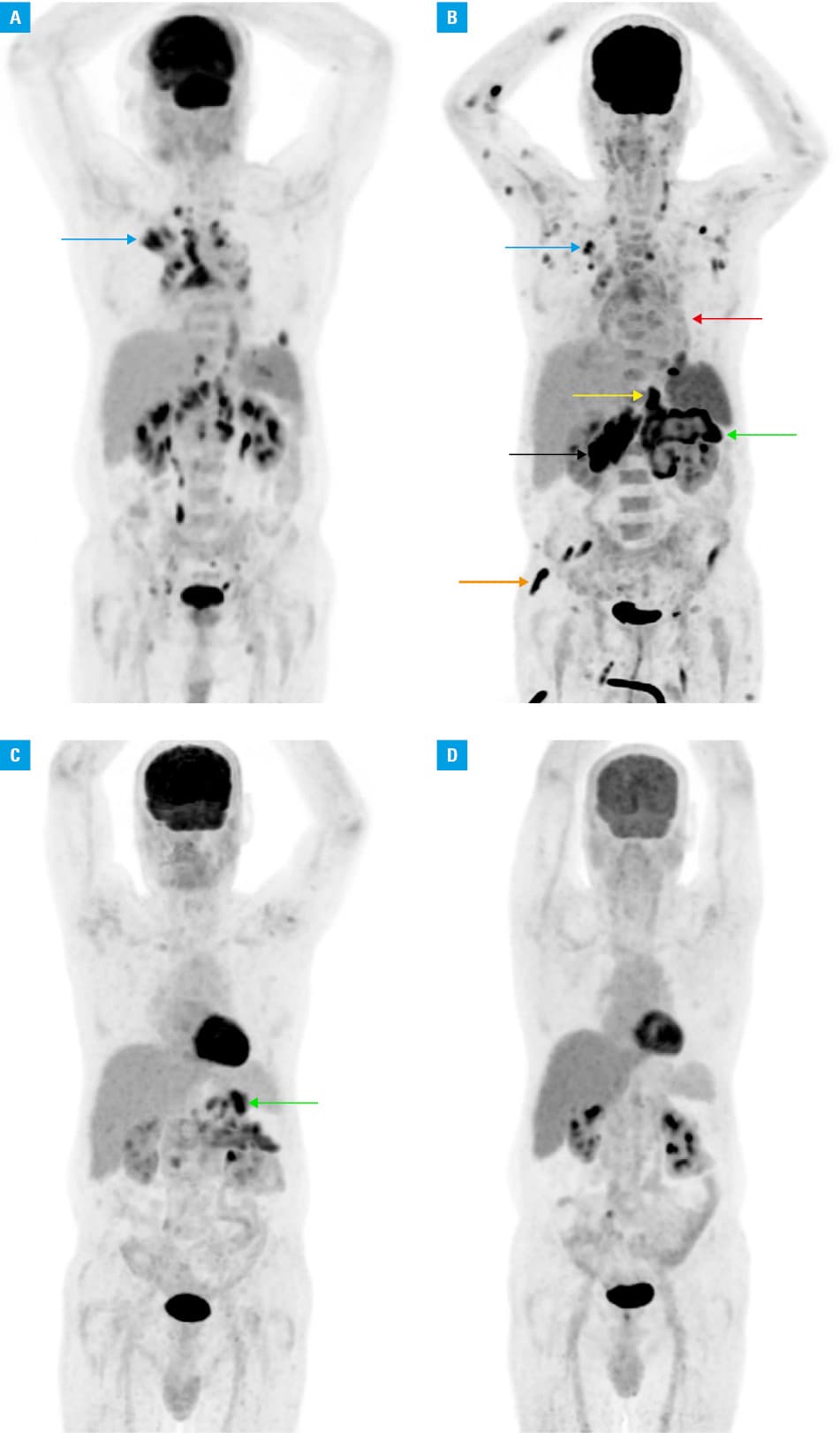
After 4 months of escalating symptoms, the antibiotic therapy was found inefficient, and the theory of bacterial infection was abandoned. AAS was considered, given the lack of clinical improvement and the absence of the culprit organism despite extensive testing. Colchicine was then started at 1 mg/day for 2 months. The patient experienced rapid clinical improvement from the first days of treatment. Another 18F‑FDG‑PET/CT scan (Figure 1C) performed 2 months after the initiation of colchicine showed a dissociated response, with intense FDG uptake around the pancreatic tail, a partial metabolic response in subdiaphragmatic lesions, and a complete metabolic response in supradiaphragmatic lesions.
Following the encouraging response to colchicine, the treatment was switched to prednisolone at a dose of 1 mg/kg/day, gradually tapered. The final 18F‑FDG‑PET/CT scan performed 2 months after the start of the steroid therapy showed a complete resolution of all lesions (Figure 1D). The treatment was discontinued, and the patient remained relapse‑free during 2 years of follow‑up.
In conclusion, AAS continues to challenge the medical community due to its diagnostic complexity and lack of known etiology. The diagnosis is still that of exclusion.3 Using advanced imaging modalities, such as 18F‑FDG‑PET/CT, clinicians can better understand the disease process and tailor appropriate therapeutic approaches to improve the patient outcome.4 Further research is warranted to unravel the underlying mechanisms of this challenging disease. The case presented here highlights the utility of 18F‑FDG‑PET/CT in the diagnosis and management of the disease, allowing for the assessment of the disease extent, treatment response, and detection of recurrence.
- André M, Piette JC, Kémény JL, et al. Aseptic abscesses: a study of 30 patients with or without inflammatory bowel disease and review of the literature. Medicine (Baltimore). 2007; 86: 145‑161. | Crossref
- Trefond L, Frances C, Costedoat‑Chalumeau N, et al. Aseptic abscess syndrome: clinical characteristics, associated diseases, and up to 30 years’ evolution data on a 71‑patient series. J Clin Med. 2022; 11: 3669. | Crossref
- André M, Aumaître O. Aseptic abscesses syndrome. Rev Med Interne. 2011; 32: 678‑688. | Crossref
- Guettrot‑Imbert G, Haroche J, Grimon G, et al. F‑18 FDG‑PET/CT in aseptic abscesses with recurrent febrile abdominal pain. Scand J Gastroenterol. 2011; 46: 577‑582. | Crossref
ARTICLE INFORMATION