Recent guidelines addressing chronic rhinosinusitis with nasal polyps: practical aspects
Key words: chronic rhinosinusitis, guidelines, nasal polyps



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Recent guidelines addressing chronic rhinosinusitis with nasal polyps: practical aspects
Chronic rhinosinusitis (CRS) is common in adults. It is diagnosed based on a high index of suspicion alongside objective means of assessing sinus inflammation. Determining the impact of CRS on patient quality of life is an important starting point for discussions regarding treatment, and is critical for longitudinal assessment of response to specific treatments. CRS can be further categorized by the presence or absence of nasal polyps. Recent Joint Task Force on Practice Parameters Grading of Recommendations Assessment, Development, and Evaluation guidelines for the management of CRS with nasal polyps (CRSwNP) focused on 3 treatment options: intranasal corticosteroids with multiple delivery methods, biologics (monoclonal antibodies targeting type 2 inflammation), and aspirin therapy after desensitization, which only applies to the subset of patients with CRSwNP who experience acute respiratory reactions following nonsteroidal anti‑inflammatory drug ingestion. The authors of the guidelines made conditional recommendations in favor of each of these 3 treatment options, highlighting the importance of shared decision‑making when choosing appropriate therapy for individuals with CRSwNP.
Recognizing chronic rhinosinusitis
Medical professionals who diagnose and treat adults are likely to encounter many patients who suffer from chronic rhinosinusitis (CRS). The estimated prevalence of CRS ranges from 2% to over 20% in some regions.1 In Poland, the prevalence of self‑reported physician‑diagnosed CRS was 11%, 12%, and 11%, respectively, in Katowice, Kraków, and Łódź. According to survey‑based symptom criteria, as per the European Position Paper on Rhinosinusitis and Nasal Polyps standard, the prevalence was 15%, 20%, and 14% for those same cities.1 When using stricter criteria to diagnose CRS, including objective evidence of sinus inflammation, the prevalence rates are nearer to 5%.2
Identifying patients with CRS requires a high index of suspicion, as the cardinal symptoms of CRS—nasal obstruction, thick nasal discharge, hyp- or anosmia, and facial pain / pressure / headache—are commonly noted in several overlapping, and sometimes coexisting, disorders. Among the patients who experience 2 of the 4 cardinal symptoms of CRS for at least 12 consecutive weeks, about a half will have a diagnosis confirmed on nasal endoscopy and / or sinus computed tomography (CT) imaging.3 The differential diagnosis of CRS includes multiple rhinitis syndromes (allergic rhinitis, nonallergic rhinitis, rhinitis medicamentosa, and others), acute and recurrent sinusitis (subsidence of symptoms and signs in‑between disease episodes lasting less than 12 weeks), and headache syndromes (eg, tension or migraine headaches, especially when facial pain, pressure, and headache are the primary symptoms). There are several “red flag” symptoms and signs that should prompt immediate evaluation and referral for further diagnostic procedures. They include symptoms or signs of orbital involvement, severe headache with meningeal signs, high fever, severe / recurrent epistaxis, or the state of severe immunocompromise and being at risk for invasive fungal sinusitis. Once the “red flags” have been reviewed and found to be absent, if CRS remains the most likely diagnosis, a decision about proceeding directly with treatment or performing additional investigations to increase diagnostic certainty can be made. This is a decision that should be made with the patient’s input. For patients and health care professionals who value diagnostic certainty, referral to an otorhinolaryngologist and / or for a sinus CT scan can provide clarity.4 For patients and health care professionals who are more comfortable with uncertainty, starting treatment for CRS (eg, with intranasal corticosteroids [INCSs]) may be preferred. Severity and duration of symptoms, alongside the response to any previous therapies are additional factors that may influence the decision to perform confirmatory imaging or endoscopy prior to a treatment trial. Figure 1 depicts a simple approach to diagnosing CRS.
