May–Thurner syndrome as the cause of recurrent venous thromboembolism in a young woman: the role of multidisciplinary treatment



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
May–Thurner syndrome as the cause of recurrent venous thromboembolism in a young woman: the role of multidisciplinary treatment
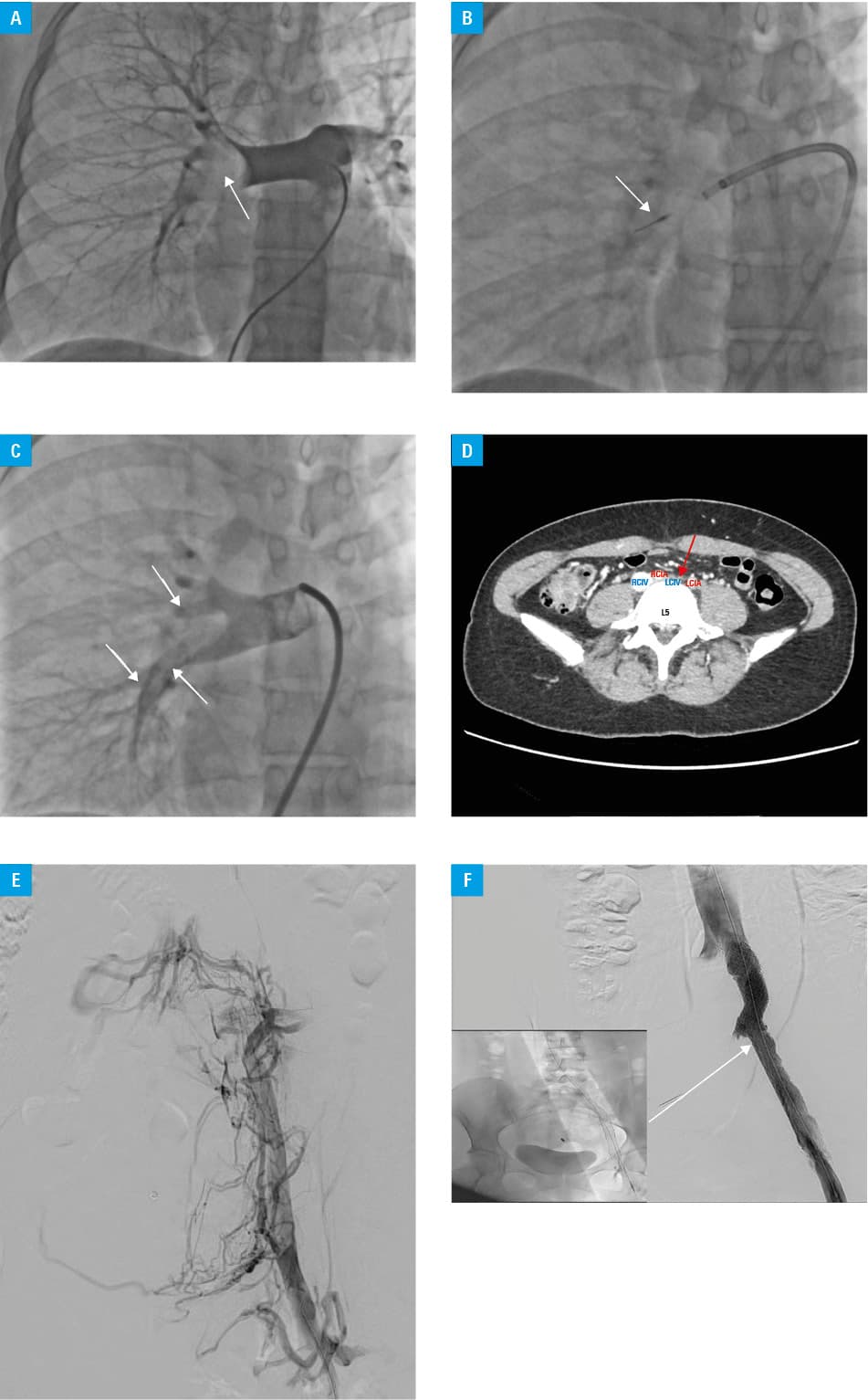
A 25‑year‑old woman was admitted due to an intermediate‑high‑risk pulmonary embolism (PE). Duplex ultrasound excluded the presence of deep vein thrombosis. Medical history of the patient included polycystic ovary syndrome and oral contraceptive use for the last 2 years. The initial therapy with low‑molecular‑weight heparin (LMWH) in a weight‑adjusted dose was ineffective, and after 48 hours the symptoms worsened (tachycardia up to 110 bpm and increased oxygen demand, without overt hypotension), with progression of right ventricular (RV) dysfunction (RV/left ventricular [LV] ratio increased from 0.9 to 1.1), and troponin increase from 0.5 to 1.1 ng/ml (reference value, <0.05 ng/ml). The institutional PE response team (PERT) qualified the patient for urgent catheter‑directed mechanical aspiration thrombectomy (CDMT).1,2 The procedure was performed with the 8F Indigo system (Penumbra, Alameda, California, United States) in the right and left pulmonary artery branches, and resulted in remarkable thrombus burden reduction and significant hemodynamic improvement (Figure 1A–1C). Testing for inherited and acquired coagulopathy was negative. The patient was discharged home 3 days later, on anticoagulation with rivaroxaban and a strong recommendation to avoid pregnancy for at least 6 months after the PE episode. She remained under the care of our outpatient clinic.
