Heart failure (HF) is a major health problem worldwide due to its high prevalence, incidence, morbidity, and mortality. Moreover, since HF is a disease most prevalent among older individuals, a large number of patients with such a diagnosis in this age group poses a major strain on health care resources, due to not only the disease itself but also comorbidities and accompanying health impairments.1 In the last decade, newer pharmacological therapy options have improved the management and outcome of many HF patients.2 However, these elderly patients with HF often use other non‑HF–related therapies to control their symptoms or associated comorbidities, many of them of noncardiovascular etiology. A common practice among these patients is the use of benzodiazepines (BZDs) for the symptomatic treatment of HF‑related (or not) symptoms, such as dyspnea, anxiety, insomnia, and depression.3 The 2021 European Society of Cardiology guidelines for the diagnosis and treatment of acute and chronic HF suggest the use of BZDs for the relief of dyspnea, although not as the first‑line treatment,3 given little evidence available for this purpose.
BDZs enhance or facilitate the action of gamma‑aminobutyric acid, an inhibitory neurotransmitter in the central nervous system that suppresses the neural activity. This suppressive action at the limbic, thalamic, and hypothalamic level translates into a combination of anxiolytic, sedative, hypnotic, skeletal muscle relaxing, and anticonvulsant effects. Since these nonspecific symptoms are highly prevalent (and not only due to the presence of HF), BZDs are widely used on a chronic basis, although they are recommended for short‑term therapies due to a significant risk of side effects (dizziness, confusion, falls, etc.) associated with their prolonged use.4
Few studies have evaluated the effects of BDZ prescription in patients with HF,3,5,6 and therefore further research evaluating this common clinical scenario, such as the one by Ribeirinho‑Soares et al7 published in this issue of Polish Archives of Internal Medicine, is welcome. The authors evaluated 854 patients (69% men) with HF and reduced left ventricular ejection fraction, of a mean age of 71 years. Remarkably, 28% of these patients were receiving treatment with BDZs, mainly those with intermediate half‑life. After a follow‑up of almost 4 years, more than half of the patients died (51%). In a multivariate‑adjusted analysis, the use of BZDs was independently associated with increased death risk among these patients, with a hazard ratio of 1.36 (95% CI, 1.06–1.75). This serious side effect was more evident in the patients older than 75 years, and those with a concomitant diagnosis of chronic kidney disease (CKD).
The study has important strengths, such as the large number of patients, long follow‑up, and significant number of patients receiving treatment with BDZs. The authors also acknowledge some of its limitations, such as a retrospective and single‑center design, no data on the reason for BZD prescription, the chronology of BZD use, their pharmacologic properties (time to onset of action, half‑life, metabolism), and doses used. The results of this study are consistent with previous data that have also shown a negative interaction between the use of BZDs and an increased risk of long‑term mortality in patients with HF.6,8,9 However, most of these studies are retrospective in design and have important limitations, again related to specific data on the type of BZDs and dosing. Therefore, well‑designed, prospective studies with details on BZD prescription are needed. They should cover the reason for which BZDs are prescribed and the aforementioned pharmacologic characteristics of the prescribed drugs (dose, duration) should be recorded and investigated.
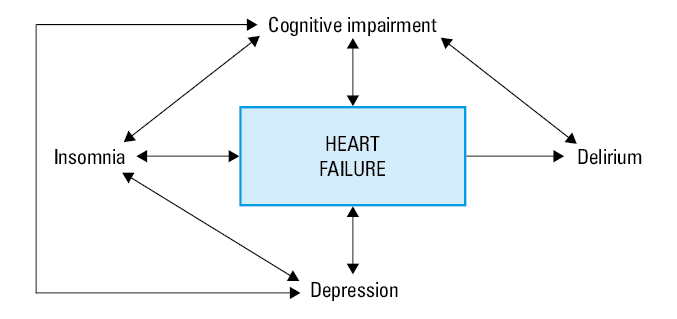
Also, it must be noted that, apart from comorbidities typically associated with HF (CKD, anemia, diabetes, etc.), other not commonly investigated conditions, such as insomnia, depression, or cognitive impairment may also worsen the prognosis of the disease.10-12 These clinical scenarios usually interact and present simultaneously in elderly HF patients, and often become evident during an episode of decompensation and resulting hospital admission, when a superimposed syndrome of delirium may also ensue (Figure 1). These are indeed clinical scenarios where the administration of BZDs may play a role, not only due to their use in symptomatic therapy, but also as a potential cause of clinical deterioration following their misuse. Another scenario may also include the BZD withdrawal syndrome, sometimes overlooked upon admission of an elderly patient with acute HF.
In conclusion, the negative aspects of BZD administration should remind us to evaluate and treat the elderly HF patients as whole human beings, and not to limit their evaluation only to HF‑related characteristics, such as the ejection fraction, congestion, or neurohormonal therapies, or only to the classic cardiovascular comorbidities, such as kidney dysfunction, electrolyte disturbances, or decreased hemoglobin levels. It is mandatory to incorporate the principles of comprehensive geriatric evaluation into our daily contacts with such patients, including a thorough review of all the prescribed drugs and the reasons for their use. It is likely that BZD use is not evidence‑based in many instances, especially when they are prescribed in a chronic fashion, since short‑term treatments with short‑acting BZDs are preferred in the guidelines.13 Future prospective studies are necessary to advance our knowledge of this relevant clinical problem.
- Jiménez‑Méndez C, Díez‑Villanueva P, Bonanad C, et al. Frailty and prognosis of older patients with chronic heart failure. Rev Esp Cardiol (Engl Ed). 2022; 75: 1011‑1019. | Crossref
- McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2022; 24: 4‑131. | Crossref
- Salamanca‑Bautista P, Romero‑Correa M, Formiga F, et al; EPICTER Investigators group. Safety of benzodiazepines in patients with acute heart failure: a propensity score‑matching study. Int J Cardiol. 2023; 382: 40‑45. | Crossref
- Capiau A, Huys L, van Poelgeest E, et al. Therapeutic dilemmas with benzodiazepines and Z‑drugs: insomnia and anxiety disorders versus increased fall risk: a clinical review. Eur Geriatr Med. 2022 Dec 28. [Epub ahead of print] | Crossref
- Diez‑Quevedo C, Lupon J, de Antonio M, et al. Benzodiazepine use and long‑term mortality in real‑life chronic heart failure outpatients: a cohort analysis. Psychother Psychosom. 2018; 87: 372‑374. | Crossref
ARTICLE INFORMATION