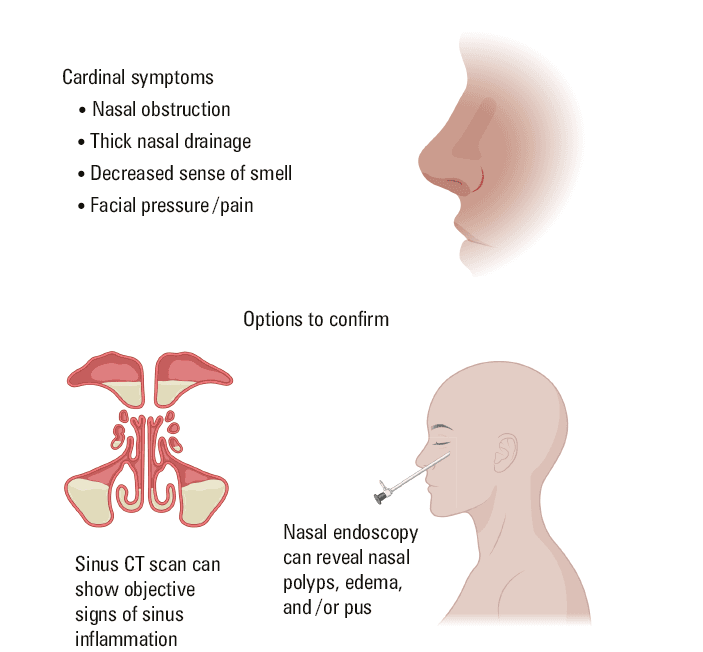
Abbreviations: CT, computed tomography
Diagnosing the chronic rhinosinusitis type
Even after a diagnosis of CRS is made, the diagnostic workup is incomplete. CRS is heterogeneous in its underlying pathophysiology, prognosis, severity, and response to treatment, similar to other airway inflammatory disorders, such as asthma. While some therapies, including saline rinse and INCSs, are used in almost every type of CRS, others only apply to specific disease subtypes. The starting point for selecting the best treatment option is to differentiate the patients who have nasal polyps (CRSwNP) from those who do not (CRSsNP) (Figure 2). Some practical recommendations for diagnosing nasal polyps include the application of nasal endoscopy (following decongestant application) using an otoscope with a nasal speculum to visualize areas that cannot be easily seen. If the polyps are large, their identification is easily possible, especially for an examiner experienced in such procedures. When medical students, internal medicine residents, or allergy‑immunology fellows‑in‑training are learning how to perform the nasal exam, it is common for them to confuse a swollen and pale middle turbinate for a polyp. In addition, cysts seen within the sinuses on CT imaging are frequently mistaken for nasal polyps. Finally, patients with prior nasal polyposis may no longer have nasal polyps following surgical and medical treatment. To identify the disease subtype in those patients (CRSwNP vs CRSsNP), it is important to review their prior examination results and operative notes.
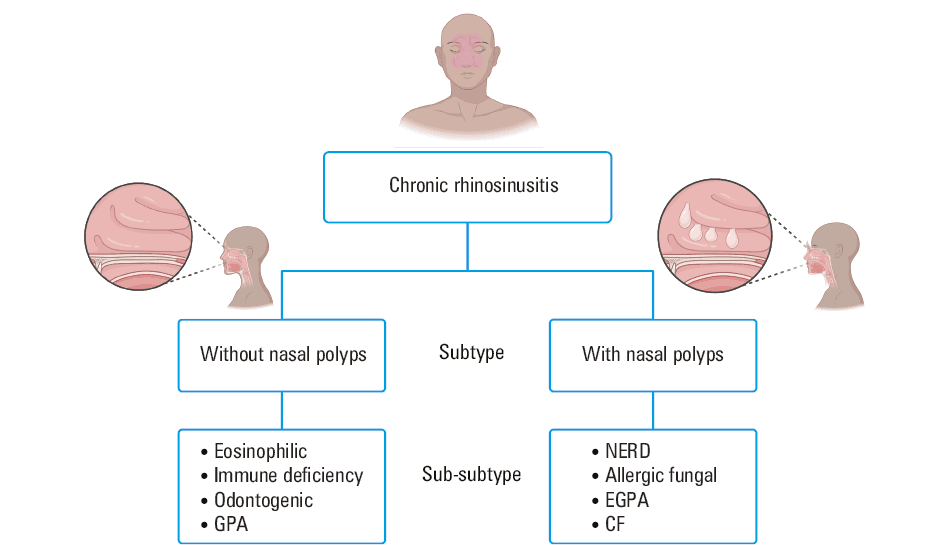
Abbreviations: CF, cystic fibrosis; EGPA, eosinophilic granulomatosis with polyangiitis; GPA, granulomatosis with polyangiitis; NERD, nonsteroidal anti‑inflammatory drug–exacerbated respiratory disease
After confirming whether a patient has CRSwNP or CRSsNP, the diagnostic workup is still not complete. Patients with CRSwNP may have one of several sub‑subtypes of the disease: nonsteroidal anti‑inflammatory drug (NSAID)-exacerbated respiratory disease (NERD), allergic fungal rhinosinusitis (AFRS), cystic fibrosis (CF), or eosinophilic granulomatosis with polyangiitis (EGPA). Most CRSwNP patients in the United States and Europe are type 2 (T2) inflammation–high and have increased tissue eosinophilia. In Asia, more patients with CRSwNP have neutrophilic tissue inflammation.5 Patients with NERD experience acute respiratory symptoms shortly after taking NSAIDs. They often have severe CRSwNP, and almost always have asthma. Patients with AFRS have fungal hyphae on pathologic examination, as well as allergic mucin, immunoglobulin (Ig) E sensitivity to 1 or more dematiaceous fungi, elevated total serum IgE level, and can be recalcitrant to initial therapies. Patients with CF usually have notable pulmonary and gastrointestinal symptoms along with frequent Pseudomonas colonization or infection. Patients with EGPA have asthma, nasal polyps, high levels of peripheral blood eosinophils, evidence of vasculitis on tissue biopsy, and sometimes also peripheral neuropathy, rash, and detectable perinuclear antineutrophil cytoplasmic antibodies (ANCA; mostly myeloperoxidase ANCA).