On the first 3‑month follow‑up visit the patient informed us about her pregnancy (5 weeks of gestation), and rivaroxaban was immediately switched to LMWH. Follow‑up visits with echocardiographic assessment were scheduled every month. The pregnancy course was uneventful, and ended with a normal vaginal delivery (at 38 weeks of gestation). Three months later, at an explicit request of the patient, anticoagulation with LMWH was stopped.
After the next 3 months, the patient presented to the emergency department with fatigue and left lower extremity pain with swelling for a few days. Duplex ultrasound demonstrated extensive left iliac vein thrombosis. Computed tomography (CT) phlebography showed that the thrombus filled the external, internal, and left common iliac vein (LCIV) with the external compression of the LCIV by the right common iliac artery (RCIA) (Figure 1D). May–Thurner syndrome (MTS) was diagnosed. CT angiography ruled out the recurrence of PE. The patient was qualified for endovascular treatment. CDMT was successfully performed in the left common and external iliac veins with the 10F Aspirex TM thrombectomy catheter (BD, Franklin Lakes, New Jersey, United States), with subsequent placement of 2 Zilver Vena stents (Cook, Bloomington, Indiana, United States) under the intravascular ultrasound guidance, without complications (Figure 1E and 1F). Anticoagulation with warfarin and antiplatelet therapy with clopidogrel (75 mg daily) for 12 months were recommended. The patient was discharged home 2 days later in a good condition. The 1‑year follow‑up was uneventful.
MTS is a clinical condition resulting from compression of LCIV between the overlying RCIA and the 5th lumbar vertebra.3,4 MTS has been implicated as the underlying etiology in 2%–5% of patients evaluated for symptomatic lower extremity venous disorder, and up to 20% of patients diagnosed with extensive left‑sided thromboembolism, especially recurrent.4,5 Herein, we report a case of MTS complicated by PE and iliac vein thrombosis successfully managed through multidisciplinary endovascular treatment.
- Kopeć G, Araszkiewicz A, Kurzyna M, et al. Role of catheter‑directed therapies in the treatment of acute pulmonary embolism. Expert opinion of the Polish PERT Initiative, Working Group on Pulmonary Circulation, Association of Cardiovascular Interventions, and Association of Intensive Cardiac Care of the Polish Cardiac Society. Kardiol Pol. 2023; 81: 423‑440. | Crossref
- Araszkiewicz A, Kurzyna M, Kopeć G, et al. Pulmonary embolism response team: a multidisciplinary approach to pulmonary embolism treatment. Polish PERT Initiative Report. Kardiol Pol. 2021; 79: 1311‑1319. | Crossref
- Kakkos SK, Gohel M, Baekgaard N, et al. Editor’s Choice ‑ European Society for Vascular Surgery (ESVS) 2021 Clinical Practice Guidelines on the Management of Venous Thrombosis. Eur J Vasc Endovasc Surg. 2021; 61: 9‑82.
- Poyyamoli S, Mehta P, Cherian M, et al. May‑Thurner syndrome. Cardiovasc Diagn Ther. 2021; 11: 1104‑1111. | Crossref
- Sławek‑Szmyt S, Stępniewski J, Kurzyna M, et al. Catheter‑directed mechanical aspiration thrombectomy in a real‑world pulmonary embolism population ‑ a multicenter registry. Eur Heart J Acute Cardiovasc Care. 2023; 12: 584‑593. | Crossref
ARTICLE INFORMATION