D-Dimers in diagnosis and prevention of venous thrombosis: recent advances and their practical implications
Key words: cancer, COVID-19, fibrin degradation product, pregnancy, venous thromboembolism



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
D-Dimers in diagnosis and prevention of venous thrombosis: recent advances and their practical implications
D‑Dimers derive from degradation of cross‑linked fibrin by plasmin, and thus their level is a marker of coagulation and fibrinolytic system activation. Guidelines recommend that D‑dimers are determined if the pretest probability (PTP) is low or intermediate, to exclude venous thromboembolism (VTE), either deep vein thrombosis or pulmonary embolism, and to avoid imaging tests. If the PTP is high or D‑dimer level is above the suggested thresholds, imaging is recommended. D‑Dimer assays offer high sensitivity and low specificity, as D‑dimer levels can be above the threshold in several other conditions than thrombosis, and they increase with age. As a result, there have been several proposals to improve the diagnostic accuracy of D‑dimer levels by adjusting the cutoffs according to patient characteristics, such as age, PTP, pregnancy, renal function, or cancer. D‑Dimer levels can also predict clinical severity of COVID‑19, and escalated anticoagulation based on D‑dimer levels can be associated with a lower risk of mortality in patients with severe COVID‑19. Finally, D‑dimer levels have been incorporated in prediction models for recurrent VTE to help identify patients who may benefit from prolonged anticoagulation.
Introduction
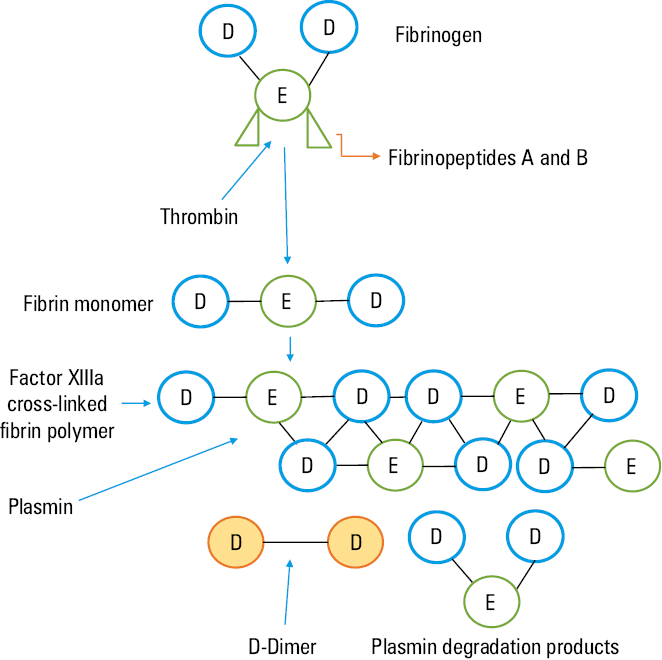
During hemostasis, activation of coagulation leads to the production of thrombin, which cleaves fibrinogen into fibrin monomers that finally form fibrin polymer. Thrombin also activates factor XIII, which stabilizes fibrin polymers with cross‑linked covalent bonds. Activation of fibrinolysis leads to the production of plasmin, which cleaves cross‑linked fibrin into various fragments, including D‑dimers1 (Figure 1). Plasmin produces several different degradation products with molecular weight (MW) ranging from 190 to over 10 000 kDa, and MW of D‑dimers is about 180 kDa.1 D‑Dimers are mainly cleared by the kidney and reticulo‑endothelial system, with a plasma half‑life of 6 to 8 hours.1,2 In physiological conditions, approximately 2%–3% of fibrinogen is converted into fibrin, which is then degraded by the fibrinolytic system.1,2 As a result, D‑dimers can be detected in low amounts in healthy individuals under physiological conditions. Plasma D‑dimer concentration depends on the extent of factor XIIIa‑stabilized fibrin formation, extent of fibrinolysis, and clearance of fibrin degradation products.
