Peripartum cardiomyopathy requiring heart transplantation, complicated by disseminated aspergillosis and superior vena cava syndrome



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Peripartum cardiomyopathy requiring heart transplantation, complicated by disseminated aspergillosis and superior vena cava syndrome
Peripartum cardiomyopathy (PPCM) may occur in late pregnancy or in early postpartum in women without previous cardiac diseases.1 PPCM manifests as signs and symptoms of heart failure (HF) due to left ventricular (LV) dysfunction with ejection fraction (LVEF) below 45%.2 We present an unusual case of PPCM requiring heart transplantation (HTx), complicated by disseminated aspergillosis and superior vena cava syndrome (SVCS).
A 27‑year‑old woman presented to our intensive care unit 3 months after delivery with PPCM with LVEF of 20%, treated unsuccessfully with bromocriptine and medications for HF in a tertiary hospital. She had shortness of breath, blood pressure of 66/45 mm Hg on dopamine infusion started in the previous hospital, and oxygen saturation of 85% on passive oxygen therapy. After admission, noradrenaline, adrenaline, then levosimendan were administered, and venoarterial extracorporeal membrane oxygenation, mechanical ventilation, and continuous renal replacement therapy (CRRT) were provided due to cardiogenic shock and multiple organ dysfunction syndrome (MODS).
Transthoracic echocardiogram (TTE) demonstrated persistent global LV hypokinesia. Urgent HTx was performed on the 7th day of hospitalization, and immunosuppressants (tacrolimus, methylprednisolone, mycophenolate mofetil) were started. On control TTE, normal LVEF and ventricular volumes were observed. CRRT was continued until the 55th day of hospitalization, and then periodical dialyses were performed until the 79th day. Elective endomyocardial biopsies were performed 6 times without signs of the graft rejection.
On the following days bronchoscopy performed for suspected lung infection revealed the presence of aspergillosis and Stenotrophomonas maltophilia, and treatment with voriconazole (orally, 200 mg/day), amphotericin B (inhaled deoxycholate formulation, 50 mg/8 ml; intravenously in a liposomal form, 0.05 g/day), and ceftazidime (intravenously, 2 g, 3 times a day) was initiated. Control bronchoscopies showed regression of the pulmonary fungal lesions, however, thyroid ultrasound revealed a 1‑cm hypoechogenic lesion, possibly an abscess. Fine‑needle biopsy of the thyroid gland confirmed fungal infiltration. Despite intensive antifungal treatment, control imaging studies showed persistent lesions in the lungs (Figure 1A) and thyroid gland (Figure 1B), as well as new lesions in the heart (Figure 1C–1F) and central nervous system (CNS) (Figure 1G).
