Resistant hypertension: challenges in everyday practice
Key words: adherence, drug-related adverse events, renal denervation, resistant hypertension



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Resistant hypertension: challenges in everyday practice
Resistant hypertension is defined as not achieving sufficient control of blood pressure (BP), that is, maintaining BP values equal to or above 140/90 mm Hg when using 3 antihypertensive drugs, including diuretics, properly combined and at maximum doses. The uncontrolled treated hypertension should be confirmed in out‑of‑office BP measurements, preferably with 24‑hour ambulatory BP monitoring. Demographic and clinical characteristics indicate that patients with resistant hypertension are older than the general population of patients with arterial hypertension and more often suffer from comorbidities. When resistant hypertension is suspected, it is necessary to assess whether optimal pharmacotherapy has been prescribed, including appropriate combinations of antihypertensive drugs and diuretics at appropriate doses. It is also important to exclude parallel use of drugs that may have unfavorable interactions leading to an increase in BP. A common cause of pseudoresistant hypertension is a patient’s failure to comply with therapeutic recommendations, including a lack of lifestyle changes and nonadherence to the prescribed medication regimen. An important step in management of resistant hypertension is targeted screening with diagnostic tests for secondary hypertension. Expanding of the drug therapy beyond a 3‑drug regimen should include a mineralocorticoid receptor antagonist, in particular spironolactone. In selected patients, device‑based hypertension treatment might be considered.
Introduction
Arterial hypertension is one of the main modifiable risk factors for death worldwide. It is known that untreated hypertension leads to numerous cardiovascular complications, such as chronic coronary syndrome, heart attack and heart failure (HF), stroke, and kidney failure.1 In industrialized countries, over 30% of the adult population suffer from hypertension.2 In Poland, studies involving representative national samples and participants of a broad range of ages, reported that the prevalence of hypertension is between 29% and 46% in men and between 29% and 43% in women.3 To avoid complications of hypertension, systematic, long‑term treatment and achieving target blood pressure (BP) values are necessary. Unfortunately, in many patients, hypertension remains undiagnosed or, despite treatment, the patients do not achieve the recommended BP values. There are many reasons for this condition, and the important ones include insufficient cooperation of patients, limited access to medical care, or therapeutic inertia of health care workers. However, among patients treated for hypertension, there are also those who, despite following the recommendations and taking medications regularly, do not achieve good BP control. One of the reasons for such a condition is resistant hypertension.
Resistant hypertension is a relatively common clinical problem. Due to the changing definition, accurate data assessing the incidence of resistant hypertension are limited, with various research groups reporting the incidence in the range of 5% to 30% of patients with treated hypertension. The prevalence of resistant hypertension is difficult to quantify, because many factors differ among studies, including the population under study, antihypertensive pharmacotherapy used, varying approach to nonadherent patients, methods of BP measurement, and the definition of target BP.4 In a systematic review and meta‑analysis of 20 observational studies and 4 randomized controlled trials (RCTs), the prevalence ratios for resistant hypertension were 13.72% and 16.32%, respectively. Yet, most studies were incapable of ruling out pseudoresistance caused by the white‑coat effect, poor medication adherence, and suboptimal dosing.5 However, after exclusion of real causes of pseudoresistant hypertension, prevalence of resistant hypertension is probably around 5% of the treated patients.6 The estimates are much lower when resistant hypertension incidence is being analyzed. In a retrospective cohort study among patients with incident hypertension, 1.9% developed resistant hypertension within a median of 1.5 years from initial treatment.7
Currently, resistant hypertension is defined as not achieving sufficient control of BP, that is, maintaining BP values equal to or above 140/90 mm Hg when using 3 drugs (including a diuretic), properly combined and at maximum doses.8 Uncontrolled treated hypertension should be confirmed in out‑of‑office BP measurements, preferably with 24‑hour ambulatory BP monitoring (ABPM). Of importance, noncompliance with therapeutic recommendations must be excluded before diagnosing true resistant hypertension.8 According to the current definition,8 resistant hypertension should also be diagnosed in patients in whom normal BP control has already been achieved but with the use of 4 or more antihypertensive medications. A diagnosis of resistant hypertension is important to identify patients with difficult‑to‑treat hypertension. These individuals require additional diagnostic procedures and therapeutic treatments, as well as, in many cases, referrals to a specialized hypertension center.