D‑Dimer level increases physiologically with age and during pregnancy and puerperium; it may be higher in African‑Americans and in smokers. Increased D‑dimer level is also observed in several pathologic conditions, in which stabilized fibrin is formed and subsequently degraded, such as in venous and arterial thrombosis, infectious diseases, neoplasms, trauma, surgery, liver disease, renal insufficiency, fibrinolytic therapy, disseminated intravascular coagulation (DIC), acute coronary syndromes, acute cerebrovascular events, subarachnoid hemorrhage, obstetric complications, or autoimmune disorders.3
D‑Dimer measurement
D‑Dimer level measurement was proposed as a laboratory test for the diagnosis of DIC in the 1970s; since then considerable advances have been made regarding its measurement, and its main clinical role is that in venous thromboembolism (VTE) diagnosis.2
Table 1 shows currently available D‑dimer commercial tests, the results of which are expressed either as “fibrinogen equivalent unit” (FEU), or “D‑dimer unit” (DDU, which is approximately half of FEU).2
Parameter | ELISAa | ELFAa | Latex‑enhanced immunoturbidimetric assay | Point‑of‑care |
Abbreviations: ELFA, enzyme‑linked immunofluorescence assay; ELISA, enzyme‑linked immunosorbent assay
a ELISA and ELFA assays modified from Linkins et al62 | ||||
Description | Quantitative | Quantitative | Quantitative | Quantitative |
Turnaround time | 2–4 h | 35 min | 15 min | 2–5 min |
Sensitivity (95% Cl), % | 94 (86–97) | 96 (89–98) | 93 (89–95) | 83 (67–93) |
Specificity (95% Cl), % | 53 (38–68) | 46 (31–61) | 53 (46–61) | 71 (57–82) |
Advantages | High sensitivity | High sensitivity, fully automated | Sensitivity comparable to ELISA, fully automated | Easy to perform, very high specificity |
Disadvantages | Not easy to perform, moderate specificity | Moderate specificity | Moderate specificity | Low sensitivity |
Simply speaking, different epitopes of D‑dimers can be the targets of monoclonal antibodies, and laboratory D‑dimer assays involve 2 steps. First, D‑dimers are captured by specific monoclonal antibodies, and second, the D‑dimer / antibody complexes are captured by other monoclonal antibodies. The types of monoclonal antibodies, substrates used to capture them, and staining or detection methods are the factors that differentiate available laboratory assays. The diagnostic accuracy of individual tests differs depending on the assay used, and D‑dimer values are not comparable across different tests.1
Although the labor‑intensive and time‑consuming Vidas (bioMérieux, Craponne, France) quantitative enzyme‑linked immunosorbent assays (ELISAs) are considered to be the reference standard for D‑dimer determination, they are impractical in routine clinical use. As a result, rapid, automated, and highly sensitive modified ELISAs have been developed, such as Vidas D‑Dimer (bioMérieux), which is a rapid enzyme‑linked immunofluorescence assay using single‑dose, ready‑to‑use reagents and offering rapid turnaround time.4
Unfortunately, an international standardization system for D‑dimer assay is lacking, and therefore each test method must be independently validated within the reference population.2,5
VTE, which includes deep vein thrombosis (DVT) and / or pulmonary embolism (PE), is a frequent acute disease that can be severe and life‑threatening, with a tendency to recur and often with delayed sequelae. A population‑based study found an incidence of DVT to be 0.93 per 1000 person‑years, and that of PE to be 0.5 per 1000 person‑years, with 30‑day mortality of 4.6% for DVT and 9.7% for PE.6
Nowadays, the reference diagnostic test for PE is computed tomography pulmonary angiography (CTPA), while venography has been replaced by compression ultrasonography (CUS) as the reference test for DVT. The availability of imaging diagnostic tests, together with an increase in the number of suspected VTE cases, resulted in a significant boost in the use of instrumental investigations to confirm VTE diagnosis. However, this is not only an expensive approach, but it also carries a risk of irradiation in the case of suspected PE, especially if we consider that less than 20% of the suspected cases are actually confirmed.6 Alternative diagnostic pathways are available, with a better cost‑benefit ratio, which makes it possible to select a higher‑risk population for instrumental investigations. The main objective of these diagnostic pathways is to identify the patients in whom anticoagulation can be avoided with acceptable safety, without reaching the certainty of exclusion that would be obtained only through the reference instrumental investigations.
Management studies evaluated the clinical evolution of patients who followed these diagnostic pathways (without resorting to the reference instrumental investigations). These studies demonstrated a rate of VTE complications of 1.5% to 2% at 3 months in the patients in whom the diagnosis was initially excluded.7 The rate of complications is comparable to that observed in the patients in whom the diagnosis was excluded by reference instrumental investigations.7
Evaluation of the clinical probability of VTE before performing a diagnostic test (“a priori” probability or pretest probability [PTP]) is the first step in all diagnostic algorithms, although the clinical diagnosis alone is not enough to exclude or confirm VTE.
The algorithms for VTE diagnosis are therefore based on various combinations of the following: 1) the use of criteria to obtain a correct stratification of the PTP (clinical decision rule); 2) the laboratory assay of D‑dimers; 3) the use of imaging diagnostic tests.
Since D‑dimers can be detected even in the plasma of healthy individuals, there is a threshold value (cutoff) for each D‑dimer measurement system, below which VTE can be excluded with very high probability. This cutoff value does not correspond to normal values in the healthy population, since clinicians are interested in excluding VTE. Therefore, it is essential that D‑dimer reference values are expressed as cutoffs and not as normal values. As a result, D‑dimer test results are interpreted as negative or positive when the measured level is, respectively, lower or higher than the pre‑established cutoff, as proposed by clinical studies and according to the clinical condition of the patient. However, the cutoff values may differ between various measurement methods, and this variability further limits the value of the test and makes its standardization more complex.
The D‑dimer test offers high sensitivity (>95%) for the diagnosis of VTE, that is, it produces few false‑negative results, and therefore has a high negative predictive value. As a result, its negativity, in combination with other tests, allows for VTE exclusion. In contrast, an important limitation is low specificity of the test (about 30% to 40%), or a high number of false positives, as D‑dimer levels may increase even if there is no thrombosis. Consequently, D‑dimer levels above the threshold value are not enough to confirm VTE due to their low positive predictive value.