In patients with CRSsNP, there are also sub‑subtypes to consider: odontogenic sinusitis, primary immune deficiency (PID), and GPA. Patients with odontogenic sinusitis are more likely to have maxillary and unilateral disease, and a history of dental problems / surgeries. PID is suggested by the presence of severe, unusual, and / or frequent infections. Patients with GPA are likely to have significant crusting, osteitis of the bones that border the sinus cavities, pulmonary disease, and positive cytoplasmic ANCA (proteinase 3 ANCA). ANCA can be detected by enzyme‑linked immunosorbent assay or indirect immunoflourescence. It is important to note that, regardless of the detection method, interpretation of ANCA tests requires nuance, and that ANCA‑related vasculitides can have heterogenous clinical presentations.6 Many patients with CRSsNP are eosinophilic and therefore may respond to treatments in a similar fashion to those with CRSwNP. Finally, environmental factors, such as smoking, air quality, and allergens, can each play an exacerbating role and should be addressed, when possible, in patients with all types of CRS.
Patients with CRS frequently have comorbid asthma, chronic obstructive pulmonary disease, or bronchiectasis. Complete pulmonary history data analysis, coupled with investigations such as pulmonary function testing and chest imaging, will often uncover these related diagnoses.
Assessment of severity and impact on quality of life
Before discussing treatment options with the patient, it can be helpful to have a full picture of the impact of CRS on their quality of life (QoL). There are several validated questionnaires for CRS‑specific QoL that can be used at baseline to best understand the various ways CRS may impact patient life. The same questionnaires can be also used longitudinally to help assess response to treatments. For example, the Sinonasal Test‑22 (SNOT‑22) is a questionnaire that has been used frequently in research studies. The SNOT‑22 scale ranges from 0 (perfect score—no symptoms or impact on QoL) to 110 (the highest possible score suggesting severe symptoms and major impact on QoL). The SNOT‑22 has a minimally important difference (MID) of 9 to 12 points that signifies improvement.7,8 A patient whose SNOT‑22 score changes by more than 9 to 12 points, as compared with the previous result, is likely to experience a patient‑important change in their disease status, where a decrease in the score suggests improvement, and a higher score suggests deterioration.