Demographic and clinical characteristics indicate that patients with resistant hypertension are older than the general population of patients with arterial hypertension and more often suffer from comorbidities, such as chronic coronary syndrome, chronic heart and renal failure, atrial fibrillation, diabetes, potency disorders, stroke or an episode of transient ischemia of the central nervous system, and metabolic syndrome.9
Identification of patients with resistant hypertension within the general hypertensive population is extremely important due to a much higher risk of premature cardiovascular events in this group, as compared with individuals with appropriately controlled BP, as well as due to a higher risk of target organ complications (hypertension‑mediated organ damage [HMOD]).
The patients with resistant hypertension are more likely to experience vascular complications (including stroke) and HF exacerbations requiring hospitalization.10 In a large REACH (Reduction of Atherothrombosis for Continued Health) registry11 of patients with atherosclerosis, one of the largest contemporary outpatient registries initiated to evaluate patients who represent the entire spectrum of stable atherosclerotic clinical syndromes (from those with risk factors but asymptomatic to those with established atherosclerotic arterial disease within any circulatory bed), resistant hypertension was present in 12.7% of over 53 000 people with hypertension. After 4 years of follow‑up, a multivariate analysis showed that a composite end point (cardiovascular death, nonfatal stroke, and nonfatal myocardial infarction) occurred significantly more often in the group of patients with resistant hypertension than in those without this condition.11
Apparent resistant hypertension
Most cases of uncontrolled hypertension represent apparent resistant hypertension, that is, a situation in which uncontrolled hypertension does not result from actual resistance to pharmacotherapy. If resistant hypertension is suspected, such a diagnosis must first be confirmed by eliminating common causes leading to incorrect assessment of BP control, causing unnecessary intensification of treatment and putting a patient at risk of hypotension. In the case of discrepancies between the results of office and home BP measurements, the actual BP values should be confirmed, including assessment of the correctness of home BP measurements provided by the patient and exclusion of the white‑coat effect during office BP measurements. When verifying the diagnosis of resistant hypertension, it may be very helpful to utilize the 24‑hour ABPM method for out‑of‑office BP measurement, to eliminate possible bias caused by a medical environment or inappropriate home BP self‑measurement by a patient.
Possible causes of apparent resistant hypertension
Patient’s compliance with recommendations requires careful assessment of actual lifestyle modifications, such as weight reduction, regular physical activity, reducing alcohol and salt consumption, or smoking cessation. When resistant hypertension is suspected, it is necessary to assess whether optimal pharmacotherapy has been prescribed, including appropriate combinations of antihypertensive drugs and diuretics at appropriate doses. It is also important to exclude parallel use of drugs that may have unfavorable interactions leading to an increase in BP, for example, nonsteroidal anti‑inflammatory drugs or glucocorticosteroids.
Medication nonadherence as a cause of apparent resistant hypertension
Another common cause of pseudoresistant hypertension is the patient’s failure to comply with therapeutic recommendations. Analyses from clinical trials show that even over 40% of patients referred to the centers specializing in resistant hypertension did not take all recommended medications, and more than 10% of patients did not take any of the prescribed medications, as confirmed by the absence of their metabolites in laboratory tests.12 It is a well‑known fact that with an increase in the number of prescribed medications and greater complexity of the therapeutic regimen, the number of drug dose omissions by the patients increases. Improving cooperation on the patient side can be achieved by simplifying the therapeutic scheme and minimizing the number of prescribed Tablets (with the use of single‑pill combinations of antihypertensive drugs). The patients with resistant hypertension often require medications more than once a day, so it is important to consider their lifestyle and daily activities while proposing the drug dosage schedule.