The D‑dimer test sensitivity can also be reduced, in fact, it can be false‑negative if it is measured more than 7–10 days after the onset of symptoms,8,9 if a reagent has low sensitivity, or during anticoagulant treatment.4,10,11 In addition, naturally occurring polyreactive antibodies, autoantibodies, human antianimal antibodies, or rheumatoid factor, also known as heterophilic antibodies, can interfere with immunoassays, especially latex‑enhanced immunoturbidimetric D‑dimer tests,12 producing false‑positive results. The Food and Drug Administration has approved commercial clinical tests for VTE exclusion on the basis of management studies.13 The most commonly used cutoff value for diagnosing VTE is set at 500 μg/l (or the equivalent 0.5 mg/ml or 500 ng/ml) for the tests that use FEU as the unit of measurement; while the threshold value is approximately half of FEU for the tests that express the results in DDUs.4
The D‑dimer test should never be used alone, but always in combination with PTP. Such a combination can reduce the use of instrumental tests (expensive ones, such as CTPA and sometimes invasive, such as angiography). When PTP is not high or is low / moderate, a negative result of D‑dimer test allows for excluding VTE, but if the D‑dimer level is above the cutoff, it is necessary to proceed with the instrumental tests (CUS or CTPA according to clinical suspicion). Conversely, when PTP is intermediate or high, the D‑dimer level should not be measured, as it has been demonstrated that in these conditions the prevalence of PE or DVT is very high (>50%),13 and D‑dimer negative predictive value is significantly reduced (Figures 2 and 3).
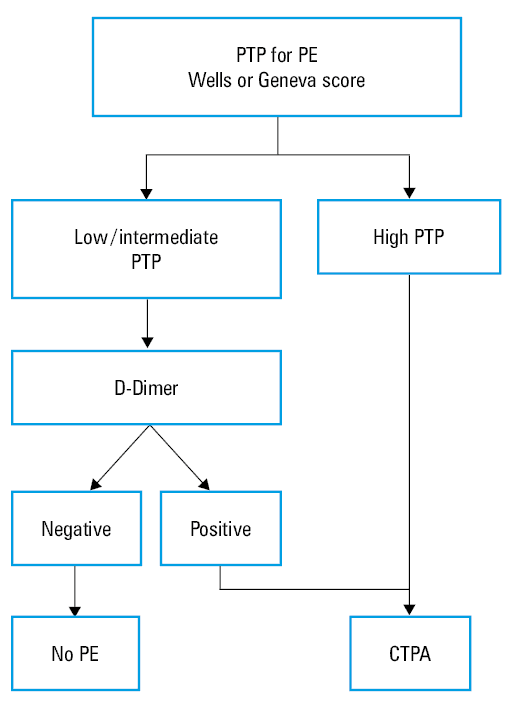
Abbreviations: CTPA, computed tomography pulmonary angiography; DVT, deep vein thrombosis; PE, pulmonary embolism; PTP, pretest probability
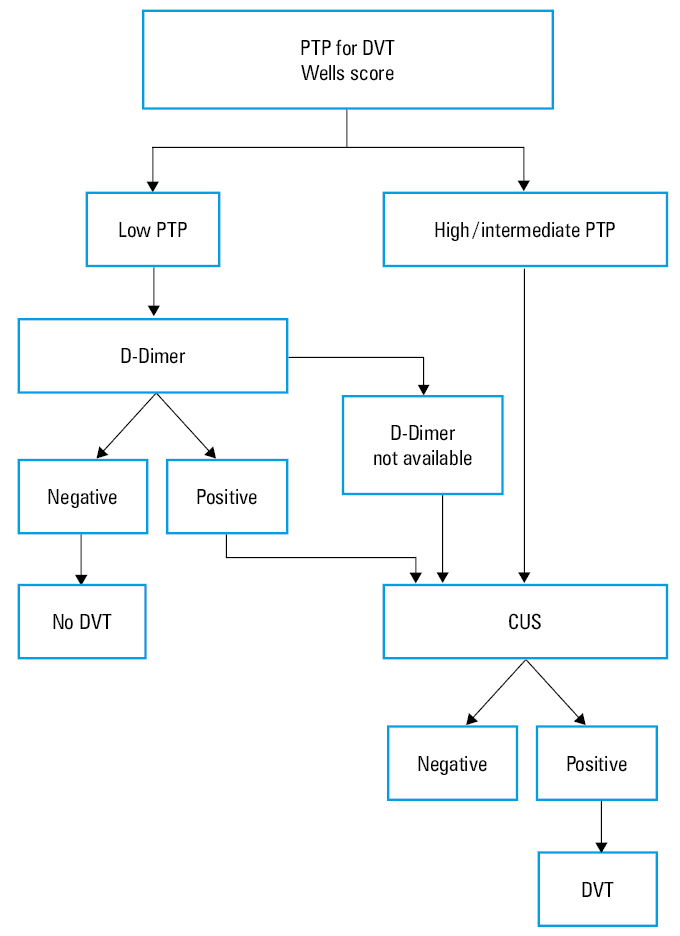
Abbreviations: CUS, compression ultrasonography; others, see Figure 2
Several approaches have been proposed to increase D‑dimer specificity by adjusting its cutoff to patient characteristics, with the aim to diminish the need for more expensive and time‑consuming imaging tests, such as CTPA, especially in the emergency departments. As a result, management studies mostly included outpatients.
How to increase efficiency (specificity) of D‑dimer assays in clinical practice
Several approaches have been proposed to adjust D‑dimer cutoffs to patient characteristics.
