Extensive cardiac damage due to Streptococcus sanguinis infective endocarditis in a patient with complex congenital heart disease

 CC BY 4.0
CC BY 4.0
Extensive cardiac damage due to Streptococcus sanguinis infective endocarditis in a patient with complex congenital heart disease
The risk of infective endocarditis is higher in patients with adult congenital heart disease than in the general population, and it differs substantially depending on the type of lesions and clinical conditions.1-4
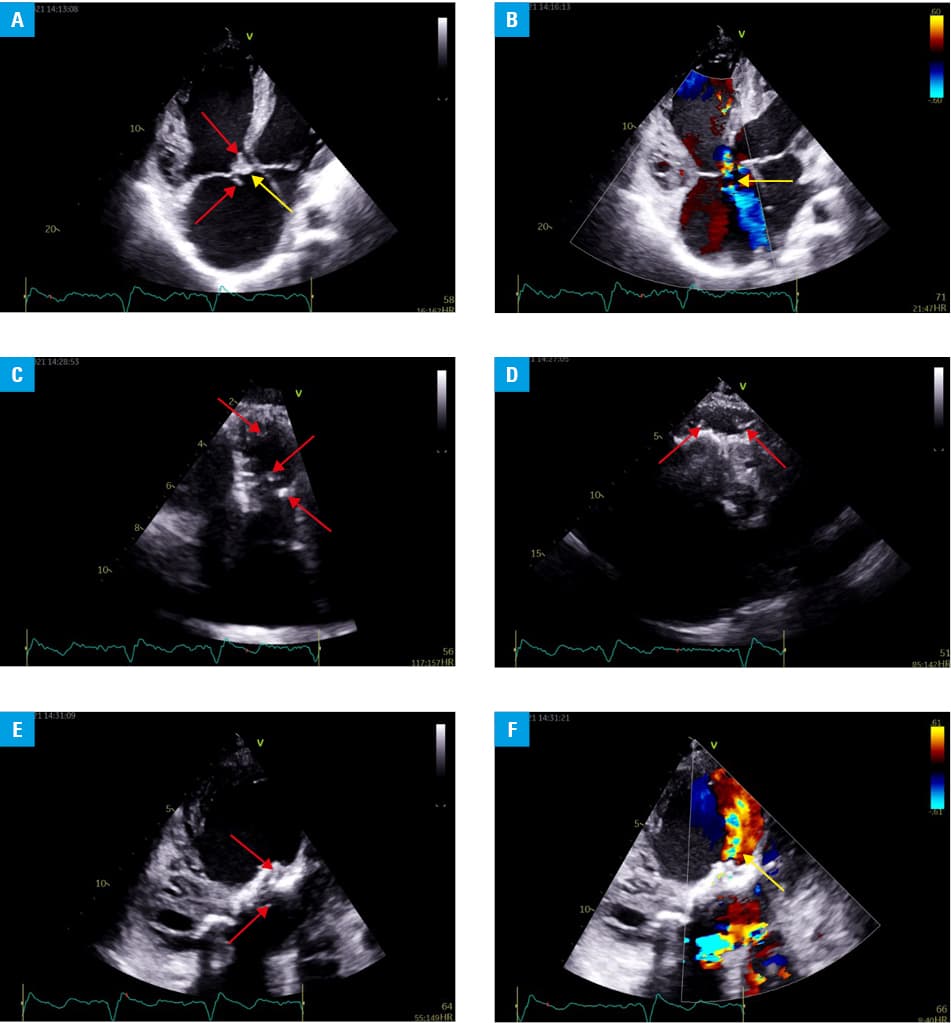
We present a case of a 34‑year‑old man with d‑transposition of the great arteries, ventricular septal defect, and valvular pulmonary stenosis after several surgical interventions: modified Blalock–Taussig shunt (1989); Rastelli procedure (1992); residual ventricular septal defect closure and septal tricuspid valve leaflet reconstruction due to significant ventricular left‑to‑right shunt and severe tricuspid regurgitation (1992); right ventricle to pulmonary artery conduit replacement, tricuspid septoanterior commissure valvuloplasty, and ascending aorta prosthesis implantation due to severe conduit regurgitation, severe tricuspid regurgitation, and ascending aorta aneurysm (2007). He had a history of staphylococcal infective endocarditis in 2008. The patient was admitted to our institution with heart failure exacerbation, New York Heart Association class III, cough and recurrent fever up to 38 °C, and chills for the last 9 months before the admission. He has been treated by a general practitioner with oral antibiotics. Laboratory tests performed on admission showed leukocytosis (12.4 × 103/µl; reference range [RR], 4.2–9.1 × 103/µl) and elevated C‑reactive protein (12 mg/dl; RR, <0.5 mg/dl) and procalcitonin (26 ng/ml; RR, <0.05 ng/ml) concentrations. Transthoracic echocardiography revealed severe systolic dysfunction of hypertrophied and enlarged right ventricle, thickened tricuspid valve leaflets with 2 vegetations attached to the anterior leaflet, and significant tricuspid regurgitation (Figure 1A and 1B). Besides, moderate stenosis and moderate regurgitation of the right ventricle to the pulmonary artery conduit with numerous vegetations in the right ventricular outflow tract were visible (Figure 1C and 1D). Moreover, residual ventricular septal defect with left‑to‑right shunt with one vegetation within the tunnel and another one connected to the patch inside the left ventricle (Figure 1E and 1F), and severe systolic dysfunction of the left ventricle could be observed. Parenteral antibiotic therapy including ampicillin and gentamicin was immediately implemented. Blood cultures were positive for Streptococcus sanguinis. A diagnosis of infective endocarditis was established based on the modified Duke criteria. Persistent chest pain and new onset of abdominal pain were the indications for a computed tomography scanning, which revealed systemic and pulmonary emboli located in the spleen and the right lung, respectively. Despite the patient’s deterioration, the Endocarditis Team decided not to refer him for surgery and to continue with the conservative treatment due to severe functional impairment of both ventricles and a history of several cardiothoracic interventions. Targeted antibiotic therapy did not, however, improve the patient’s condition. On the second week of medical therapy, he suddenly collapsed and required intensive cardiac care with mechanical ventilation, catecholamine infusion and, eventually, renal replacement therapy and endocardial ventricular pacing. After 12 days of septic shock management he demonstrated cardiac arrest not responding to cardiopulmonary resuscitation.
Infective endocarditis should be suspected in all patients with congenital heart disease presenting with fever and heart failure exacerbation. Not only physicians should be aware of this potentially fatal complication but patients as well. Advanced stage of the disease usually precludes effective pharmacologic treatment.
- Haas NA, Bach S, Vcasna R, et al. The risk of bacterial endocarditis after percutaneous and surgical biological pulmonary valve implantation. Int J Cardiol. 2018, 268: 55‑60. | Crossref
- Ostergaard L, Valeur N, Ihlemann N, et al. Incidence of infective endocarditis among patients considered at high risk. Eur Heart J. 2018; 39: 623‑629. | Crossref
- Kuijpers JM, Koolbergen DR, Groenink M, et al. Incidence, risk factors, and predictors of infective endocarditis in adult congenital heart disease: focus on the use of prosthetic material. Eur Heart J. 2017; 38: 2048‑2056. | Crossref
- Thornhill MH, Jones S, Prendergast B, et al. Quantifying infective endocarditis risk in patients with predisposing cardiac conditions. Eur Heart J. 2018; 39: 586‑595. | Crossref
ARTICLE INFORMATION