To control whether a patient follows the therapeutic recommendations, many experts suggest reducing the time between follow‑up visits, prescribing drugs for a shorter period, asking the patients to bring empty drug packaging to the follow‑up visits, or using medication dispensers. The use of mobile applications can also be helpful in increasing patient’s engagement in the therapeutic process, by reminding of taking the medicines or providing BP measurement. An application can also require the patient to enter current BP value or obtain it via a wireless connection with a BP monitor, which later allows for creating various types of statistics.
Confirmation of adherence to antihypertensive medications may be provided by drug screening of urine or blood whenever available13 or by pharmacodynamic markers of exposure to medications (bradycardia on β-blockers, increased blood levels of uric acid on diuretics, increase in plasma renin concentration on diuretics or renin‑angiotensin system inhibitors).
One of the reasons for patient overt nonadherence to antihypertensive treatment might be unfavorable experience with various medications leading to adverse drug reactions (ADRs). In a group of 1000 hypertensive patients, in whom medical history of ADRs was assessed with a standardized questionnaire and confirmed in medical records, the prevalence of ever experiencing ADRs was 40.7% in men and 53.6% in women. The risk of experiencing ADRs increased significantly with longer duration of hypertension.14 Moreover, multiple drug intolerance syndrome, defined as experiencing side effects while taking 3 or more drug classes, occurred in 8% of hypertensive patients under study.15
Diagnostics workup
According to the 2023 European Society of Hypertension (ESH) guidelines, exclusion of pseudoresistant hypertension requires: 1) demonstration of an elevated ABPM; 2) exclusion that the BP elevation comes from inaccurate BP measurement, for example, a spurious BP increase associated with marked brachial artery calcification, especially in older patients or in patients with advanced chronic kidney disease (CKD); 3) exclusion of a secondary cause of hypertension or of poor adherence to the prescribed treatment regimen (Table 1).16 The prevalence of secondary hypertension, especially due to primary aldosteronism and atherosclerotic renal artery stenosis (particularly in older patients or patients with CKD) can be as high as 10%–20% of individuals with resistant hypertension.17 Screening for obstructive sleep apnea (OSA) (sleep history and specific tests) should not be omitted, because of frequent involvement of this condition in resistant hypertension, including night‑time hypertension.18 OSA is found in up to 83% of patients with resistant hypertension. Moreover, patients with resistant hypertension have a 2.5‑fold increased risk of OSA, as compared with other hypertensive patients.19 Fibromuscular dysplasia, which is no longer considered a rare cause of renovascular hypertension in young women, but rather appears as a systemic arterial disease in both sexes at any age and with a wide range of manifestations, should also be taken into account when searching for possible secondary causes of resistant hypertension.20
No. | Consideration | Practical approach |
Abbreviations: ABPM, ambulatory blood pressure monitoring; BP, blood pressure | ||
1. | Diagnose resistant hypertension | Office BP ≥140/90 mm Hg while on 3 antihypertensive medications, including a diuretic, at maximal doses |
2. | Exclude the white‑coat effect | Provide out‑of‑office BP measurement (ABPM), recommend and assess home BP measurements |
3. | Exclude apparent resistant hypertension | Collect in‑depth medical history, including information on lifestyle, sodium and alcohol intake, medication potentially increasing BP |
4. | Improve nonpharmacologic approach | Provide instruction concerning required lifestyle changes |
5. | Confirm medication adherence | Discuss with a patient their concerns toward medications |
6. | Consider undetected secondary hypertension as the cause of resistance to medications | Screening tests for secondary hypertension |
7. | Pharmacotherapy modifications | Dose adjustment, addition of spironolactone, loop diuretic, α- or β-blocker |
8. | Consult a hypertension specialist | Refer a patient to a tertiary hypertension clinic |
Identification of apparent resistant hypertension is important in preventing expensive, potentially risky diagnostics and avoiding unjustified intensification of treatment carrying the risk of side effects in the group of patients who do not suffer from true resistant hypertension. The incidence of true resistant hypertension may be lower than generally accepted.