Age‑adjusted D‑dimer
The first approach was to adjust D‑dimer values according to age. The physiological increase in D‑dimer levels with age is an important limitation for the clinical use of this test, as the elderly suffer from high incidence of venous thrombotic events. It would be highly advantageous to have a test with adequate specificity to exclude VTE in this population. For this purpose, a strategy of using a D‑dimer test with cutoffs increasing with age has been proposed. According to this strategy, in individuals older than 50 years, the threshold value is calculated by multiplying the age by 10 (for tests expressing the results in FEUs). This way, for a 70‑year‑old person, the cutoff value will be 700 ng/ml, instead of 500 ng/ml. This strategy has been validated for suspected PE in the ADJUST‑PE (Age‑Adjusted D‑Dimer Cutoff Levels to Rule Out Pulmonary Embolism) management trial,14 with the demonstration of its advantageous cost‑to‑effectiveness ratio.15 It is already widely used in the cases of suspected DVT, especially in emergency departments, although it has not yet been validated with a specific management study.13 A systematic review and meta‑analysis showed that 8 prospective or retrospective studies approached DVT diagnosis with age‑adjusted D‑dimer, either isolated or with PE.16 They all showed improved utility of the age‑adjusted D‑dimer cutoff and similar safety as of the standard D‑dimer cutoff, although the results did not allow for direct comparisons due to heterogeneity in reporting.16
D‑Dimer adjusted according to pretest probability
The PEGeD (Pulmonary Embolism Graduated D‑Dimer) study17 addressed the diagnostic approach to PE exclusion using the Wells score with different cutoffs, to distinguish the patients with low and intermediate PTP and with D‑dimer cutoffs adapted to PTP. The Wells score of 0 to 4 points (instead of 0–1.5 points in the original Wells model) was categorized as low PTP, and the D‑dimer cutoff of 1000 ng/ml was used to exclude PE. The Wells score of 4.5 to 6 points (instead of 2–6 points) was categorized as moderate PTP, and the standard D‑dimer cutoff of 500 ng/ml was used to exclude PE. Finally, the Wells score equal to or above 6.5 points was considered as high PTP, and the patients with such a score were referred directly for CTPA.17
The outcomes of this study were comparable with those of prior studies on the efficiency of D‑dimer, as the number of CTPAs was reduced by 17.6% (when compared with the standard threshold of 500 ng/ml) without false negatives (0%; 95% CI, 0–0.29).17 This strategy had been previously validated also for the diagnosis of DVT.18 More recently, the PEGeD diagnostic algorithm was externally validated in an independent cohort of 3308 patients, among whom 1615 (49%) could have PE excluded according to the PEGeD algorithm, without the need for imaging.19 Of these patients, 38 (2.3%; 95% CI, 1.7–3.2) were diagnosed with symptomatic PE at initial testing or during 3‑month follow‑up.19 However, among the 414 patients with the D‑dimer level below 1000 ng/ml but above the age‑adjusted cutoff, VTE was detected in 36 individuals (8.7%; 95% CI, 6.4–11.8), indicating caution in this group of patients.19
PTP can be determined using clinical decision rules for PE (eg, the Wells score, the Revised Geneva Score), but also using the more recently proposed YEARS score, which encompasses 3 items: clinical signs of DVT, hemoptysis, and PE as the most likely diagnosis, with 1 point for the presence of each item.
In the case of 0 YEARS items, the D‑dimer cutoff is 1000 ng/ml, while in the case of at least 1 YEARS item, the D‑dimer cutoff is 500 ng/ml (Figure 4).20 van der Hulle et al20 prospectively validated the YEARS diagnostic algorithm and different cutoffs of D‑dimer levels in over 3000 patients with suspected PE, and found that the incidence of thromboembolic complications in the 3‑month follow‑up was low (0.43%; 95% CI, 0.17–0.88) among those in whom PE was initially excluded. A reduced number of CTPAs was also observed—by 14% when compared with the use of the classic strategy based on the Wells score and fixed D‑dimer cutoff (500 ng/ml), and by 8.7% in comparison with the Wells score and D‑dimer with age‑adjusted cutoff.20
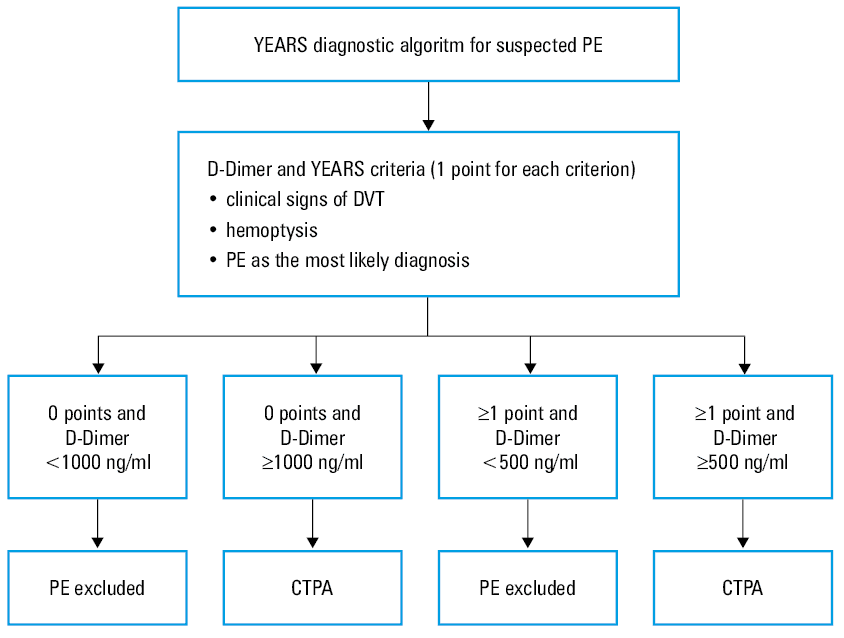
Abbreviations: see Figure 2
Using the YEARS strategy, van der Pol et al21 observed lower prevalence of subsegmental PE, determined by the reduced number of CTPAs performed for a higher D‑dimer cutoff, without an increased risk of VTE in the subsequent follow‑up.