When patients with CRS were interviewed about which outcomes mattered the most to them, not surprisingly, they listed nasal symptoms and the impact on their QoL as the top concerns over other outcomes, such as sinus imaging results and the size of polyps on examination.9 For this reason, recent guidelines considered disease‑specific QoL a critical outcome when making recommendations.10
Considering all potential treatment options for chronic rhinosinusitis
There are 3 recent guidelines on the management of CRS that can be helpful when selecting treatment options: the European Position Paper on Rhinosinusitis and Nasal Polyps (EPOS2020) guideline,5 the International Consensus Statement on Allergy and Rhinology: Rhinosinusitis 2021 (ICAR‑RS),3 and The Joint Task Force on Practice Parameters (JTFPP) Grading of Recommendations Assessment, Development and Evaluation (GRADE)11 for CRSwNP.10 EPOS2020 and ICAR‑RS are comprehensive guidelines that review the pathophysiology, prognosis, diagnostics, and almost all treatment options. They differ slightly in their focus on surgical techniques and, in small ways, with respect to the level of confidence for specific treatments.12 The JTFPP GRADE guidelines include a systematic summary of all available evidence for 3 specific treatments for CRSwNP: INCSs, biologics, and aspirin therapy after desensitization (ATAD). The last treatment, ATAD, applies only to patients with NERD.
Recent guidance on the treatment of chronic rhinosinusitis with nasal polyps
The JTFPP GRADE guidelines sought all trial evidence for INCS use in CRSwNP, and used a network meta‑analysis technique to compare several outcomes.13 INCSs have long been considered the standard of care in CRSwNP. They can be delivered in a varying manner (and with different drugs, doses, and frequencies). The JTFPP GRADE guidelines for CRSwNP found low‑certainty evidence for most outcomes when individual INCSs were considered.10 A list of different INCS types for CRSwNP and the outcomes expected for each delivery method are presented in Table 1. The 2 most beneficial INCS delivery methods for impacting disease‑specific QoL (as measured on the SNOT‑22 scale) both failed to exceed the 9- to 12‑point threshold as compared with placebo (rinse, –6.83 points; 95% CI, –11.94 to –1.71; exhalation delivery system, –7.96 points; 95% CI, –14.64 to –1.08).10 On the other hand, 3 delivery methods exceeded the preset threshold (>0.3 points on a 0–3 visual analog scale [VAS]) for improving nasal obstruction symptoms: spray (–0.51 points; 95% CI, –0.61 to –0.41), exhalation delivery system (–0.35 points; 95% CI, –0.51 to –0.18), and stent (–0.31 points; 95% CI, –0.54 to –0.08).10
Method of INCS delivery | Description | Beneficial for |
Abbreviations: INCS, intranasal corticosteroid; QoL, quality of life | ||
Spray | Corticosteroids are suspended in an aqueous medium with varying concentrations. The patient pushes the applicator, and the spray is delivered laterally to each nostril. |
|
Rinse | Corticosteroids are suspended in a saline solution and then delivered into the nostril using a high‑volume flush. |
|
Exhalation delivery system (EDS) | Corticosteroids are suspended in an aqueous medium. By blowing out through the EDS, the patient seals the soft palate, isolating the nose from downstream airways, thus preventing drug dispersion. |
|
Stent / dressing | Stents or dressing containing corticosteroids are placed in the nasal cavities by surgeons. The corticosteroids are released slowly over time. |
|
Drops | Corticosteroids are suspended in an aqueous medium. The drops are instilled with the patient assuming a specific body position, based on the intended area of delivery (as directed by a health care professional). |
|
The recommendation to use INCSs for CRSwNP treatment is conditional. The factors that may be important to discuss with the patient include the effectiveness (particularly the small treatment effect size), safety, costs, and availability of different delivery methods.
