A case of legionnaires’ disease during the legionella epidemic in south-eastern Poland in August 2023

 CC BY 4.0
CC BY 4.0
A case of legionnaires’ disease during the legionella epidemic in south-eastern Poland in August 2023
In Poland, legionnaires’ disease has not been an epidemic threat to date. In 2019, 74 cases were recorded, in 2020 and 2021 as many as 46, while in 2022 there were 109 cases.1 By the end of August 2023, there have been 157 confirmed cases, 18 of which were fatal. Due to diagnostic difficulties, the above Figures are probably underestimated. However, the reported increase in morbidity rate should be considered a local epidemic.
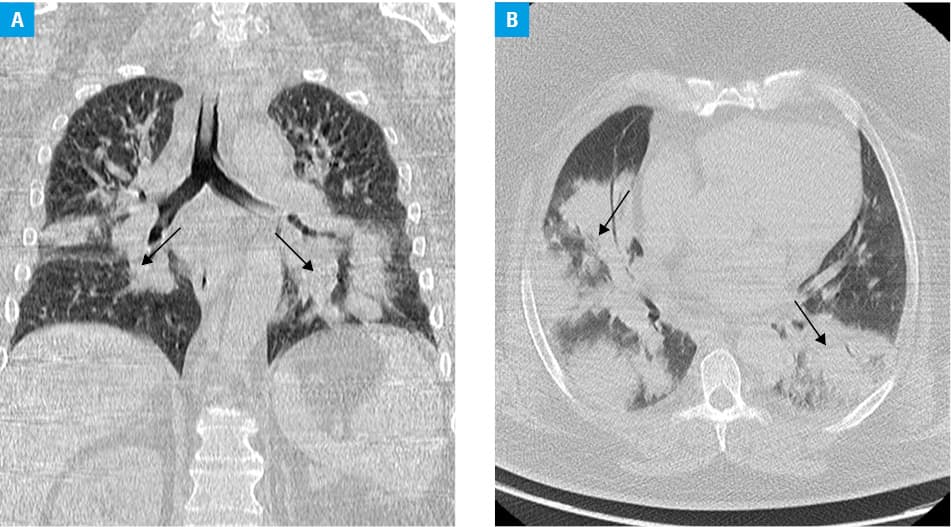
We report a case of pulmonary legionellosis. A 53‑year‑old patient with morbid obesity admitted to our hospital with progressive weakness, nonproductive cough, and fever up to 40 °C. The first symptoms appeared 5 days earlier. The initial diagnosis of bilateral massive pneumonia was based on a radiological image. Empirical antibiotic therapy was instituted (levofloxacin and ceftriaxone), passive oxygen therapy was applied via a Venturi mask with 50% O2. Despite the treatment and noninvasive ventilation, rapid deterioration of the patient’s condition was observed, and respiratory failure progressed. The patient was treated in the intensive care unit (ICU) from the first day of hospitalization. A computed tomography scan showed bilateral inflammatory lesions (Figure 1A and 1B). The patient was qualified for respiratory therapy. Blood, urine, and lower respiratory tract aspirate were immediately collected for microbiological testing. A Gram‑stained slide was prepared from the lower respiratory tract aspirate, and cultures were performed on standard microbiological media. No bacteria were found on the slide. The presence of Legionella pneumophila was detected in the aspirate by the multiplex polymerase chain reaction method. The presence of the pathogen was also confirmed by the recommended method2,3 of antigen detection in urine. Antibiotic therapy with levofloxacin was continued.2-4 From day 3 of the ICU stay, a significant decrease in inflammatory parameters and resolution of fever were observed. At the turn of days 7 and 8 of hospitalization in the ICU, a repeated but less severe increase in the inflammatory parameters was observed, and the fever rose up to 39 °C. Considering negative culture results, it was decided to extend the treatment targeting L. pneumophila. Antibiotic therapy was expanded to include clarithromycin.5 A satisfactory outcome was achieved, as assessed by a decrease in inflammatory parameters, resolution of fever, and improvement in ventilation parameters, including oxygen demand. On day 9 of hospitalization, rapid further deterioration of renal function was observed, accompanied by an increase in azotemia parameters, a decrease in diuresis below 0.25 ml/kg body weight/h, and brown coloring of urine. Creatine kinase level was determined, and it exceeded the upper limit of normal (reference range, 39–308 U/l) by 4.6 times on day 9 and by 13.68 times on day 10. Given the patient’s morbid obesity, poor general condition, and forced supine position, rhabdomyolysis was diagnosed. Despite intensive treatment, increasing signs of multiorgan damage were observed. Furthermore, symptoms of ileus appeared. The patient died on day 12 of ICU hospitalization and on day 17 from the onset of the first symptoms.
The case shows the stages of severe legionellosis leading to multiorgan damage.
- National Institute of Public Health ‑ National Institute of Hygiene, Department of Epidemiology and Surveillance of Infectious Diseases, Laboratory of Monitoring and Epidemiological Analysis [in Polish]. http://wwwold.pzh.gov.pl/oldpage/epimeld/2023/INF_23_08A.pdf. Accessed August 31, 2023.
- Hryniewicz W, Albrecht P, Radzikowska A. Recommendations for the management of non‑hospital respiratory infections [in Polish]. National Medicines Institute. 2016; 161‑181.
- Viasus D, Gaiga V, Manzur‑Barbur C, Carratala J. Legionnaires’ disease: update on diagnosis and treatment. Infect Dis Ther. 2022; 11: 973‑986. | Crossref
- Żukowska A, Hryniewicz W. Recommendations for diagnosis, therapy and antibiotic prophylaxis of hospital‑acquired infections ‑ 2020, material for therapeutic committees and antibiotic therapy teams [in Polish]. National Medicines Institute. 2020; 19‑20.
- Cruz C, Rodrigues L, Fernandes F, et al. Antibiotic susceptibility pattern of Portuguese environmental Legionella isolates. Front Cell Infect Microbiol. 2023; 13: 1141115. | Crossref
ARTICLE INFORMATION