With these results in mind, the latest European Society of Cardiology (ESC) guidelines22 indicate that the assessment of clinical probability of PE is the first step in PE diagnosis, and in all diagnostic algorithms for VTE. The ESC guidelines also recommend D‑dimer testing in patients with low / intermediate or unlikely PTP, preferably with a high‑sensitivity immunoassay.22 Both age‑adjusted and PTP‑adjusted cutoffs can be used, albeit with lower strength of recommendation for both cutoffs.22
Pregnancy‑adjusted D‑dimer
D‑Dimer levels increase physiologically and progressively in consecutive trimesters of pregnancy, and remain elevated in the puerperium. They return to normal 6 weeks postpartum. As a result, the usefulness of a D‑dimer assay may be limited. This makes VTE diagnosis challenging. The thrombotic risk increases during pregnancy and puerperium, while there is limited availability of diagnostic means for the reduced specificity of D‑dimer tests, and partial contraindication to irradiation during CTPA.23
Altered D‑dimer level in the third trimester is reported in approximately 25% of pregnant women. However, it can be clinically useful to measure it to exclude VTE in the case of negative results, despite the increase in false‑positive results. In the case of suspected lower limb DVT, ultrasound examination can be carried out, with possible serial scans, if the first finding is negative. The management of suspected PE is more complex, since CTPA entails high‑dose irradiation of the patient and the fetus.
D‑Dimer adjusted cutoffs have been proposed based on trimester (eg, first trimester = standard, second trimester = standard × 2, etc.),24,25 or according to clinical probability (YEARS) with different cutoffs (eg, 800 ng/ml or 1000 ng/ml).26 However, only 3 studies evaluated such management strategies, with different PE prevalence (4%–26%) and different negative predictive values (76%–100%) in a limited number of participants.24-26 The ESC guidelines recommend a diagnostic strategy based on clinical probability, D‑dimer, CUS, and CTPA to safely exclude PE in pregnancy.22 The exclusion of PE on the basis of a negative D‑dimer test is possible in about 10% of women with low or intermediate PTP on the Geneva scale, a percentage which decreases to 4% in the third trimester.22
Renal function–adjusted D‑dimer
D‑dimer is excreted by the kidney and its level increases with decreasing glomerular filtration rate (GFR). As a result, the clinical usefulness of D‑dimer decreases with renal impairment. However, a negative D‑dimer assay can rule out PE in a substantial proportion of patients with non‑high clinical probability, avoiding exposure to contrast media.
Few studies have evaluated D‑dimer cutoffs adjusted according to renal function.27-30 In a single‑center retrospective data analysis of electronic health care records of 14 447 emergency department patients with suspected VTE, adjusted D‑dimer levels were applied (as previously determined >333 µg/l for estimated GFR [eGFR] >60 ml/min/1.73 m2, >1306 µg/l for eGFR 30–60 ml/min/1.73 m2, and >1663 µg/l for eGFR <30 ml/min/1.73 m2).28 Negative predictive value (>99%), sensitivity (91.2% vs 93.4%), and specificity (42.7% vs 50.7%) were similar to those of the conventional D‑dimer cutoff used to rule out VTE (<500 µg/l).28 However, no management studies are available on renal function‑adjusted D‑dimer for exclusion of VTE, and such an approach cannot be recommended in clinical practice.
D‑Dimer adjusted to COVID‑19
Severe acute respiratory syndrome due to SARS‑CoV‑2 infection is associated with increased D‑dimer levels, especially in the case of concomitant VTE. Several authors have proposed tailoring the D‑dimer cutoffs to the specific context of COVID‑19, with suggested levels of 1000, 2000, 3000, or even higher than 6000 ng/ml to better identify the patients with PE.31-34
Planquette et al35 conducted a French, multicenter, retrospective cohort study among 774 COVID‑19 patients with suspected PE (Co‑LEAD study). D‑Dimer threshold adjusted to the extent of lung damage found on CT was extrapolated by a derivation set. Its safety was assessed in an independent validation set. In the derivation set (n = 337), D‑dimer safely excluded PE, with 1 false negative, when using a 900 ng/ml threshold for lung damage extent below 50%, and 1700 ng/ml for lung damage extent equal to or greater than 50%. In the derivation set, the algorithm sensitivity was 98.2% (95% CI, 94.7–100), and its specificity was 28.4% (95% CI, 24.1–32.3).35 The negative likelihood ratio was 0.06 (95% CI, 0.01–0.44). Using the Co‑LEAD algorithm, 76 of 250 COVID‑19 patients (30.4%) with suspected PE could be managed without CTPA, and 88 patients (35%) required 2 CTPAs.35 The algorithm of the Co‑LEAD study could safely exclude PE, and reduce the use of CTPA in COVID‑19 patients. Chassagnon et al36 retrospectively evaluated COVID‑19 outpatients from 15 university hospitals who underwent CTPA for suspected PE. They took into account D‑dimer levels, variables of the revised Geneva and Wells scores, as well as laboratory findings, and clinical characteristics related to COVID‑19 pneumonia, and they reviewed CTPA reports for the presence of PE and the extent of lung damage. PE rule‑out strategies were based solely on D‑dimer tests using different thresholds, and then the revised Geneva and Wells scores, and a COVID‑19 PE prediction model built on the same dataset, were compared.36 In total, 124 out of 1369 included patients (9.1%) were PE‑positive. Failure rate and efficiency of D‑dimer cutoff above 500 ng/ml were 0.9% (95% CI, 0.2%–4.8%) and 10.1% (95% CI, 8.5%–11.9%), respectively, increasing to 1% (95% CI, 0.2%–5.3%) and 16.4% (95% CI, 14.4%–18.7%), respectively, for an age‑adjusted D‑dimer level.36 D‑dimer level above 1000 ng/ml resulted in an unacceptable failure rate of 8.1% (95% CI, 4.4%–14.5%). The best performance of the revised Geneva and Wells scores was obtained using the age‑adjusted D‑dimer cutoffs. They had the same failure rate of 1% (95% CI, 0.2%–5.3%), while efficiency was 16.8% (95% CI, 14.7%–19.1%), and 16.9% (95% CI, 14.8%–19.2%) respectively. These data indicate that the same strategy to safely exclude PE in non–COVID‑19 patients should be applied in those with COVID‑19. The COVID‑19 PE prediction model had a minor added value.36
Comparison of management strategies with different adjusted D‑dimer cutoffs
There are limited management studies comparing different D‑dimer thresholds for VTE exclusion. A systematic review and meta‑analysis of 68 studies involving 141 880 patients showed that D‑dimer standard cutoff had high sensitivity (0.99; 95% CI, 0.98–0.99) and limited specificity (0.23; 95% CI, 0.16–0.31).37 Sensitivity was similar for age‑adjusted (0.97; 95% CI, 0.96–0.98) and YEARS algorithm (0.98; 95% CI, 0.91–1), but lower than for PTP‑adjusted (0.95; 95% CI, 0.89–0.98) and COVID‑19–adjusted thresholds (0.93; 95% CI, 0.82–0.98).37 All adjustment strategies had higher specificity than standard D‑dimer cutoffs (age, 0.43; 95% CI, 0.36– 0.5; PTP, 0.63; 95% CI, 0.51–0.73; YEARS algorithm, 0.65; 95% CI, 0.39–0.84; and COVID‑19, 0.51; 95% CI, 0.4–0.63).37 The YEARS algorithm had the best negative likelihood ratio (0.03; 95% CI, 0.01–0.15), followed by age‑adjusted (0.07; 95% CI, 0.05–0.09), PTP‑adjusted (0.08; 95% CI, 0.04–0.17), and COVID‑19–adjusted thresholds (0.13; 95% CI, 0.05–0.32).35 A limited number of studies for pregnancy and renal function‑adjusted cutoffs did not allow for carrying out a meta‑analysis for these populations.37 That meta‑analysis suggests that adjustment of D‑dimer thresholds to patient‑specific factors is safe, and can considerably limit the number of imaging examinations. However, robustness, safety, and efficiency are considerably variable among different adjustment strategies with a high degree of heterogeneity.37
D‑Dimer and COVID‑19 treatment and prognosis
D‑Dimer levels can be valuable in predicting clinical severity and prognosis of COVID‑19. Elevated D‑dimer levels identified individuals at risk of thrombotic complications among 32 636 patients hospitalized for COVID‑19 in the American Heart Association COVID‑19 Cardiovascular Disease Registry.31 Several studies also found that increased D‑dimer level is associated with the disease progression and death.38 Varikasuvu et al39 pooled the results of 68 unadjusted and 39 adjusted clinical studies (for a total of 42 613 patients), and reported that D‑dimer values at admission were strongly associated with increased risk of the disease progression (adjusted odds ratio [OR], 1.64; 95% CI, 1.29–2.09), including severe / critical illness (adjusted OR, 2; 95% CI, 1.65–2.14), and death (adjusted OR, 1.36; 95% CI, 1.2–1.54).37 Naymagon et al40 found that COVID‑19–hospitalized patients with progressively increasing D‑dimer levels had nearly 80% and 70% higher risk of needing mechanical ventilation or dying, respectively, than those with a stable D‑dimer concentration.40
A systematic review and meta‑analysis41 of a total of 23 studies including 3423 patients showed higher D‑dimer levels in the severe COVID‑19 group vs the nonsevere COVID‑19 group, in the intensive care unit (ICU) patients vs non‑ICU patients, and in patients who died vs those who survived.
