Metastatic colon cancer in an elderly woman manifesting as hypopituitarism and vision loss



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Metastatic colon cancer in an elderly woman manifesting as hypopituitarism and vision loss
The pituitary gland represents an uncommon site for malignant tumors and metastatic lesions. Among metastatic tumors, breast and lung cancers account for more than 50% of cases, with colon carcinoma contributing to 2%–3%. The presence of pituitary metastases significantly impacts the prognosis, and poses a risk to the patient well‑being, through the induction of hypopituitarism, notably in the context of secondary adrenal insufficiency. It is noteworthy that diabetes insipidus is a predominant clinical manifestation reflecting frequent posterior lobe affection.1-3
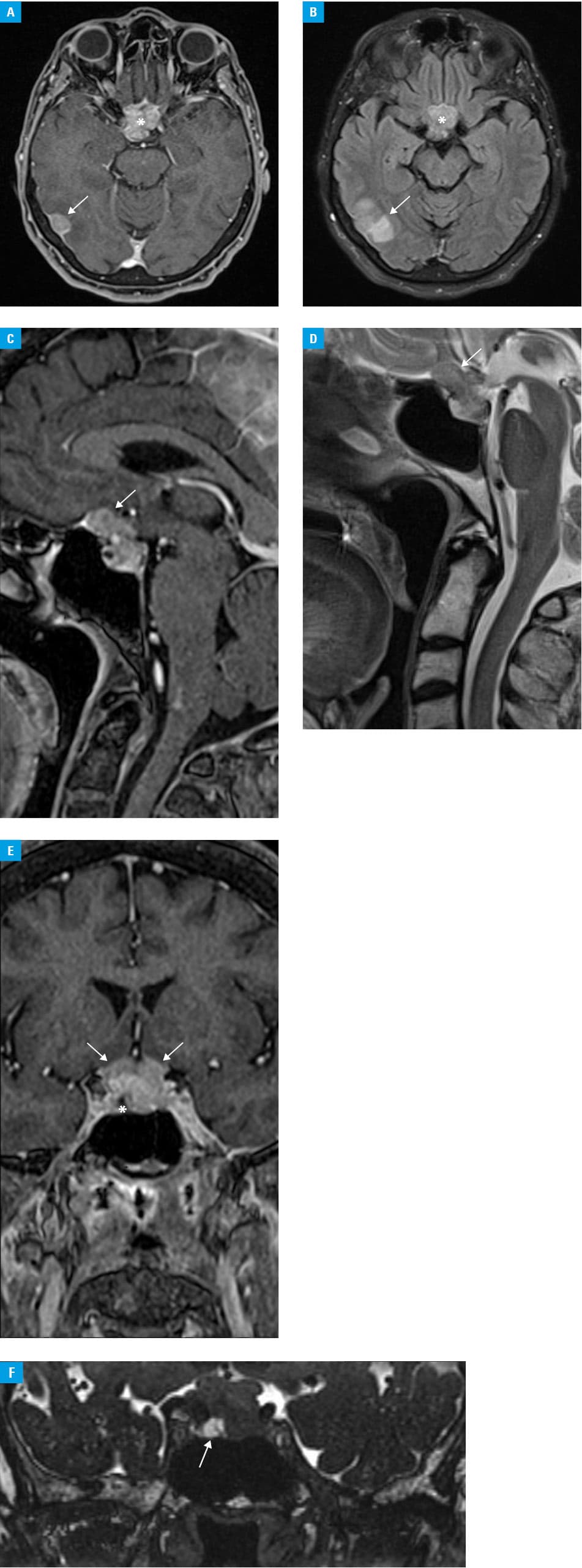
A 68‑year‑old woman was admitted to a hospital following a sudden right‑eye visual impairment. Her medical history included descending colon adenocarcinoma, which had been complicated by intestinal perforation and fecal peritonitis 7 months prior to the admission. This condition necessitated left hemicolectomy, with transverse colostomy and adjuvant chemotherapy treatment due to peritoneal and hepatic metastases. Upon admission, the patient reported weakness and nocturnal enuresis over the past 3 months. Physical examination revealed unilateral and painless vision loss, with the absence of other neurologic symptoms. After an ophthalmologic consultation, the patient underwent a magnetic resonance (MR) examination of the head. The MR scans revealed a polycyclic mass within the anterior cranial fossa, penetrating the sella turcica on the right side, extending into the right cavernous sinus, infiltrating the optic chiasm, and displacing the pituitary infundibulum (Figure 1A–1F). A suspicion of a metastatic lesion was raised because the morphologic characteristics of the tumor on the MR images were atypical for the most common pathologies. Laboratory investigations showed partial hormonal dysfunction of the pituitary gland, encompassing insufficiency in the gonadotropic and thyrotropic axis, alongside hyperprolactinemia. Dysfunction in the adrenocorticotropic axis could not be ruled out due to dexamethasone treatment, which was employed to mitigate edema and alleviate optic nerve compression. Due to the urgency of the case, a full diagnostic process to confirm diabetes insipidus (water deprivation test, desmopressin test) was abandoned after an endocrinologic consultation. Polyuria, low urine density, high serum osmolality, good response to desmopressin, and exclusion of other causes of nycturia confirmed the diagnosis of this disorder (Supplementary material, Table S1). Consequently, treatment with levothyroxine and desmopressin was initiated. Subsequently, the patient was qualified for transcranial tumor resection, employing the fronto‑sphenoidal approach. Postoperative histologic examination identified adenocarcinoma metastasis as the cause of the patient’s symptoms. Although a follow‑up MR examination confirmed decompression of the optic chiasm, the patient experienced binocular vision loss. It can be inferred that the vision loss and pituitary insufficiency were most likely secondary to the metastatic lesion, and were associated with the mass effect. The patient was referred for ongoing oncologic treatment and remains under the joint care of the ophthalmology and endocrinology outpatient clinics.
Screening tests, advanced diagnostic modalities, and enhanced therapeutic interventions have contributed to improved prognosis and prolonged survival rates among oncologic patients. Consequently, late neoplastic recurrences, after extended periods of remission, may affect uncommon organs, such as the pituitary gland. This underscores the importance of considering the pituitary gland as a potential site for metastasis, and highlights the need for clinical vigilance. Furthermore, the sudden onset of hypopituitarism in elderly individuals warrants inclusion of metastatic tumors in the differential diagnosis, particularly when the patients have a documented history of cancer.4,5
- Javanbakht A, D’Apuzzo M, Badie B, Salehian B. Pituitary metastasis: a rare condition. Endocr Connect. 2018; 7: 1049‑1057. | Crossref
- Kleinschmidt‑DeMasters BK. Metastases to the pituitary gland: histological patterns of spread and review of the literature. J Neuropathol Exp Neurol. 2021; 80: 1033‑1042. | Crossref
- Shimon I. Metastatic spread to the pituitary. Neuroendocrinology. 2020; 110: 805‑808. | Crossref
- Henry A, Nugent A, Wallace IR, et al. Pituitary metastasis: a clinical overview. Ulster Med J. 2021; 90: 146‑150.
- Castle‑Kirszbaum M, Goldschlager T, Ho B, et al. Twelve cases of pituitary metastasis: a case series and review of the literature. Pituitary. 2018; 21: 463‑473. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION