Collision sellar lesion: coexistence of growth hormone–secreting pituitary neuroendocrine tumor and pituicytoma

 CC BY 4.0
CC BY 4.0
Collision sellar lesion: coexistence of growth hormone–secreting pituitary neuroendocrine tumor and pituicytoma
In the sellar region, pituitary adenomas (pituitary neuroendocrine tumors [PitNETs]) are the most frequent lesions originating from the pituitary gland. Additionally, low‑grade tumors arising from the pituicytes of the posterior pituitary gland or infundibulum, including pituicytoma, can also be found in this region.1 The term “collision sellar lesion” is used to describe cases where a PitNET coexists with another pituitary or sellar lesion.2 The coexistence of pituicytoma within pituitary adenoma is a rare occurrence, with only 20 reported cases worldwide.2,3 Most commonly, PitNETs are found together with Rathke cleft cysts or craniopharyngiomas.4,5 Both PitNETs and pituicytomas have favorable oncologic prognosis in the long‑term follow‑up.
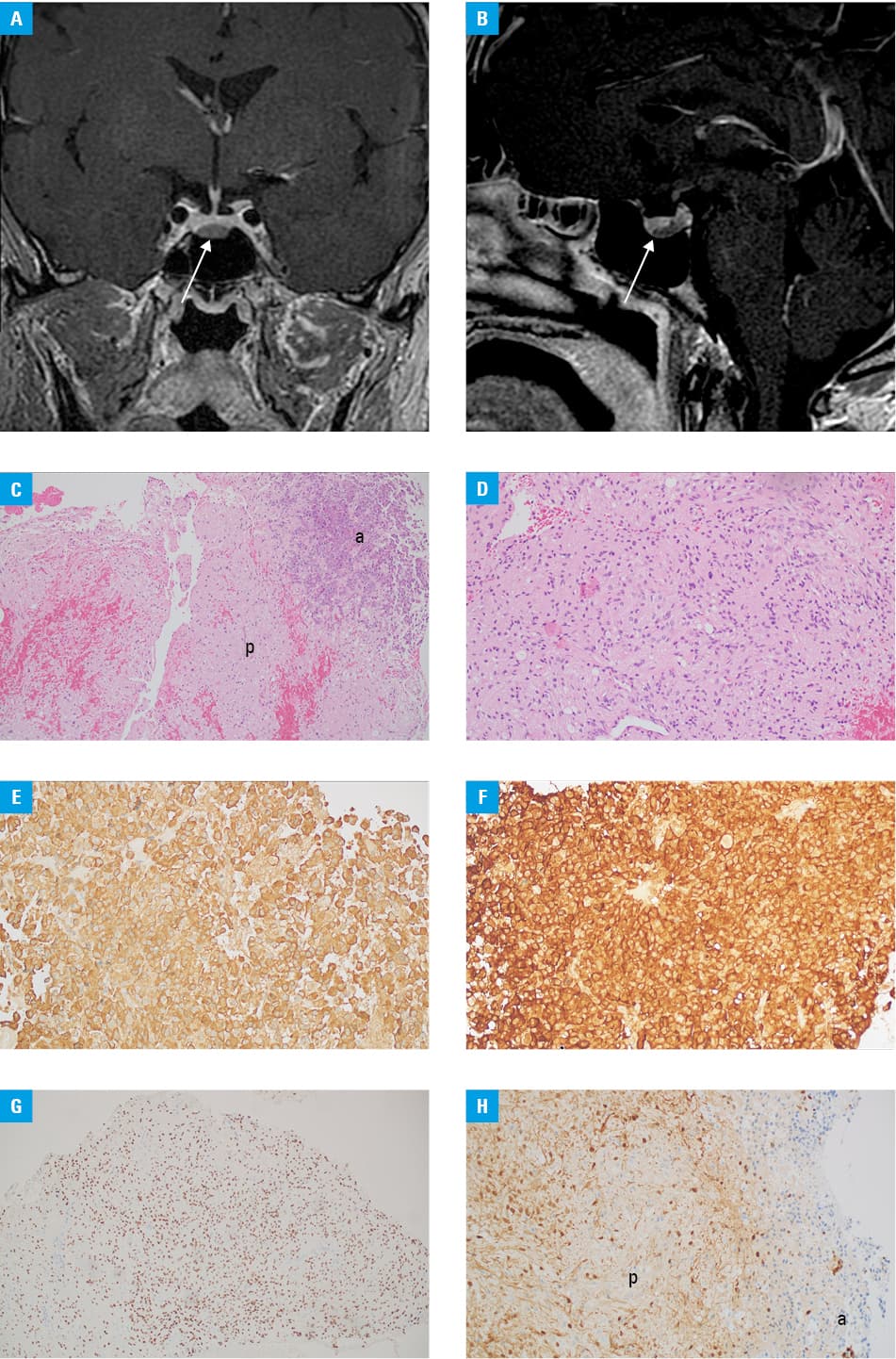
A 47‑year‑old man was initially diagnosed in the Department of Endocrinology due to clinical signs indicative of acromegaly. The suspicion of acromegaly arose from clinical observations that included digital hypertrophy, characterized by increased dimensions and thickness of the fingers and toes, as well as hypertrophy of nasal structures, prognathism, and concurrent symptoms of sleep apnea. The hormonal profile was normal except for the growth hormone (GH) levels, which were at the upper limit of the reference range (2.4 ng/ml; normal range, 0.03–2.47 ng/ml), with no GH suppression during the oral glucose tolerance test (until 1.99 ng/ml). Additionally, the patient exhibited elevated levels of insulin‑like growth factor 1 (487.4 ng/ml; reference range, 71–224 ng/ml). Notably, there were no signs of diabetes insipidus. Magnetic resonance imaging (MRI) revealed a normal‑size pituitary gland within the sella with a visible lesion with radiological features of microadenoma (3 mm × 7 mm × 9 mm) along the entire base of the pituitary (Figure 1A and 1B). Based on the hormonal profile and imaging findings, a diagnosis of acromegaly was established without any suggestion of a collision lesion.