Many randomized trials investigated if increased or therapeutic doses of heparins (mostly low‑molecular‑weight heparin [LMWH]) have additional advantages over standard‑dose heparins, in both noncritically ill and critically ill patients with COVID‑19.42,43
No advantages of using increased or therapeutic doses of heparins in critically ill populations were found, with an enhanced risk of major bleeding.42,43 However, in noncritically ill populations, 2 trials showed that a therapeutic dose of heparin (mostly LMWH) reduced the need for organ support and improved survival until hospital discharge or reduced a composite of major thromboembolism and all‑cause mortality without a significant increase in major bleeding.43 Inclusion criteria in these trials were elevated D‑dimer levels (2 or 4 times over the upper limit of normal [ULN]) or increased oxygen requirements, and greater absolute treatment effects in the populations with elevated D‑dimer levels were shown.43 Guidelines on antithrombotic treatment for hospitalized COVID‑19 patients suggest or recommend standard‑dose heparins for thromboprophylaxis in a medical ward and critically ill patients, and the use of therapeutic‑dose heparin (LMWH) in noncritically ill patients, especially those with elevated D‑dimer levels (>2 times ULN) or increased oxygen requirements.44,45 In a prospective cohort study, intermediate‑intensity thromboprophylaxis with enoxaparin at 1 mg/kg body weight once daily was administered to COVID‑19 patients not on anticoagulants but with a high risk of VTE, associated with prior VTE, known thrombophilia, active cancer, active inflammatory bowel disease, age over 75 years, immobilization (especially during oxygen therapy or mechanical ventilation), or rapid increase in D‑dimer levels by 1000 ng/ml per day. Standard thromboprophylaxis was also administered to patients, and therapeutic doses of heparins were given to patients on anticoagulants. This thromboprophylaxis protocol, approved at the local institution, was associated with a relatively low risk of thromboembolism (4.4%; 16 of 350 patients) and bleeding (9%; 31 of 350 patients).46
D‑Dimer level is more frequently elevated in COVID‑19 patients with postdischarge clinical sequelae, and the increased D‑dimer level, which reflects a residual prothrombotic state, could be detected in as many as 15% of these patients, more frequently in those with severe respiratory disease and enhanced inflammation.5,47 Li et al48 conducted a clinical study in nearly 3000 adult patients hospitalized for COVID‑19, and found that the patients with highly increased peak D‑dimer level (ie, >3000 ng/ml) had a nearly 4‑fold higher risk (OR, 3.76; 95% CI, 1.86–7.57) of developing postdischarge VTE episodes.
Finally, D‑dimer elevation post–COVID‑19 vaccination is associated with an increased risk of developing vaccine‑induced thrombocytopenia and thrombosis.49
D‑Dimer and cancer
VTE prevalence in cancer patients is increased in the intrinsic prothrombotic state and concomitant presence of VTE risk factors, such as reduced mobility, chemotherapy, and surgical therapy in addition to the tumor site, histology, and grade.50 Thromboembolic complications in these patients are associated with a reduced overall survival, and represent the second most common cause of death. In outpatients, the risk of VTE complications in the first 6 months after cancer diagnosis is estimated to be approximately 10% to 15%.51
The specificity and positive predictive value of the D‑dimer tests are reduced in cancer patients due to their prothrombotic state. Therefore, in the case of suspected VTE associated with cancer, the current literature does not support the usefulness of D‑dimer measurements and PTP but underlines the need for instrumental investigations. In fact, cancer on its own increases the clinical probability of VTE in the most commonly used prediction models, such as the revised Geneva score (active cancer adds 2 points to a threshold of 4 points for a moderate probability category) and the DVT Wells score (active cancer accounts for 1 point resulting in the moderate probability category).52 As a result, cancer patients are often classified as having moderate or high clinical probability of VTE. To improve VTE exclusion criteria, several approaches have been proposed, such as ordering systematic imaging tests, new diagnostic algorithms based on clinical probability assessment, and adjusted D‑dimer thresholds. However, the population of cancer patients still lacks a dedicated diagnostic algorithm for VTE diagnosis.
More recently, a prospective multicenter observational study showed that the plasma D‑dimer levels in the highest quartiles were associated with the risk of death in 135 patients with ischemic stroke and active cancer.53
In unprovoked VTE, that is, in the absence of external risk factors, markedly elevated D‑dimer values at VTE diagnosis could be related to a greater risk of occult cancer. D‑Dimer concentrations above 4000 ng/ml were independently associated with higher probability of occult cancer in unprovoked VTE.54 Therefore, at the time of diagnosis of unprovoked VTE, the D‑dimer assay could serve as a surrogate marker to indicate the likelihood of associated cancer.54
Stratification of the risk of venous thromboembolism recurrence: evaluation of the duration of anticoagulant treatment
The risk of VTE recurrence in the first year after discontinuing anticoagulant therapy is estimated at about 10%, and it is higher in men and after an unprovoked index event. This risk rises to about 30% in 10 years. As a result, stratifying the risk of recurrence for individual patients for extension of anticoagulant treatment is highly relevant. Clinical studies have shown that the risk of VTE recurrence is higher in the patients with a positive D‑dimer value after at least 3 months of anticoagulant therapy with vitamin K antagonists than in those with a negative D‑dimer value; this finding being more evident in men.55 As a result, D‑dimer measurements can help stratify the risk of VTE recurrence when stopping anticoagulation, especially after unprovoked VTE.