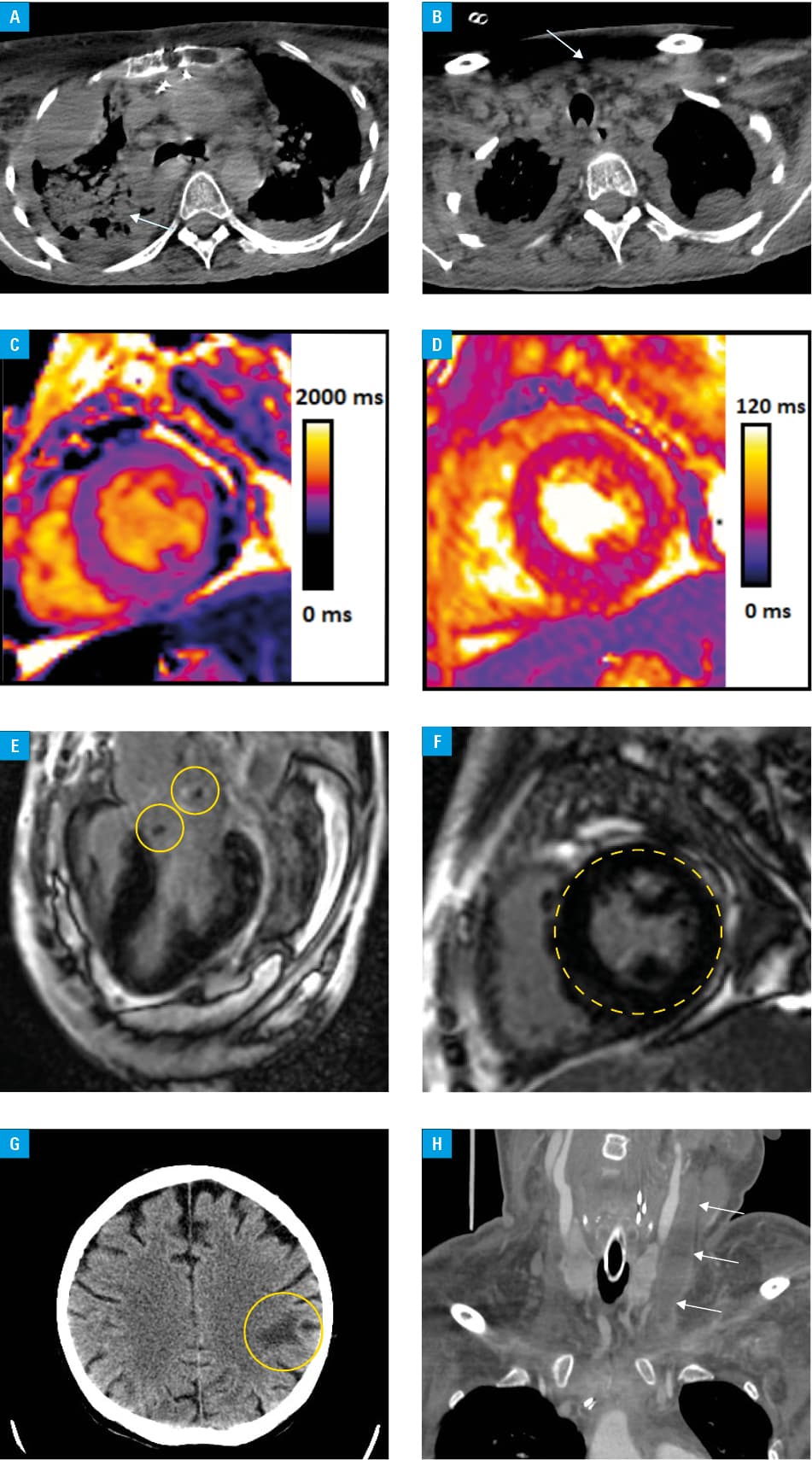
After a brief improvement, the patient’s condition suddenly worsened. Cytomegalovirus and Klebsiella pneumoniae infections were diagnosed and treated with valganciclovir (orally, 900 mg once or twice a day) and colistin (inhaled, 1 million IU, and intravenously, 3 million IU, each 3 times a day). Over the following days, the patient developed SVCS (Figure 1H) and dizziness. Venous thrombosis was treated conservatively with therapeutic doses of unfractionated heparin (with activated partial thromboplastin time controlled), and later with enoxaparin 60 mg/0.6 ml or 40 mg/0.4 ml every 12 hours. Partial thyroidectomy was performed. Progressive circulatory failure, acidosis, and increased lactate levels were observed despite intensive treatment, including administration of inotropic agents and CRRT. The patient died on the 151th day of hospitalization due to MODS and septic shock.
This case highlights a combination of rare presentations of PPCM requiring HTx complicated by disseminated aspergillosis, bacterial infections, and SVCS. PPCM shows a rapid onset and progression, and can be life‑threatening despite intensive and complex treatment.3 The current approach to managing PPCM involves standard treatment of HF with reduced LVEF with bromocriptine. The key is an early diagnosis to avoid advanced stages of HF that require mechanical support or HTx.4 The mortality rate in invasive aspergillosis in HTx recipients is high, exceeding 20% after 3 months and 38%–67% after 1 year, especially in disseminated cases with CNS involvement.5 This indicates the need for testing early infections and providing preventive antifungal medication in high‑risk patients.
- Sanusi M, Momin ES, Mannan V, et al. Using echocardiography and biomarkers to determine prognosis in peripartum cardiomyopathy: a systematic review. Cureus. 2022; 14: e26130. | Crossref
- Hosseinpour A, Hosseinpour H, Kheshti F, et al. Prognostic value of various markers in recovery from peripartum cardiomyopathy: a systematic review and meta‑analysis. ESC Heart Fail. 2022; 9: 3483‑3495. | Crossref
- Dinic V, Markovic D, Savic N, et al. Peripartum cardiomyopathy in intensive care unit: an update. Front Med (Lausanne). 2015; 2: 82. | Crossref
- Honigberg MC, Givertz MM. Peripartum cardiomyopathy. BMJ. 2019; 364: k5287. | Crossref
- Husain S, Camargoon JF. Invasive aspergillosis in solid‑organ transplant recipients: guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin Transplant. 2019; 33: e13544. | Crossref
ARTICLE INFORMATION