Patients with true resistant hypertension are characterized by very high systolic BP and are often diagnosed with advanced target organ complications related to arterial hypertension.21 They are at a higher risk of HMOD,22 CKD,23 and premature cardiovascular events.24
The next stage of management for a patient with resistant hypertension is targeted screening with diagnostic tests for secondary hypertension. The authors of the updated ESH guidelines16 propose an approach with special attention to selected disease entities that may be responsible for secondary forms of hypertension. Particular emphasis is put on often accompanying signs and symptoms, including OSA (snoring, excessive daytime sleepiness), primary hyperaldosteronism (spontaneous hypokalemia, muscle weakness),25 CKD (creatinine clearance <30 ml/min), renal artery stenosis (female sex, young age or the presence of atherosclerosis in other locations, worsened kidney function),26 pheochromocytoma (paroxysmal hypertension, palpitations, headache), Cushing syndrome (moon face, central obesity, skin stretch marks), or coarctation of the aorta (pulse differences in the brachial and femoral artery, systolic murmur in the interscapular area).
Management of true resistant hypertension
Initiation of treatment of resistant hypertension is based on the introduction of the guideline‑recommended 3‑drug regimen, if it has not been used before. It should consist of a drug that inhibits the renin‑angiotensin‑aldosterone system (ie, angiotensin‑converting enzyme inhibitor or angiotensin receptor blocker), a thiazide or thiazide‑like diuretic, and a calcium antagonist (Figure 1). To improve medication adherence, the regimen should be administered at the maximum tolerated doses and in the form of single‑pill preparations. Introduction of these treatment principles in some patients with resistant hypertension already allows for achieving the correct level of BP control.
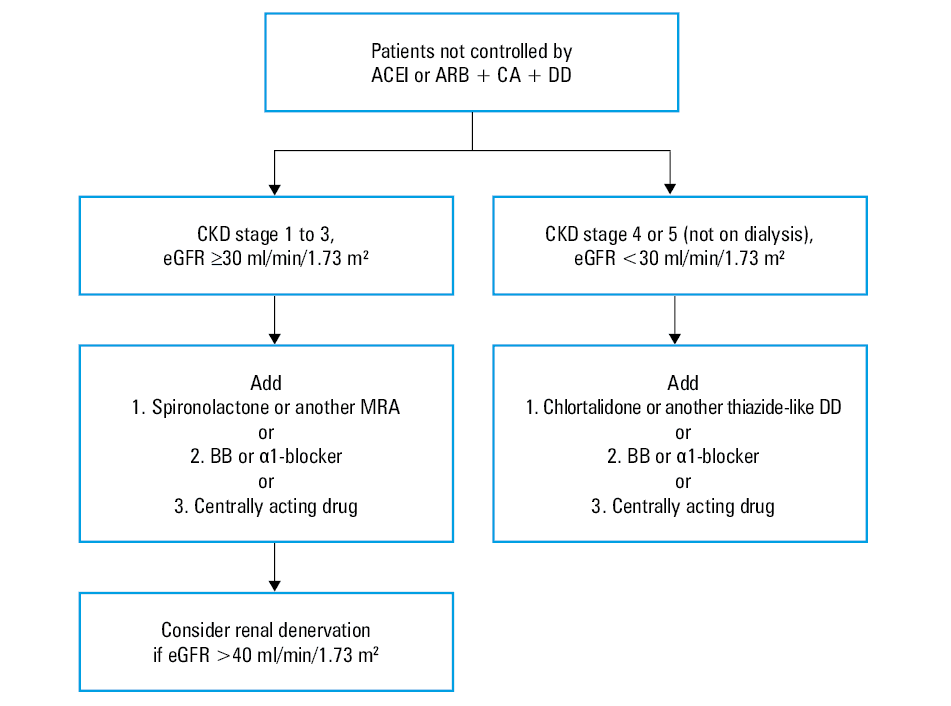
Abbreviations: ACEI, angiotensin‑converting enzyme inhibitor; ARB, angiotensin receptor blocker; BB, β-blocker; CA, calcium antagonist; CKD, chronic kidney disease; DD, diuretic; eGFR, estimated glomerular filtration rate; MRA, mineralocorticoid receptor antagonist
According to the recently published 2023 ESH guidelines16, as volume retention of multifactorial origin is frequent, reduced intake of sodium (<2 g/day) or NaCl (<5 g/day) and increased intensity of diuretic therapy, particularly in older patients, patients of Black African origin, or individuals with CKD, should be implemented. Dietary interventions are of particular importance, as adherence to dietary guidelines is low, even among patients with already established cardiovascular disease.27 If estimated glomerular filtration rate (eGFR) is above 30 ml/min/1.73 m2, BP control may be improved by increasing the dose of a current thiazide diuretic or by switching to a possibly more potent and longer‑acting thiazide‑like diuretic (indapamide or chlorthalidone). If eGFR is below 30 ml/min/1.73 m2, a loop diuretic (furosemide, bumetanide, or torsemide) should replace thiazide / thiazide‑like diuretics, although even then thiazides may retain their natriuretic and antihypertensive effects. In the CLICK (Chlorthalidone in Chronic Kidney Disease) trial,28 patients with stage 4 CKD (eGFR, 15–29 ml/min/1.73 m2) and poorly controlled hypertension, showed an about 10 mm Hg 24‑hour systolic BP reduction with chlortalidone vs placebo, and the antihypertensive effect was particularly evident in patients already on loop diuretics. Furosemide and bumetanide should be administered twice daily, because of their short duration of action, whereas longer‑acting agents, such as torsemide, can be administered once daily.29
