Are in-hospital mortality predictors based on complete blood count useful in patients with infective endocarditis? A retrospective tertiary center perspective (2015–2022)

 CC BY 4.0
CC BY 4.0
Are in-hospital mortality predictors based on complete blood count useful in patients with infective endocarditis? A retrospective tertiary center perspective (2015–2022)
Introduction
Infective endocarditis (IE) is a rare and life‑threatening disease with a mortality rate ranging from 18% to 25%.1,2 Numerous studies have reported a growing incidence of IE3 and an increase in the complexity of IE cases,4 but a decreasing mortality rate worldwide in recent decades.5 Consequently, novel outcome predictors in patients with IE are being extensively discussed. Researchers are exploring various markers and ratios based on standard laboratory tests, including complete blood count (CBC). Recent studies have shown utility of new outcome predictors, such as red blood cell distribution width (RDW) and neutrophil‑to‑lymphocyte ratio (NLR). In this study, we provide a retrospective, 8‑year experience of a tertiary center on the predictors of in‑hospital mortality derived from basic laboratory tests in patients with valve‑related IE (VRIE).
Patients and methods
Our tertiary center serves a stable population of 2.5 million citizens. We retrospectively selected all consecutive patients with VRIE hospitalized between January 1, 2015 and December 31, 2022 who qualified for conservative or surgical treatment. We analyzed the total number of cases and in‑hospital deaths, including pre- and perioperative deaths. In‑hospital preoperative death was defined as death occurring during hospitalization in the patients referred for conservative treatment, or death occurring before the procedure in those referred for surgical treatment. In‑hospital perioperative death was defined as death occurring during or after the surgical procedure. The technological and employee base of our facility remained comparable throughout the entire study period. We analyzed laboratory test results on admission (including CBC parameters, C‑reactive protein, procalcitonin, N‑terminal pro–B‑type natriuretic peptide [NT‑proBNP], estimated glomerular filtration rate [eGFR], creatinine, and urea) to identify predictors of in‑hospital death. The upper limit for NT‑proBNP in our laboratory changed over the years (2015–2017, 35 000 pg/ml; 2017–2022, 70 000 pg/ml). Therefore, in many patients, the levels of this parameter exceeded the upper limit. In such cases, values of 35 000 pg/ml or 70 000 pg/ml, as appropriate, were used for the analysis. Additionally, for RDW, NLR, and NT‑proBNP, we identified cutoff values associated with an increased risk of in‑hospital death and compared the predictive accuracy of these 3 parameters.
Statistical analysis
Statistical analysis was performed using Statistica 13.1 software (Tibco, Palo Alto, California, United States) and R version 4.2.1 (R Foundation for Statistical Computing, Vienna, Austria). Nominal variables are presented as numbers and percentages, or as median (range or interquartile range) and mean (SD), depending on the normality of their distribution. Univariable logistic regression analysis was used to assess the impact of specific factors on mortality, including overall, pre-, and perioperative mortality. Afterward, significant variables identified in the univariable analysis were included into the multivariable logistic regression model. To determine the optimal cutoff values predicting mortality (for RDW, NLR, and NT‑proBNP), we analyzed the area under the receiver operating characteristic (ROC) curve (AUC) and used the Youden index. The DeLong test was used to assess 95% CIs for AUCs. P values below 0.05 were considered significant.
Results
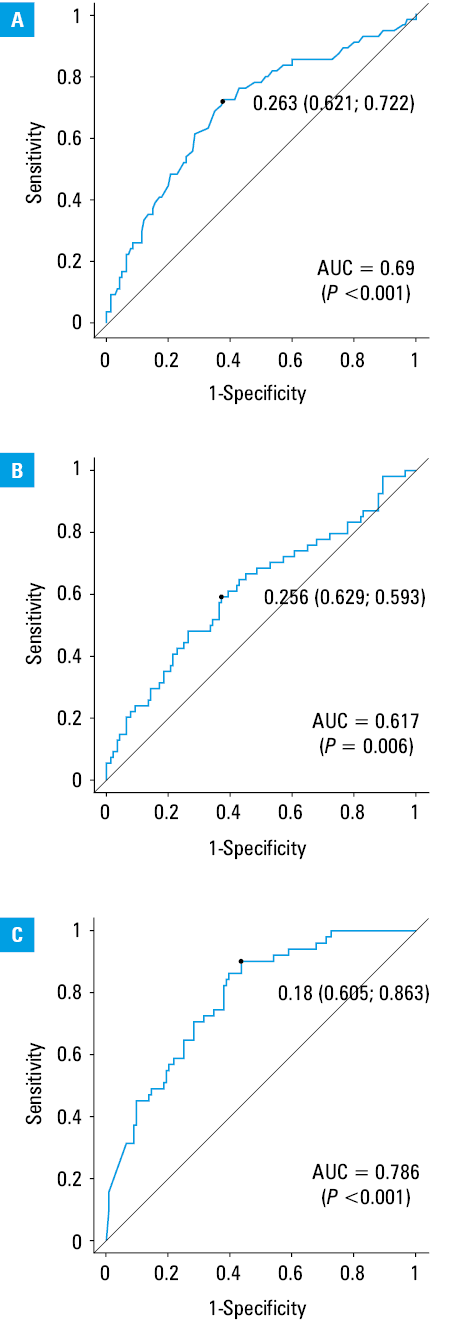
