A rare case of continuous upper gastrointestinal hemorrhage with chronic pancreatitis



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
A rare case of continuous upper gastrointestinal hemorrhage with chronic pancreatitis
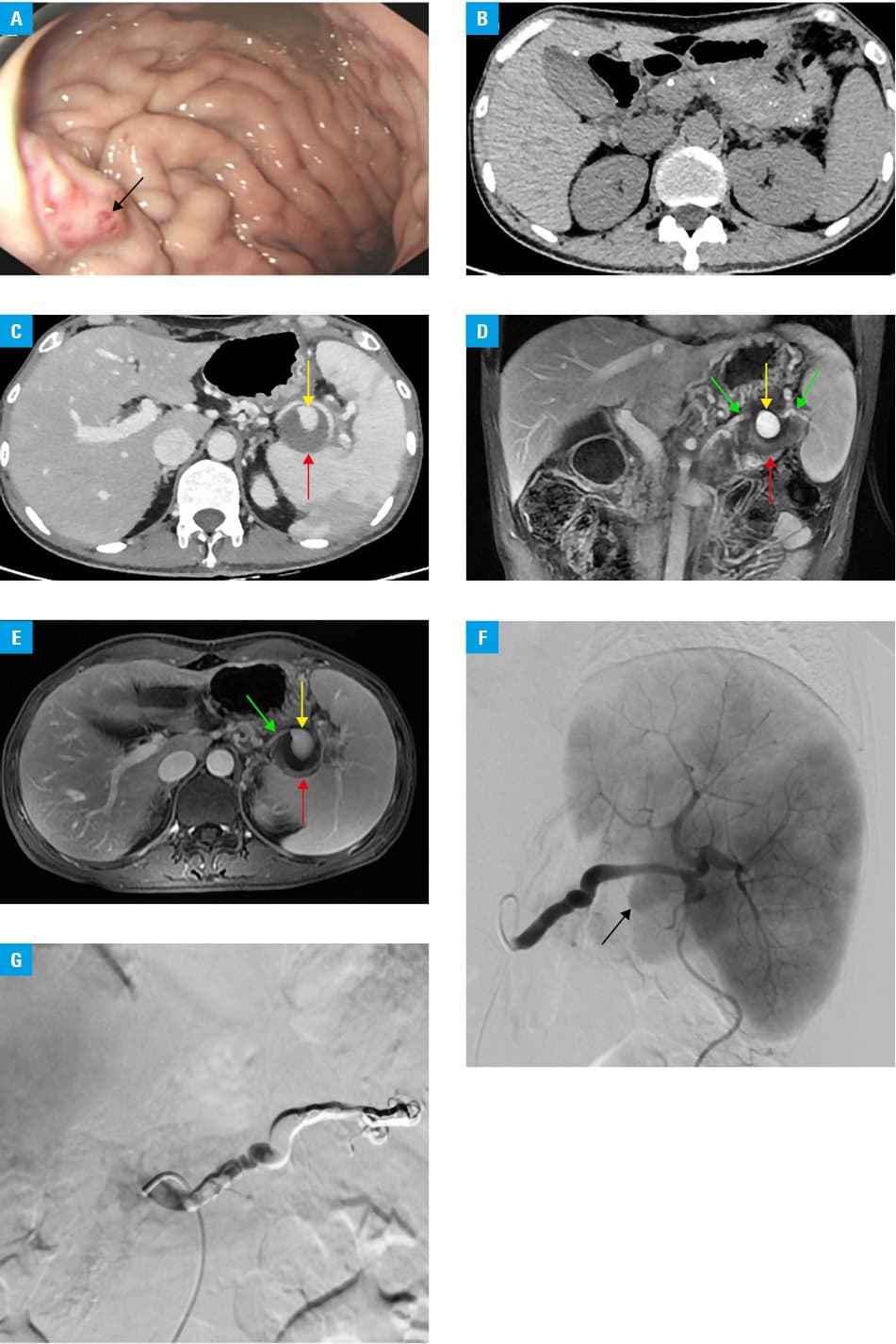
A 37‑year‑old man with a history of frequent episodes of acute pancreatitis over a period of 10 years was admitted to our hospital due to progressively worsening abdominal pain, melena, and dizziness for 10 days. An abdominal mass (about 2 cm in diameter) with a relatively tough texture presented in the left upper abdomen on physical examination. The fecal occult blood test showed strongly positive results, and gastroscopy found gastric varices in the greater curvature of the stomach with a red‑color sign (Figure 1A). Computed tomography (CT) revealed a normal liver and an atrophic pancreas with multiple calculi (Figure 1B). The patient was initially managed conservatively, including fasting, fluid resuscitation, proton pump inhibitors, somatostatin, and hemostatic agents. Follow‑up gastroscopy was performed, and the red‑color sign had disappeared. However, melena and abdominal pain were progressively worsening, and laboratory workup revealed a decreased level of hemoglobin at 76 g/l (reference range [RR], 115–150 g/l), elevated serum amylase at 236 U/l (RR, 35–135 U/l), and elevated D‑dimer at 2.37 mg/l (RR, 0–0.55 mg/l). Then, a follow‑up contrast‑enhanced CT scan showed a nonenhanced pancreatic pseudocyst (PPC) (largest diameter, 39 mm; Figure 1C) in the tail of the pancreas, with an enhanced focal region (largest diameter, 22 mm; Figure 1C). In order to specify the enhanced focal region visible on the CT scan, contrast‑enhanced magnetic resonance imaging (MRI) was arranged, and it confirmed a pseudoaneurysm within the PPC (Figure 1D and 1E). The pseudoaneurysm communicated with the adjacent splenic artery, which suggested it might be a splenic artery pseudoaneurysm. Digital subtraction angiography (DSA) was performed, and the contrast extravasated from the splenic artery during the procedure (Figure 1F), which confirmed the diagnosis of chronic pancreatitis (CP) complicated by PPC, splenic artery pseudoaneurysm, and pancreatic portal hypertension (PPH). A coil and liquid glue were used to embolize the splenic artery and stop bleeding (Figure 1G). Melena and dizziness symptoms improved after the interventional therapy and other medical treatments (proton pump inhibitors, somatostatin, and hemostatic agents). The patient was referred to the General Surgical Department for splenectomy.
PPH should be suspected in CP patients with upper gastrointestinal bleeding, especially in individuals with isolated gastric varices and normal hepatic functions. Early endoscopy is a gold standard for diagnosis, and splenectomy or interventional therapy, such as splenic artery embolization and splenic vein stenting are recommended treatments.1