The second treatment method evaluated in the JFTPP GRADE guidelines for CRSwNP are biologics. The different biologics applicable in CRSwNP are similar in that they all are monoclonal antibodies that target aspects of the T2 inflammatory pathway, which is thought to be dysregulated in most patients with CRSwNP. On the other hand, they differ in that they target specific pathways, including IgE, interleukin (IL)-5, and IL‑4/IL‑13. The main findings from the network meta‑analysis are that biologics have larger treatment effects than INCSs, and that the treatment outcomes differ among individual biologic classes.14 Dupilumab (–19.91 points; 95% CI, –22.50 to –17.32) and omalizumab (–16.09 points; 95% CI, –19.88 to –12.30) were the most beneficial when considering disease‑specific QoL assessed with the SNOT‑22 scale.14 With respect to nasal symptom scores (assessed on a 0–10 VAS scale with a MID of 1 point), dupilumab (–3.25 points; 95% CI, –4.31 to –2.18), omalizumab (–2.09 points; 95% CI, –3.15 to –1.03), and mepolizumab (–1.82 points; 95% CI, –3.13 to –0.50) were the most beneficial.14 Biologics often need to be used for 6 months so that their potentially beneficial effects can be observed. The most commonly reported adverse effect of any of the abovementioned biologics is a local injection site reaction. Dupilumab also has a unique potential side effect of eosinophilia. Severe adverse effects of biologics are rare. The beneficial effects are greater for dupilumab than for omalizumab or mepolizumab, which may lead to its selection as the preferred biologic in CRSwNP; however, the effect sizes are similar enough that choosing omalizumab or mepolizumab is also reasonable. Selection of the biologic can also be driven by comorbid conditions, such as atopic dermatitis, chronic urticaria, or asthma. Dupilumab has concomitant approval for atopic dermatitis, omalizumab for chronic urticaria, and all 3 biologics are approved for asthma. Other biologics, such as benralizumab, reslizumab, and tezepelumab require additional research on their applicability in CRSwNP before any recommendations for their use can be made.
The conditional recommendation for biologics is driven by multiple factors, including the availability of other options that could be considered first or could be used together with biologics, such as INCSs, surgery, and ATAD (in patients with NERD). The patients who did not respond to treatment with INCSs or surgery, or those with very severe disease at baseline, may prefer biologics, whereas those who have not tried other treatments, have difficult access to biologics, or have lower overall disease burden may prefer to not use this class of drugs. Biologics may be preferred over ATAD in NERD, especially in patients with an increased risk of harm with ATAD.
The JTFPP GRADE guidelines for CRSwNP also discussed the applicability of ATAD in patients with NERD. It is frequently difficult to explain to patients how NSAIDs, which cause acute and distressing respiratory symptoms in patients with NERD, can be used as a long‑term therapy.15 However, ATAD is an important treatment option to consider in patients with NERD. In the JTFPP GRADE guidelines, ATAD was conditionally recommended, based on trials finding moderate‑certainty evidence for a treatment effect size closer to that seen for biologics than that observed for INCSs.10 ATAD improves disease‑specific QoL as measured on the SNOT‑22 scale by –10.61 points (95% CI, –14.51 to –6.71), as compared with placebo.16 It also improves nasal symptoms score as measured on a 0–10 scale by –2.74 points (95% CI, –3.92 to –1.57), as compared with placebo.16 Importantly, in the network meta‑analysis, the relative risk of having an adverse event associated with ATAD, as compared with placebo, was 3.84 (95% CI, 1.11–13.22). Appropriate patient selection is an important strategy to mitigate this risk.16 The most common adverse events are bleeding and gastritis. Advanced age, male sex, smoking, diabetes, hypertension, systemic corticosteroid (SCS) use, and lower weight or body mass index increase the risk of adverse effects above the baseline risk associated with aspirin use. The main factor driving the conditional recommendation for ATAD is the close balance of patient‑important benefits and harms. Potential topics for shared decision‑making (SDM) discussions include the risks during desensitization, such as poorly controlled asthma, and the risks associated with long‑term aspirin use.
Recent guidance on the management of chronic rhinosinusitis with nasal polyps in the context of other key management options
It is valuable to know that 2 other commonly selected CRS treatment options, that is, endoscopic sinus surgery (ESS) and SCSs, were not assessed in the JTFPP guidelines using the GRADE methodology. It is important to consider how and where these treatments fit in with the 3 treatments addressed in the JTFPP GRADE guidelines. First, a detailed consideration of the ESS techniques and evidence from relevant studies can be found in the EPOS2020 and ICAR‑RS guidelines.3,5 Second, there are limited trial data for ESS, at least partly due to challenges associated with conducting trials on surgical interventions. A recent trial comparing ESS combined with medical therapy and medical therapy alone found that ESS together with medical therapy were associated with slightly greater SNOT‑22 improvements (–4.9 points; 95% CI, –9.4 to –0.4).17 Finally, a large body of observational evidence reviewed in the EPOS2020 and ICAR‑RS guidelines supports the incorporation of ESS into algorithms for managing CRSwNP.3,5 A suggested approach that includes both ESS and SCSs is presented in Figure 3.
