The role of high-resolution computed tomography in diagnosing pneumonia caused by Legionella pneumophila



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
The role of high-resolution computed tomography in diagnosing pneumonia caused by Legionella pneumophila
Legionnaires’ disease, an important, well‑known, and relatively rare form of atypical community‑acquired pneumonia (CAP‑L), can be fatal if not treated early. The clinical picture of the disease is not significantly different from that of pneumonia caused by other bacteria, which makes the diagnosis challenging in clinical practice.1,2 Antibodies against Legionella pneumophila have been detected in the blood of patients with various conditions affecting the internal organs.3
We analyzed thoracic high‑resolution computed tomography (HRCT) scans of 10 out of 26 patients with endemic CAP‑L confirmed through urine testing for the L. pneumophila serotype 1 antigen (test sensitivity and specificity, 99%). The patients were admitted to the internal medicine department of a regional hospital in south‑eastern Poland between August 14 and August 31, 2023. The nationwide number of CAP‑L cases in 2020, 2021, and 2022 was 47, 46, and 118, respectively.4 Figure 1 shows chest HRCT images of 4 patients with CAP‑L, who are described in more detail below.
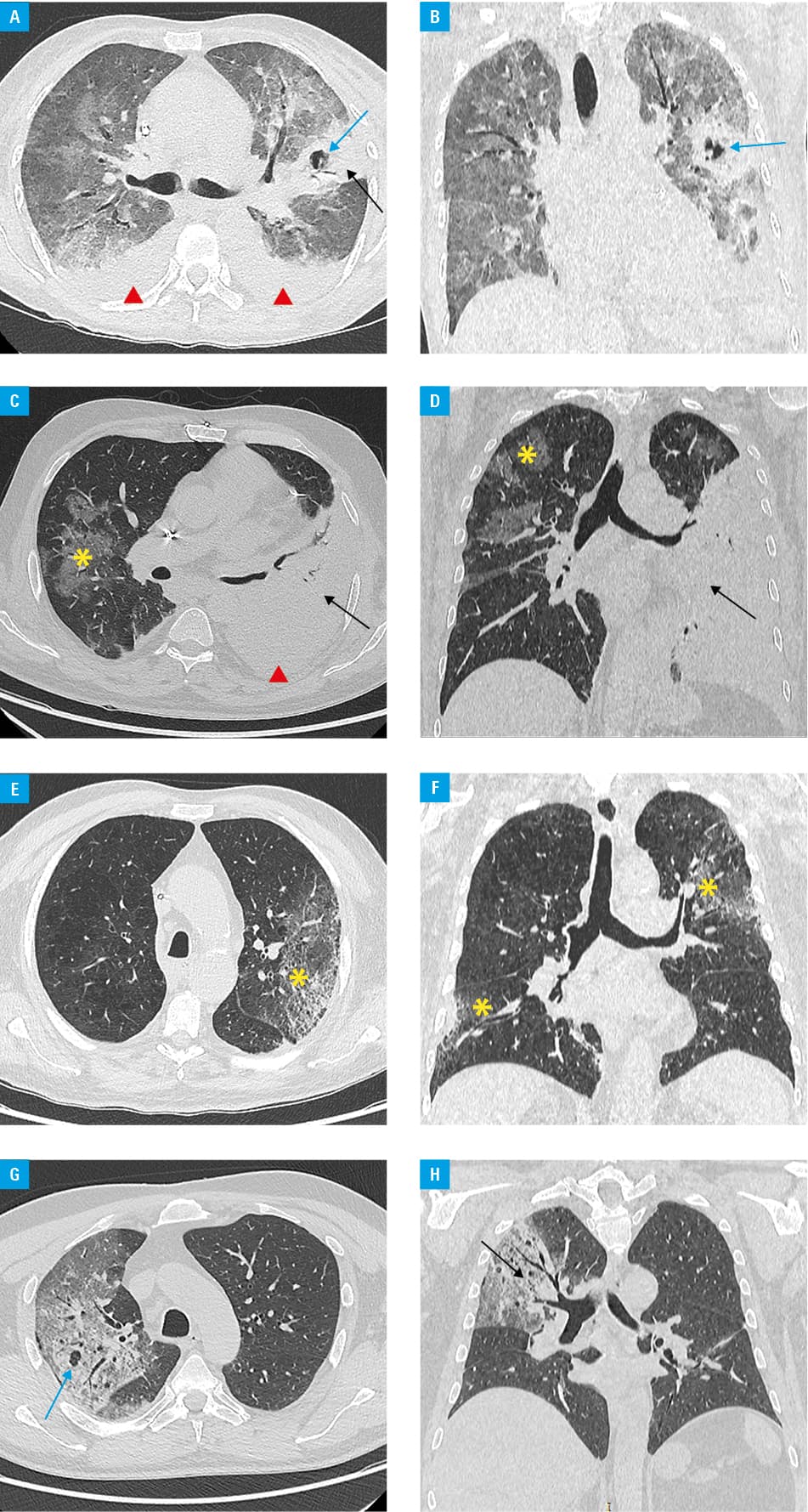
Patient 1 (Figure 1A and 1B) was a 51‑year‑old woman with antiphospholipid syndrome, acute renal failure in the course of lupus nephritis, and a history of cardiovascular events. She was urgently admitted to the hospital due to expectoration of bloody sputum, fever, and dyspnea with symptoms of respiratory failure. Patient 2 (Figure 1C and 1D) was an 86‑year‑old man with chronic heart failure due to chronic coronary syndrome, chronic kidney disease, and type 2 diabetes. He presented to the hospital with cough, shortness of breath, and dizziness. Patient 3 (Figure 1E and 1F) was a 54‑year‑old man with post–myocardial infarction heart failure, who was admitted to the internal medicine department in serious general condition, presenting with shortness of breath, dry cough accompanied by fever up to 39.5 °C, and diarrhea. Patient 4 (Figure 1G and 1H) was