The next step in expanding the drug therapy is supplementing the above 3‑drug regimen with a mineralocorticoid receptor antagonist (MRA), in particular spironolactone. The results of the PATHWAY‑2 (Prevention and Treatment of Hypertension with Algorithm based Therapy)30 study showed that supplementing the basic triple therapy with a fourth drug, spironolactone, even at a low dose (25–50 mg daily), was associated with a stronger BP‑lowering effect as compared with bisoprolol or doxazosin.
The ReHOT (Resistant Hypertension Optimal Treatment)31 study compared the hypotensive effect of spironolactone and clonidine. Although the results regarding the percentage of patients achieving proper BP control confirmed by ABPM and office BP measurement were similar in both groups, the patients taking spironolactone achieved slightly lower values of systolic and diastolic BP during 24 hours, and diastolic BP during the day. In view of the above observations, spironolactone should be added to the existing first‑line treatment in patients with resistant hypertension.
One should keep in mind possible antiandrogenic effects of spironolactone, that is, tenderness of the mammary glands and gynecomastia (in approximately 6% of men), menstruation disorders in women, or impotence in men. Spironolactone can be used effectively and safely to treat resistant hypertension in patients without significant renal dysfunction (eGFR ≥45 ml/min/1.73 m2 and serum potassium concentration ≤4.5 mmol/l). It is necessary to control electrolyte and creatinine concentrations shortly after the therapy initiation. If the laboratory test results are within the normal range, further checks should be performed at least once a year. If antiandrogenic side effects occur, an alternative may be to use another antagonist of mineralocorticoid receptors, that is, eplerenone at 50–100 mg daily. In selected cases, also amiloride, a potassium‑sparing diuretic, sodium channel blocker on the luminal surface of the distal tubule of the nephron, may prove effective at a dose of 5–10 mg per day.
Resistant hypertension is often associated with increased aldosterone concentration as a result undiagnosed primary hyperaldosteronism or increased aldosterone secretion after its initial reduction caused by blockage of the renin‑angiotensin‑aldosterone system. Therefore, reduced stimulation of the mineralocorticoid receptors by increased aldosterone concentration, as a result of treatment with MRAs, is highly effective in lowering BP in this group of patients.32 A new, more selective nonsteroidal MRA, finerenone, approved for the treatment in diabetic kidney disease might provide future alternatives to spironolactone for patients with resistant hypertension.33
If target BP is not achieved when applying the procedures described above, or if there are contraindications to MRAs, a loop diuretic (torasemide) should be initiated, as an addition to a thiazide / thiazide‑like diuretic. In patients with significantly reduced kidney function (eGFR <30 ml/min/1.73 m2), a loop diuretic should be used instead of a thiazide / thiazide‑like diuretic. Regular follow‑up of serum electrolyte (potassium, magnesium) concentrations is recommended, aiming at their effective supplementation.