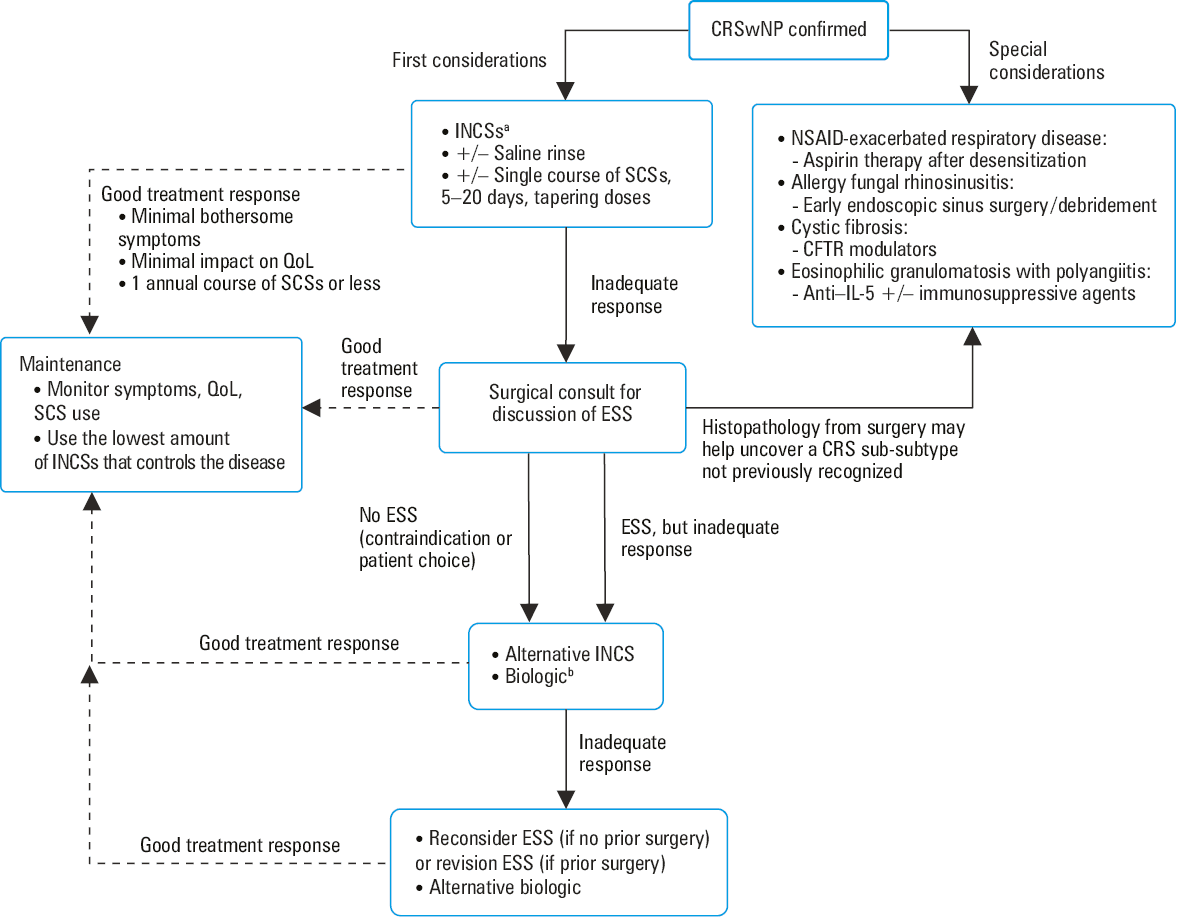
a INCS delivery methods with the best effectiveness and safety evidence are sprays, rinses, and exhalation delivery systems.
b Biologic drugs with the best effectiveness and safety evidence are dupilumab, mepolizumab, and omalizumab.
Abbreviations: CRSWnp, chronic rhinosinusitis with nasal polyps; CFTR, cystic fibrosis transmembrane conductance regulator; ESS, endoscopic sinus surgery; IL, interleukin; NSAID, nonsteroidal anti‑inflammatory drug; SCS, systemic corticosteroid; others, see Table 1
The other treatment option not directly assessed in the JTFPP GRADE guidelines for CRSwNP are SCSs. A meta‑analysis suggests that SCSs are effective in CRSwNP, with a treatment effect size larger than that of INCSs and similar to that of biologics.18 However, most experts discourage the use of SCSs, except in rare circumstances, due to the risk of adverse effects. SCS use can be considered in specific circumstances, such as severe exacerbation of the disease with major effects on patient QoL and / or an associated severe asthma exacerbation, in which case treatment with an oral SCS could be used for 5 to 20 days, often with tapering doses. The patients who require treatment with more than 1 SCS per year should be reassessed for other chronic treatment options with an overall goal of limiting SCS exposure to as low as possible.
The importance of shared decision‑making when using guidelines on the management of chronic rhinosinusitis with nasal polyps
All recommendations regarding treatment listed in the JTFPP GRADE guidelines for CRSwNP are conditional, which calls for SDM. A conditional recommendation means that most patients in a particular situation, having been fully informed, would want the suggested course of action, but many would not, and a discussion between the patient and their physician may help reach a decision.19,20 In this context, one of the roles of a clinician is also to help each patient make a decision regarding treatment that incorporates their values and preferences.
The factors that may be important for SDM with respect to each intervention were discussed earlier in this manuscript, and may serve as a starting point for the conversation. There are several excellent descriptions of effective SDM.19,20 Given how frequently guideline recommendations are conditional, it makes sense for health care professionals to become proficient in SDM.
Future directions
This review focused on treatment interventions for CRSwNP. The JTFPP GRADE guidelines for CRSwNP revealed some weaknesses in the evidence; thus, all of the recommendations were conditional. This means that additional research into these interventions could lead to a strong recommendation in favor in the future, but also to a suggestion or recommendation against. There are several unanswered questions regarding the role of other treatments for CRSwNP (most notably ESS and SCSs) and, importantly, how these treatments should be used in sequence or concomitantly. Head‑to‑head trials, trials on combined treatments, testing new treatments, development and validation of relevant decision aids, and cost‑effectiveness studies based on high‑certainty evidence are all warranted to improve CRSwNP management.
The JTFPP GRADE guidelines for CRSwNP did not address the management of CRSsNP, where the evidence for treatment methods is even more incomplete than in the case of CRSwNP. Trials involving patients with CRSsNP are highly needed to build the evidence base for future CRSsNP guidelines.
Summary
CRS is a common disease in adults. Careful diagnosis, including subtyping and applying clinical guideline treatment suggestions, are likely to improve disease‑specific QoL in many patients. In the management of CRSwNP, using SDM to consider INCSs, biologics, and ATAD (in patients with NERD) is the most recent guideline suggestion.
- Hastan D, Fokkens WJ, Bachert C, et al. Chronic rhinosinusitis in Europe – an underestimated disease. A GA2LEN study. Allergy. 2011; 66: 1216‑1223. | Crossref
- Sedaghat AR, Kuan EC, Scadding GK. Chronic rhinosinusitis: prevalence and risk factors. J Allergy Clin Immunol Pract. 2022; 10: 1395‑1403. | Crossref
- Orlandi RR, Kingdom TT, Smith TL, et al. International consensus statement on allergy and rhinology: rhinosinusitis 2021. Int Forum Allergy Rhinol. 2021; 11: 213‑739.
- Leung RM, Chandra RK, Kern RC, et al. Primary care and upfront computed tomography scanning in the diagnosis of chronic rhinosinusitis: a cost‑based decision analysis. Laryngoscope. 2014; 124: 12‑18. | Crossref
- Fokkens WJ, Lund VJ, Hopkins C, et al. Executive summary of EPOS 2020 including integrative care pathways. Rhinology. 2020; 58: 82‑111. | Crossref
ARTICLE INFORMATION