a 60‑year‑old man, chronically treated with glucocorticosteroids for cluster headaches. He was hospitalized due to persistent fever (up to 39 °C, for approximately 4–5 days), progressive weakness, resting dyspnea, and a dry, tiring cough. In laboratory workup, all patients had high levels of C‑reactive protein (range, 239.3–395.6 mg/l; reference range [RR] <10 mg/l), positive procalcitonin (range, 1.32–29.53 ng/ml; RR <0.5 ng/ml), and increased levels of alanine transaminase and aspartate aminotransferase (range, 51–164 U/l; RR <23 U/l and range, 44–618 U/l; RR <44 U/l, respectively). Hyponatremia, which was previously reported in CAP‑L, was observed in only 2 patients (sodium, 118–135 mmol/l; RR, 135–145 mmol/l).
On the lung HRCT images of our patients, we observed pulmonary parenchymal consolidations with air bronchograms typical of lobular pneumonia visible in the background (often bilateral), sometimes accompanied by pneumocele, ground‑glass densities, and pleural effusion, with no apparent lymphadenopathy. While the pulmonary lesions on HRCT images were consistent among all patients, they were not pathognomonic; thus, CAP‑L could not be diagnosed on this basis alone.
Therefore, it is important to closely monitor the epidemiology of CAP in clinical practice. In the event of increasing incidence of CAP in a region, especially during periods of high ambient temperatures, L. pneumophila infection should be considered in CAP differential diagnosis.
- Barimani MJ. Legionella: an uncommon cause of community‑acquired pneumonia. JAAPA. 2022; 35: 38‑42. | Crossref
- Kim KW, Goo JM, Lee HJ, et al. Chest computed tomographic findings and clinical features of legionella pneumonia. J Comput Assist Tomogr. 2007; 31: 950‑955. | Crossref
- Sikora A, Koszarny A, Kozioł-Montewka M, et al. The occurrence of antibodies against Legionella pneumophila in patients with autoimmune rheumatic diseases. Pol Arch Med Wewn. 2015; 125: 749‑754. | Crossref
- National Institute of Public Health ‑ National Institute of Hygiene. Registry of morbidity from infectious diseases, infections, and poisonings [in Polish]. https://wwwold.pzh.gov.pl/oldpage/epimeld/2022/Ch_2022. Accessed May 20, 2023.
ARTICLE INFORMATION