The next stage of antihypertensive treatment intensification is the use of an α1‑blocker (doxazosin at 4–8 mg daily with modified release) or a β-blocker (bisoprolol at 5–10 mg daily). Effectiveness of these drugs in resistant hypertension was confirmed in the PATHWAY‑2 study,34 in which bisoprolol and doxazosin, used separately as add‑on treatments, resulted in smaller reductions in BP as compared with spironolactone. However, this reduction in BP was significant when compared with the patients receiving placebo. Therefore, the use of bisoprolol or doxazosin is justified in the case of spironolactone intolerance or any contraindications to its use. Optionally, another cardioselective β-blocker with vasodilating properties can be considered, for example, nebivolol at a dose of 10 mg daily.
In rare cases of resistant hypertension, older‑generation drugs may be effective, for example, centrally acting ones, such as clonidine, or directly dilating arterioles, such as dihydralazine. New antihypertensive drugs based on various mechanisms of action (aldosterone synthase inhibitors, vasopressin antagonists, nitric oxide donors, endothelin antagonists, or endopeptidase inhibitors [neprilysin]) are still under study.
Moreover, the complex pharmacotherapy of resistant hypertension very often requires dosing the medications at least 2 times a day, and taking into account the duration of action of individual preparations when determining the dosage regimen. An important information to determine the appropriate daily routine drug dosing is provided by the daily BP profile obtained with ABPM. In the group of patients with resistant hypertension, a frequently observed phenomenon is a lack of BP drop at night (nondipper BP profile), or even its increase during night hours (reverse‑dipper profile); such a situation requires higher doses of antihypertensive drugs in the afternoon.
In recent years, research has been continued on new drugs that can effectively lower BP in patients with resistant hypertension. These include drugs from the group of sodium‑glucose cotransporter 2 inhibitors (SGLT‑2is). A post hoc analysis of the EMPA‑REG Outcome study (Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients)35 showed that empagliflozin significantly reduced BP as compared with placebo in patients with presumed resistant hypertension. A selective aldosterone synthase inhibitor, baxdrostat, also seems to be a promising drug. In a recently published study,36 it reduced BP proportionally to its dose in patients with resistant hypertension, without showing any significant side effects. Research is ongoing also on an antagonist of endothelin (ET)-1 ETA and ETB receptors, aprocitentan. In preliminary studies in patients with resistant hypertension, aprocitentan was well tolerated and more effective than placebo in reducing BP at week 4, and the effect was maintained at week 40.37
Device‑based treatment of resistant hypertension
There has been a lot of research over the years into the techniques of invasive treatment of hypertension, however, currently no accepted technique has been developed as a standard of management in hypertension. Since not all patients with resistant hypertension can achieve BP control despite recommended pharmacotherapy, invasive treatment methods are sometimes used, for example, stimulation of carotid sinus baroreceptors, denervation of renal arteries, and surgical methods, such as removal of the carotid body and creation of an arteriovenous anastomosis.
Stimulation devices for carotid baroreceptors or the baroreceptor reflex enhancers are available to increase parasympathetic tone and inhibit sympathetic activity. Stimulation of the carotid sinus baroreceptors using a stimulator or a stent is intended to increase the tone of the carotid bulb and reflexively reduce sympathetic activation with a secondary reduction in arterial pressure.38 In the case of creating an iliac arteriovenous anastomosis, partial equalization of pressures between the arterial and venous systems is achieved with a reduction of systemic pressure.39
The best‑known technique for the invasive treatment of resistant hypertension is intravascular denervation of renal arteries, which involves bilateral damage to the sympathetic afferent and efferent fibers during a point application of energy with an intravascular catheter or highly‑concentrated ultrasound energy or perivascular injection of alcohol. Damage to the efferent fibers results in vasodilation of the renal vessels, increased renal blood flow and glomerular filtration, decreased tubular reabsorption of sodium and water, and decreased renal secretion of renin and noradrenaline.40 Data confirming the hypotensive effect of renal denervation are divergent, but more and more results from formerly conducted studies (DENERHTN,41 RADIANCE‑HTN SOLO,42 SPYRAL HTN‑ON MED43) indicate effective antihypertensive action of this method in combination with appropriate pharmacotherapy. In the EnCoRed (European Network Coordinating research on Renal Denervation) study,44 renal denervation was associated with a decrease in BP variability independent of the BP level, suggesting that responders may derive benefits from the reduction in BP variability as well.