The patient was scheduled for surgery, endoscopic transsphenoidal tumor removal. Intraoperatively, a mass lesion characteristic of pituitary adenoma was identified, clearly distinguishable by both color and structure from the normal pituitary gland. Postsurgery, there was a significant decrease in serum GH levels (0.3 ng/ml on postoperative day 3), along with development of postoperative diabetes insipidus requiring desmopressin treatment. Postoperative imaging revealed minimal surgery‑induced changes within the sella.
Histopathologic and immunohistochemical examination revealed the presence of 2 neoplastic components in the lesion: pituicytoma and PitNET with positive immunostaining for GH (Figure 1C–1H).
At 18‑month follow‑up, MRI confirmed the removal of the pathologic mass, and clinical and biochemical symptoms of acromegaly resolved. There were no signs of pituitary insufficiency, including diabetes insipidus, which allowed for withdrawal of desmopressin treatment.
In conclusion, rare posterior pituitary tumors and collision tumors should be considered in a differential diagnosis of MRI‑visible intrasellar lesions, even if the lesions do not involve the suprasellar space. According to the existing literature and the authors’ personal experience, distinguishing a collision sellar tumor preoperatively can be challenging, as these lesions often present as a single tumor on imaging. For symptomatic lesions, surgical intervention is recommended.
- Salge‑Arrieta FJ, Carrasco‑Moro R, Rodriguez‑Berrocal V, et al. Clinical features, diagnosis and therapy of pituicytoma: an update. J Endocrinol Invest. 2019; 42: 371‑384. | Crossref
- Marco Del Pont F, Villalonga JF, Ries‑Centeno T, et al. Pituicytoma associated with acromegaly and Cushing disease. World Neurosurg. 2020; 136: 78‑82. | Crossref
- Xiao T, Duan L, Chen S, et al. Pituicytoma associated with suspected Cushing’s disease: two case reports and a literature review. J Clin Med. 2022; 11: 4805. | Crossref
- Koutourousiou M, Kontogeorgos G, Wesseling P, et al. Collision sellar lesions: experience with eight cases and review of the literature. Pituitary. 2010; 13: 8‑17. | Crossref
- Matyja E, Maksymowicz M, Grajkowska W, et al. Ganglion cell tumours in the sella turcica in close morphological connection with pituitary adenomas. Folia Neuropathol. 2015; 53: 203‑218. | Crossref
ARTICLE INFORMATION