Recently, a multicenter, prospective cohort study APIDULCIS (Apixaban for Extended Anticoagulation)56 assessed an algorithm incorporating serial D‑dimer testing, age-, and sex‑adjusted cutoffs. Only the patients with a positive test received reduced‑dose apixaban (2.5 mg twice daily). A total of 732 outpatients aged 18 to 74 years, anticoagulated for at least 12 months after the first unprovoked VTE (75.8%, the remaining associated with weak risk factors), were enrolled. Of those, 446 individuals (60.9%) had positive D‑dimer results and received apixaban (2.5 mg twice daily), whereas 286 (39.1%) had persistently negative results and remained without anticoagulation. The study was interrupted after a planned interim analysis for the high rate of primary outcomes (7.3%; 95% CI, 4.5–11.2), including symptomatic proximal DVT or PE recurrence, death from VTE, and major bleeding observed in patients off anticoagulation, when compared with those receiving low‑dose apixaban (1.1%; 95% CI, 0.4–2.6; adjusted hazard ratio 8.2; 95% CI, 3.2–25.3). This incidence was not only higher than expected based on observations from previous studies, but also higher when compared with the results of a similarly designed study.55 Furthermore, the incidence of VTE events was much higher than that recorded in the patients who continued anticoagulation with reduced‑dose apixaban. A potential explanation was that the pandemic has affected these results, directly or by various mechanisms, contributing to an increased risk of recurrences that could not be predicted by negative D‑dimer assay performed at the time of the study enrollment. It is well established that the COVID‑19 pandemic is associated with an increased rate of VTE events, which is not limited to the seriously affected patients.57
Prediction models for the risk of venous thromboembolism recurrence
Prediction models have been proposed to establish the recurrence risk of idiopathic or unprovoked VTE in the patients who have completed 3 to 6 months of anticoagulant therapy, and to assess whether such a risk is low enough to stop the therapy. There are as many as 17 models for VTE recurrence available. Sex, age, type, and location of VTE event were the most often used variables, with D‑dimer measurement incorporated in 8 of these scores during anticoagulation or after its interruption.58 In the latter case, the interval varies from 3–5 weeks to 3 months, and this may be less convenient clinically, as the patients have to stop and then possibly resume treatment. D‑Dimer cutoffs for excluding VTE have been employed, together with sex- and age‑adjusted cutoffs.55,56 Most models encompass a scoring system that calculates a total score, which is then classified as a high or low risk. The Vienna prediction model (VPM) proposes a nomogram that considers sex, VTE location (distal vs proximal / PE) and the D‑dimer value measured 1 month after stopping treatment on a continuous scale (measured as µg/l).59 It assigns each patient a percentage of risk of VTE recurrence in 60 months, on the basis of which a clinician can decide on continuation or suspension of therapy. Nine of these models have been externally validated with modest C statistic around 0.55 to 0.65.58 Only 2 models were employed in management studies: the HERDOO2 for women (men are considered at high risk and therefore they continue anticoagulation) in the REVERSE II study (Clinical Decision Rule Validation Study to Predict Low Recurrent Risk in Patients with Unprovoked Venous Thromboembolism),60 and the VPM in the VISTA study.61
In the REVERSE II study, the HERDOO2 score included D‑dimer measured during anticoagulation with a cutoff of 250 ng/ml, together with the presence of skin hyperpigmentation, edema or erythema of a lower limb, body mass index greater than or equal to 30 kg/m2, age above 65 years, assigning 1 point for the presence of each parameter.60 In the primary analysis, low‑risk women who discontinued anticoagulants developed recurrent VTE in 3% per patient‑year (95% CI, 1.8%–4.8%).56 In the high‑risk women and men who discontinued anticoagulants, VTE occurred in 8.1% (95% CI, 5.2%–11.9%).60 Women with the first unprovoked VTE event and none or 1 of the HERDOO2 criteria have a low risk of recurrent VTE, and can safely discontinue anticoagulants after completing short‑term treatment.60
The VISTA randomized trial compared usual care with the VPM, and showed that application of the VPM in all patients with unprovoked VTE was unlikely to reduce overall recurrence risk.61 Yet, in the individuals with a low predicted risk of recurrence, the observed rate was also low, suggesting that it might be safe to stop anticoagulant treatment.61
Risk assessment is particularly important in the modern era of direct oral anticoagulants, considering that therapeutic reintroduction is simple, possible even at low doses, but not completely devoid of a bleeding risk.
Conclusions
D‑Dimer testing is a key component of diagnostic algorithms for the exclusion of VTE due to its high sensitivity and negative predictive value that allow for avoiding imaging examinations. However, the specificity of D‑dimer standard cutoffs is unsatisfactory.
Adjustment of D‑dimer cutoffs to patient characteristics has been proposed to increase their specificity. Management studies have shown that age- and PTP‑adjusted D‑dimer cutoffs can be safely incorporated into diagnostic algorithms for VTE exclusion with further reduction of imaging examinations. However, there is a lack of dedicated algorithms for VTE diagnosis in cancer patients. D‑Dimer tests have a prognostic value and can aid in the choice of escalated thromboprophylaxis with anticoagulants in COVID‑19 patients. Prediction models for the risk of recurrence after unprovoked VTE have also incorporated D‑dimer testing during and after stopping anticoagulation, although with modest discriminatory potential. The 2 management studies employing 2 different prediction models brought about conflicting results.
- Weitz JI, Fredenburgh JC, Eikelboom JW. A test in context: D‑dimer. J Am Coll Cardiol. 2017; 70: 2411‑2420. | Crossref
- Favresse J, Lippi G, Roy PM, et al. D‑dimer: preanalytical, analytical, postanalytical variables, and clinical applications. Crit Rev Clin Lab Sci. 2018; 55: 548‑577. | Crossref
- Iwaniec T, Celińska‑Löwenhoff M, Zaręba L, et al. Chronic prothrombotic tendency in patients with granulomatosis with polyangiitis. Pol Arch Intern Med. 2021; 131: 666‑672. | Crossref
- Riley RS, Gilbert AR, Dalton JB, et al. Widely used types and clinical applications of D‑dimer assay. Lab Med. 2016; 47: 90‑102. | Crossref
- Lippi G, Mullier F, Favaloro EJ. D‑dimer: old dogmas, new (COVID‑19) tricks. Clin Chem Lab Med. 2022; 61: 841‑850. | Crossref
ARTICLE INFORMATION