In this case, PPH was not the actual etiology of continuous upper gastrointestinal bleeding. A high index of suspicion for pseudoaneurysm, a rare but life‑threatening condition, with a mortality rate of 23% even following treatment, is essential, especially in patients with PPC, and appropriate imaging examinations, such as CT or MRI are required. Laboratory tests also play an important role in the diagnosis of pseudoaneurysms, because elevated levels of serum amylase may imply an episode of acute pancreatitis, which would be the cause of PPC formation, and high D‑dimer concentrations may be a potential serological marker of pseudoaneurysms.2 Based on these imaging and laboratory tests, we suspected the possible relationship between CP and the formation of splenic artery pseudoaneurysm in our patient. Firstly, increased pressure in the pancreatic duct caused by pancreatic duct stones and / or stricture are closely related to the recurrent episodes of acute pancreatitis, releasing proteolytic fluid from the pancreas into the adjacent peritoneal cavity, and forming the PPC. Secondly, the splenic artery pseudoaneurysm developed after the enzymatic digestion, destruction, and erosion of the surrounding blood vessels within the PPC.3 Lastly, due to the communication between the PPC and the main pancreatic duct, secondary hemorrhage from the pseudoaneurysm contributed to melena. DSA has been the gold standard of diagnosis for a long time, while open surgery is a conventional management, with either bypass or aneurysmectomy. In addition, embolization procedures with coils, gelatin sponge, or injection of thrombin‑collagen compounds could also be used.4 In this case, DSA was performed to arrest bleeding from the splenic artery, not only to treat PPH by resolving hypertension on the splenic side of the portal circulation, but also to deal with the rupture of the splenic artery pseudoaneurysm.
- Wei B, Zhang L, Tong H, et al. Retrospective comparison of clinical outcomes following splenic vein stenting and splenic arterial embolization in sinistral portal hypertension‑related gastrointestinal bleeding. AJR Am J Roentgenol. 2021; 216: 1579‑1587. | Crossref
- Hoke M, Koppensteiner R, Schillinger M, et al. D‑dimer testing in the diagnosis of transfemoral pseudoaneurysm after percutaneous transluminal procedures. J Vasc Surg. 2010; 52: 383‑387. | Crossref
- Hyare H, Desigan S, Nicholl H, et al. Multi‑section CT angiography compared with digital subtraction angiography in diagnosing major arterial hemorrhage in inflammatory pancreatic disease. Eur J Radiol. 2006; 59: 295‑300. | Crossref
- Ho M, Chan Y, Cheng S. Successful endovascular management of giant splenic artery aneurysms. Vascular. 2013; 21: 317‑322. | Crossref
ARTICLE INFORMATION