Infectious aneurysm: a rare form of intracranial aneurysm. Two cases with distinct clinical and imaging manifestations



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Infectious aneurysm: a rare form of intracranial aneurysm. Two cases with distinct clinical and imaging manifestations
Infectious intracranial aneurysms (IIAs) are rare complications of systemic infections that lead to microbial infiltration and degradation of a normal or extended arterial vessel wall.1 They represent 0.7% to 6.5% of all IAs.2 A majority of reported cases involve young or middle‑aged adults, with male predominance.1,3 The most common etiology of IIAs is septic embolization due to infectious endocarditis (IE).1,2 These aneurysms are often multiple and localized in distal parts of cerebral arteries, mainly the middle cerebral artery (MCA).1,3 Unruptured IIAs are usually asymptomatic. Larger aneurysms cause focal neurologic symptoms secondary to a mass effect or occlusion of the affected artery and ischemic stroke.1,3,4 Aneurysm rupture causes subarachnoid, cerebral, and intraventricular hemorrhages, with meningeal signs and neurologic deficits.1,2,4 Although brain computed tomography (CT) and CT angiography (CTA) as well as magnetic resonance imaging (MRI) and magnetic resonance angiography enable the diagnosis of IIAs, digital subtraction angiography (DSA) remains the gold‑standard diagnostic modality.2-4 We present 2 clinically distinct cases of IIAs resulting from left‑sided bacterial endocarditis.
Patient 1 was a 40‑year‑old cachectic woman with drug‑resistant catatonic schizophrenia. During electroshock therapy, she suddenly developed consciousness disturbances with fever, severe left‑sided hemiparesis, and meningeal signs, and was subsequently admitted to the neurology department. Neuroimaging demonstrated edema in the right cerebral hemisphere, with multiple hemorrhagic foci (Figure 1A–1C) and adjacent bleeding into the subarachnoid space (Figure 1A). Due to changes in cerebrospinal fluid (CSF; slightly elevated polynuclear cell count and protein levels) and suspected neuroinfection, empiric antibiotic treatment (ceftriaxone and vancomycin intravenously [IV]) was introduced. The diagnosis of IE was established based on the results of blood cultures (methicillin‑sensitive Staphylococcus aureus), CSF cultures (negative), and transesophageal echocardiography findings. After a week of guided antibiotic therapy (cloxacillin IV), the patient’s condition improved; she was conscious and logically responsive, and had moderate left‑sided hemiparesis. Follow‑up MRI revealed regression of the edema and presence of IIAs in the MCA branches unilaterally, best visible on susceptibility‑weighted imaging (SWI) (Figure 1D). After 6 weeks of guided antibiotic therapy and 2 months of hospitalization, the patient was discharged home with mild left‑sided hemiparesis.
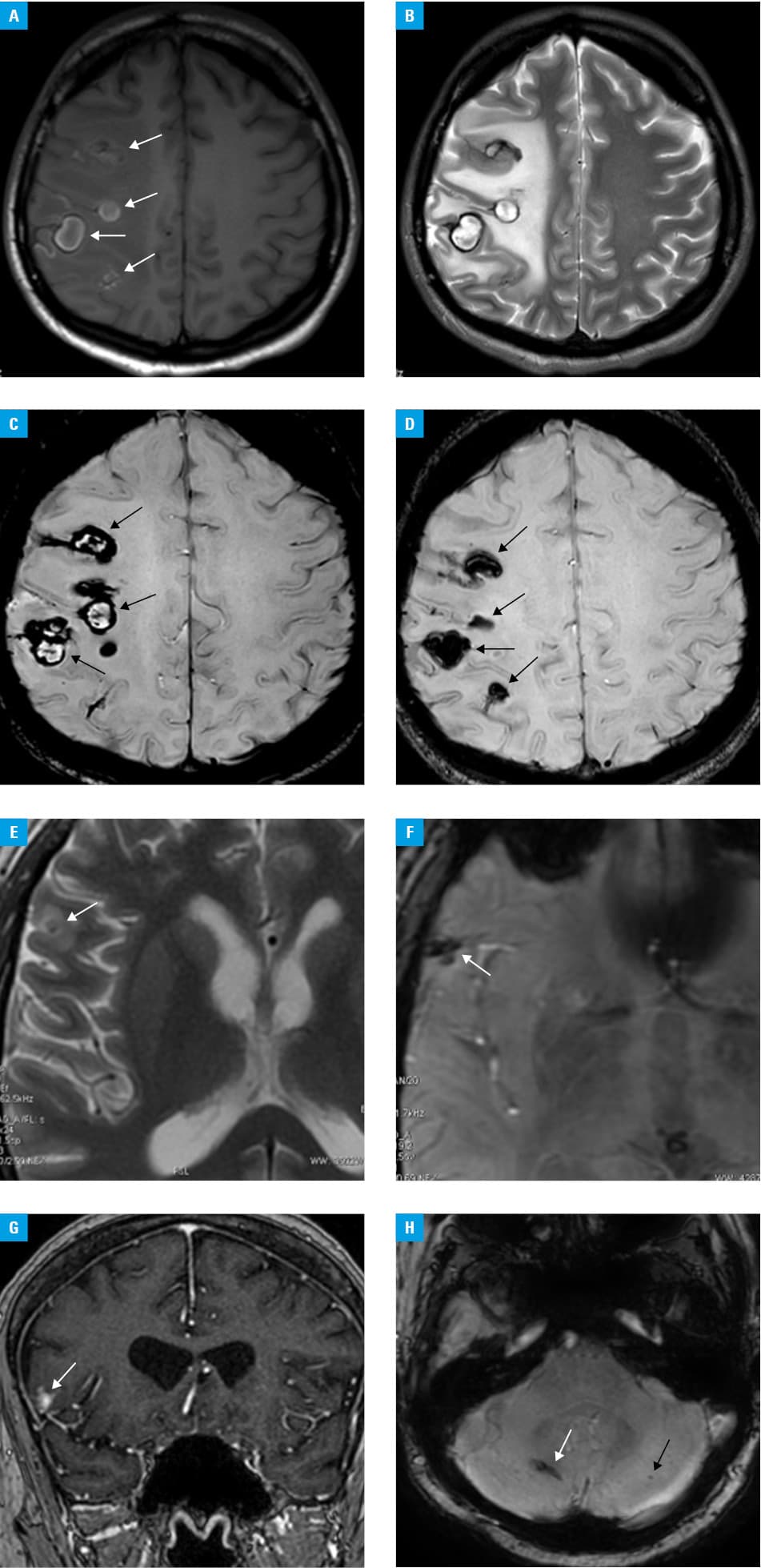