A total of 194 consecutive patients with confirmed VRIE were included in the study. The median (interquartile range) age of the patients was 62 (51–69) years, and the majority of them were men (75.3%). In the cases with a confirmed etiologic factor (n = 117), the most common causes of IE were Staphylococcus spp. (51.3%), Enterococcus spp. (22.2%), and Streptococcus spp. (15.4%). The most frequent IE types were left‑sided (92.3%) and native valve IE (72%). As many as 64.9% of the patients received surgical treatment. The overall mortality rate was 27.8% (Supplementary material, Table S1). Initially, due to a disturbing finding of a decreasing number of IE cases in our province (in opposition to global trends), we published the preliminary findings of our study as a short communication,6 which included an analysis of mortality, the number of IE cases diagnosed, basic clinical findings (such as IE location and etiology), and their impact on mortality. The results of laboratory tests on admission are presented in Supplementary material, Table S2. We found that most of the analyzed laboratory parameters were significantly associated with in‑hospital mortality (overall mortality: RDW, platelet count, hemoglobin, NLR, procalcitonin, NT‑proBNP, eGFR, creatinine, urea; preoperative mortality: lymphocyte count, RDW, platelet count, NLR, procalcitonin, NT‑proBNP, eGFR, creatinine, urea; perioperative mortality: RDW, NT‑proBNP, urea; Supplementary material, Table S3). However, the multivariable analysis revealed that only white blood cell count was an independent predictor of overall in‑hospital mortality (odds ratio, 1.46; 95% CI, 1.004–2.11; P = 0.048). ROC analysis was performed for 3 parameters (RWD, NRL, and NT‑proBNP), and each of them showed an acceptable AUC above 0.05 for overall mortality (RDW, AUC = 0.69; NLR, AUC = 0.62; NT‑proBNP, AUC = 0.79; Figure 1A–1C). The highest accuracy (based on AUC) for predicting in‑hospital mortality (overall, pre-, and perioperative death) was observed for NT‑proBNP, and it was the only parameter that showed significant results in all 3 mortality categories (Supplementary material, Table S4).
Discussion
Our study demonstrates that RDW, NLR, and NT‑proBNP can be useful in predicting in‑hospital mortality among patients with VRIE. RDW has been shown to be a prognostic indicator in a wide range of cardiac conditions, from coronary syndromes,7 throughout the spectrum of short-, medium-, and long‑term risk of death in patients with congestive heart failure [HF],8 up to IE. A study by Buburuz et al9 performed in a group of 126 patients showed that RDW was a good predictor of in‑hospital mortality with an AUC of 0.653, which is comparable to our observations.9 Similarly, Wei et al,10 based on data from 158 hospitalizations, found RDW to be an independent predictor of postoperative in‑hospital mortality, with an optimal cutoff value of 15.45%. Another study carried out in a group of 100 patients with IE also identified RDW as an independent predictor of 1‑year mortality (AUC = 0.7; cutoff value, 15.3%).11 Our analysis included a larger group of IE patients than the aforementioned studies, and although elevated RDW was not an independent predictor of death, the cutoff value was comparable. NLR has also proven to be useful in predicting in‑hospital complications of IE (AUC = 0.82; cutoff value, 7.1; n = 121).12 Moreover, it was associated with an increased risk of in‑hospital mortality (AUC = 0.729; cutoff value, 8.085; n = 142),13 and may be used for predicting the condition in patients with suspected IE.14 A summary of findings from all the aforementioned studies, as compared with our observations, is presented in Supplementary material, Table S5. It is worth mentioning that other variables derived from CBC also showed effectiveness in predicting mortality in IE patients. Zencir et al,15 in a group of 62 patients, identified a platelet‑to‑lymphocyte ratio as a predictor of in‑hospital mortality (AUC = 0.72; cutoff value, 191.01).15 There are also studies reporting a significant predictive value of a platelet‑to‑neutrophil ratio16 or a mean platelet volume‑to‑platelet count ratio17 in patients with IE.
Although our study and many other reports confirm the predictive value of CBC‑based ratios and parameters, we observed the highest AUC for NT‑proBNP. It is well known that the NT‑proBNP level not only reflects the clinical condition of a patient but also has a prognostic value. In patients with IE, NT‑proBNP serves as a predictor of in‑hospital mortality, as confirmed, for example, in studies by Bertolino et al18 (AUC = 0.744; cutoff value, 2926.5 pg/ml; n = 337) and Wei et al19 (AUC = 0.79; cutoff value, 2260 pg/ml; n = 703).19 Unfortunately, we did not find any previous studies with that would separately analyze pre- and perioperative in‑hospital mortality. In our study, the highest cutoff values for RDW, NLR, and NT‑proBNP were observed in the analysis of preoperative risk of death. This means that patients in a worse general clinical condition on admission are at a higher risk of preoperative death.