Recent RCTs have shown that endovascular renal denervation can be associated with a significant, albeit not marked, office and ambulatory BP reduction in patients with uncontrolled hypertension.45 In a large registry of renal denervated patients, the BP reduction was long‑lasting and safety was considerably high.46 Renal denervation can thus be proposed as an adjunctive therapy to patients with resistant hypertension and eGFR above 40 ml/min/1.73m2, in whom BP control cannot be achieved or serious side effects cannot be avoided with antihypertensive medications.47
Treatment of resistant hypertension includes frequent comorbidities, for which additional treatment options may apply. For patients with OSA, continuous positive airway pressure (CPAP) may provide some benefits,48 especially when this condition is severe, baseline BP is high, and adherence to CPAP is good.49 In patients with obesity, glucagon‑like peptide‑1 receptor agonists can reduce body weight,50 modestly lower BP,51 and improve cardiovascular prognosis in individuals with type 2 diabetes or with established cardiovascular disease.52 Bariatric surgery can lower BP, cardiovascular risk factors, and risk of cardiovascular events in severely obese patients,53 and may reduce the burden of antihypertensive medication when these patients have resistant hypertension.54 In patients eligible for treatment with SGLT‑2is, their use may add a moderate BP‑lowering effect to the background antihypertensive therapy of resistant hypertension.55 Finally, when compared with valsartan alone, the sacubitril–valsartan combination reduced BP in patients with HF with preserved ejection fraction and resistant hypertension, despite treatment with at least 4 antihypertensive drugs.56 Given the association with multiple comorbidities and the need for multiple and complex drug therapeutic regimens, the ESH experts recommend to refer patients with resistant hypertension to a hypertension specialist or, if necessary, to a hypertension referral center.16 A dedicated tertiary hypertension clinic can be useful to perform the necessary diagnostic steps, optimize the multidrug treatment regimen, reduce the likelihood of drug‑related adverse effects, and increase adherence to treatment. Patients should receive a dedicated follow‑up program.
To summarize, resistant hypertension is a relatively common clinical scenario, although after excluding cases of apparent resistant hypertension, true resistant hypertension occurrs in only about 5% of hypertensive patients. Diagnostic workup should concentrate on the search for undetected forms of secondary hypertension. In‑depth medical history might help to stimulate lifestyle changes, improve treatment adherence, and provide management plan with adjustment of pharmacotherapy. In selected patients, device‑based hypertension treatment might be considered.
- Brouwers S, Sudano I, Kokubo Y, Sulaica EM. Arterial hypertension. Lancet. 2021; 398: 249‑261. | Crossref
- Mills KT, Stefanescu A, He J. The global epidemiology of hypertension. Nat Rev Nephrol. 2020; 16: 223‑237. | Crossref
- Pająk A, Jankowski P, Zdrojewski T. The burden of cardiovascular disease risk factors: a current problem. Kardiol Pol. 2022; 80: 5‑15. | Crossref
- Carey RM, Sakhuja S, Calhoun DA, et al. Prevalence of apparent treatment‑resistant hypertension in the United States. Hypertension. 2019; 73: 424‑431. | Crossref
- Achelrod D, Wenzel U, Frey S. Systematic review and meta‑analysis of the prevalence of resistant hypertension in treated hypertensive populations. Am J Hypertens. 2015; 28: 355‑361. | Crossref
ARTICLE INFORMATION