Patient 2 was a 50‑year‑old man with a mechanical ascending aortic prosthesis and a mechanical prosthetic valve implanted in the aortic position due to aortic dissection. He was admitted to a cardiology department due to recurrent fever and exertional dyspnea for several days. A diagnosis of IE was made based on transesophageal echocardiography findings, and empiric antibiotic treatment (gentamicin, ampicillin, and cloxacillin IV) was started. Blood cultures were positive for Enterobacter cloacae, and guided antibiotics (ceftriaxone and gentamicin IV) were introduced. The antibiotic therapy was complicated by splenic infarction and rupture of a splenic abscess requiring splenectomy. Simultaneously, the patient developed dizziness, with low‑amplitude nystagmus and mild left‑sided hemiparesis. Brain MRI demonstrated a single, small, clinically benign IIA in the right frontal lobe (Figure 1E–1G), and probably a second one in the right cerebellar hemisphere, visible only on the SWI sequence, with microbleeds in the cerebellum (Figure 1H). Due to the progression of IE and formation of an abscess in the mechanical prosthetic aortic valve, the patient underwent urgent cardiac surgery to insert a biological ascending aortic prosthesis and a bioprosthetic aortic valve. Six weeks of guided antibiotic treatment resulted in resolution of neurologic symptoms, and a follow‑up MRI examination (not shown) revealed regression of acute lesions; there was no edema or contrast enhancement. The patient was discharged home in a good general condition after 4 months of hospitalization.
Treatment of IIAs involves long‑term intravenous antibiotic therapy. Unruptured aneurysms can be managed conservatively.2,3 Neurosurgical or endovascular intervention should be considered in patients with ruptured aneurysms, or in those who do not respond to conservative treatment.1,3,4
Although the course of IIAs in the 2 presented patients was different, neither required further intervention following administration of guided antibiotics and supportive treatment, and good final outcomes were observed. IIAs should be considered as a possible cause of hemorrhagic lesions, not only in patients with diagnosed IE but also in those in whom hemorrhage is the first clinical manifestation of IE.5 We highlighted the potential role of MRI in the diagnosis of IIAs; in particular, SWI may be helpful in detection of low‑signal lesions not visible on other sequences. In certain cases, the use of MRI with the SWI sequence might prevent the need for superior modalities associated with radiation and iodine contrast exposure, such as CTA or invasive DSA.1,4,5
- Ducruet AF, Hickman ZL, Zacharia BE, et al. Intracranial infectious aneurysms: a comprehensive review. Neurosurg Rev. 2010; 33: 37‑46. | Crossref
- Kannoth S, Thomas SV. Intracranial microbial aneurysm (infectious aneurysm): current options for diagnosis and management. Neurocrit Care. 2009; 11: 120‑129. | Crossref
- Alawieh A, Chaudry MI, Turner RD et al. Infectious intracranial aneurysms: a systematic review of epidemiology, management, and outcomes. J Neurointerv Surg. 2018; 10: 708‑716. | Crossref
- Delgado V, Ajmone Marsan N, De Waha S, et al. 2023 ESC Guidelines for the management of endocarditis. Eur Heart J. 2023; 44: 3948‑4042.
- Williams TJ, Starr M, El‑Dalati S. Intracranial hemorrhage as a marker for mycotic aneurysm in patients with infective endocarditis. Neurol Clin Pract. 2023; 13: e200144. | Crossref
ARTICLE INFORMATION