Elevated RDW and NLR are associated with an increased risk of in‑hospital death and may be useful in everyday clinical practice, as they can be easily derived from CBC. NT‑proBNP is also a routinely assessed laboratory parameter. It had the highest AUC in our study for predicting in‑hospital mortality, and is known to strongly correlate with the clinical condition of patients. Thus, based on our results, its predictive utility surpasses that of the CBC‑based parameters.
The pathophysiology of IE is complex, and involves a generalized septic / inflammatory state combined with HF in the vast majority of cases. HF is one of the most important complications in patients with IE. Decreased cardiac output due to damage to cardiac structures (mainly heart valves) caused by bacterial vegetations leads to volume overload, congestion, and, in general, acute decompensated HF (ADHF). As stated in the current European Society of Cardiology (ESC) guidelines,20 HF remains the most frequent complication and the main indication for cardiac surgery. Although NT‑proBNP levels are elevated in many clinical conditions (including inflammation), a greater increase in its concentration (higher specificity) is definitely observed in patients with HF/ADHF.
Confirming the utility of novel mortality risk predictors is important; however, we need to look not just for any but for the best markers we can use in everyday practice. Our study shows that the accuracy of NT‑proBNP is higher than that of the CBC‑based predictors, and additionally, NT‑proBNP reflects the clinical condition of each patient with HF (due to IE). Even though the CBC‑based predictors are useful, their clinical performance is worse than that of the great diagnostic and therapeutic response marker we already have—NT‑proBNP. IE is a complex disease requiring a comprehensive clinical approach. We propose a new perspective in the discussion on the outcome predictors in patients with IE. In our opinion, in comparison with NT‑proBNP, the CBC‑based parameters are generally less useful due to their lower accuracy and lower general clinical applicability. As indicated above, in comparison with NT‑proBNP, the CBC‑based markers seem less relevant in predicting the outcome of IE and IE‑related mortality. Our paper questions the other studies on CBC‑based factors and their predictive power, and addresses an essential doubt: are the novel CBC‑based factors better than what we already have? Our answer is “no.”
With the complexity of IE cases increasing every year, the overall risk assessment made by an experienced clinician based on the patient’s clinical condition and all necessary laboratory and imaging test results remains crucial. As stated in the current ESC guidelines,20 the prognosis assessment on admission in patients with IE should rely on simple biological, echocardiographic, and clinical parameters. None of the CBC‑based predictors were actually mentioned in these guidelines. This emphasizes that, though they are proven to be effective in risk assessment, their role in clinical practice is minimal. Based on our results, NT‑proBNP seems more accurate as a predictor of in‑hospital death in IE patients; additionally, it strongly corresponds with the clinical condition of individual patients. We must not lose sight of the whole picture by focusing solely on small details.
Limitations
The main limitation of this study is its retrospective design. Furthermore, the data on NT‑proBNP levels are not fully precise, as described in the Patients and methods section. Additionally, our study focused only on 2 (RDW, NLR) out of many potential predictors derived from CBC.
Conclusions
Predictors of in‑hospital mortality derived from CBC (such as RDW and NLR) can be useful in assessing the risk of in‑hospital death in patients with IE. However, NT‑proBNP appears to be a more accurate and stronger predictor of in‑hospital mortality that also reflects the clinical condition of patients. Although novel CBC‑based markers are effective in predicting in‑hospital mortality in patients with IE, their clinical usefulness remains worse than that of NT‑proBNP. Patients with IE present with a complex clinical picture that necessitates a comprehensive assessment of all clinical features by an experienced physician.
- Iung B, Duval X. Infective endocarditis: innovations in the management of an old disease. Nat Rev Cardiol. 2019; 16: 623‑635. | Crossref
- Cimmino G, Bottino R, Formisano T, et al. Current views on infective endocarditis: changing epidemiology, improving diagnostic tools and centering the patient for up‑to‑date management. Life (Basel). 2023; 13: 377. | Crossref
- Becher PM, Goßling A, Fluschnik N, et al. Temporal trends in incidence, patient characteristics, microbiology and in‑hospital mortality in patients with infective endocarditis: a contemporary analysis of 86,469 cases between 2007 and 2019. Clin Res Cardiol. 2022 Sep 12. [Epub ahead of print] | Crossref
- Ambrosioni J, Hernández‑Meneses M, Durante‑Mangoni E, et al. Epidemiological changes and improvement in outcomes of infective endocarditis in europe in the twenty‑first century: an International Collaboration on Endocarditis (ICE) prospective cohort study (2000‑2012). Infect Dis Ther. 2023; 12: 1083‑1101.
- Jensen AD, Østergaard L, Petersen JK, et al. Temporal trends of mortality in patients with infective endocarditis: a nationwide study. Eur Heart J Qual Care Clin Outcomes. 2022; 9: 24‑33. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION