Healthy vaccinee effect: a bias not to be forgotten in observational studies on COVID-19 vaccine effectiveness


 CC BY 4.0
CC BY 4.0
Healthy vaccinee effect: a bias not to be forgotten in observational studies on COVID-19 vaccine effectiveness
To the editor
We have followed with interest the enriching discussion opened by Prof. Zagożdżon1 and Dr. Jarynowski2 regarding biases in observational studies on the effectiveness of COVID‑19 vaccines, inspired by an interesting study by Pietrzak et al.3 We agree that these biases are rarely sufficiently accounted for. There is, however, another type of bias that is even more rarely mentioned in such studies—the so‑called healthy vaccinee effect, as recently suggested by Hoeg et al.4 It refers to a situation in which the population opting for vaccination is generally healthier than the population opting out of vaccination. Here, we would like to illustrate this effect using data from a population that is genetically, culturally, and geographically very close to the Polish one—the Czech population.
In general, most studies on COVID‑19 vaccines, including that by Pietrzak et al,3 assume the same fragility among the vaccinated and unvaccinated groups. In other words, such observational studies are based on the assumption that individuals in the vaccinated group would be subject to the same risk of dying as the unvaccinated population, if they remained unvaccinated. Here, we would like to present our analysis of data from the General Health Insurance Company of the Czech Republic, which proves that this baseline likelihood of dying greatly differs between these groups.
The state‑owned General Health Insurance Company is the largest health insurance / health care services payer in the Czech Republic (health insurance is mandatory). It covers almost 60% of the Czech population. The company kindly responded to our request submitted according to the Czech version of the Freedom of Information Act, and provided cumulative data on all deaths (ie, all‑cause deaths) among its vaccinated and unvaccinated policyholders between January and September 2021, categorized by months and decades of age.5 As this insurance company has a disproportionately large share of elderly policyholders, the data provided covered 72% of all deaths in the Czech Republic over the analyzed period.
For each month and each age category, we obtained a total number of vaccinated and unvaccinated policyholders as well as the total number of deceased policyholders in these groups. We further classified the data according to the epidemiological situation into the high‑COVID (January–March 2021) and low‑COVID (July–September 2021) periods. Overall, approximately 15 000 individuals (out of 47 100 all‑cause deaths) died with a positive result of the polymerase chain reaction test during the high‑COVID period, while only 160 (out of 28 200 all‑cause deaths) died during the low‑COVID period.6,7
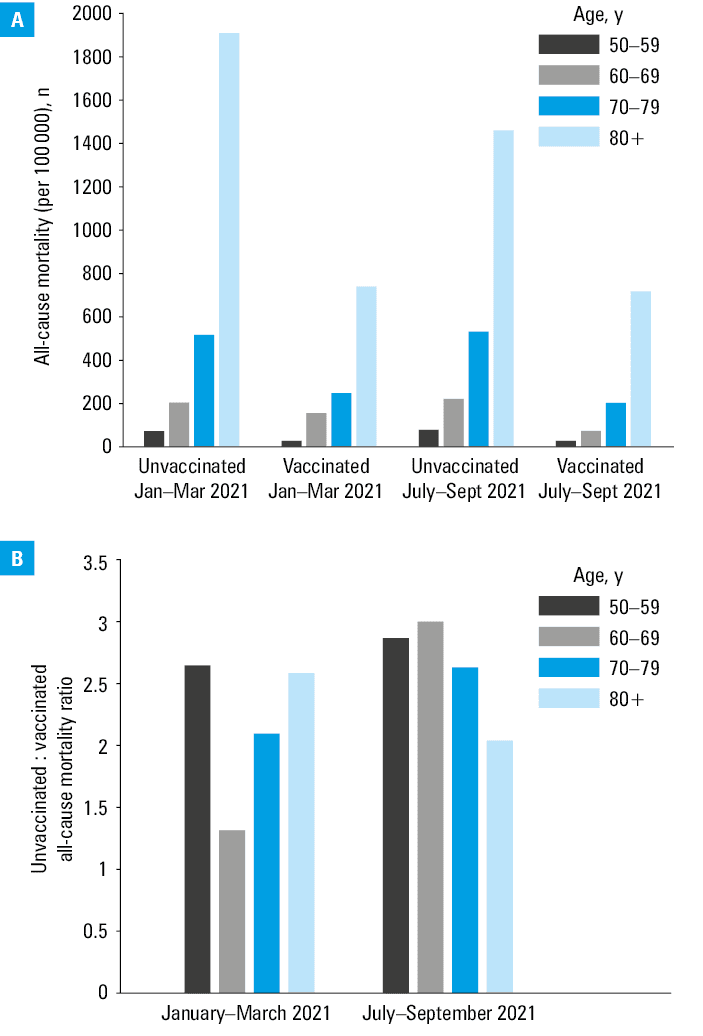
A comparison of all‑cause death rates among vaccinated and unvaccinated persons in individual age groups normalized per 100 000 population is presented in Figure 1A. Due to the small number of deaths in younger age groups, the mortality rates are only shown for individuals aged 50 years and older. As expected, in all age groups, the mortality in the unvaccinated population consistently exceeded that observed in the vaccinated population. This is, of course, not surprising in the high‑COVID period; however, the same pattern can be seen during the low‑COVID period, when almost no deaths of SARS‑CoV‑2–positive patients were registered in the Czech Republic. Figure 1B conveys the same message, showing the ratios of the unvaccinated to the vaccinated individuals. These data clearly indicate that all‑cause mortality in the unvaccinated population was generally approximately 2 to 3 times higher than in the vaccinated population in the respective age groups, during both low‑COVID and high‑COVID periods. Using the approach adopted in most observational studies, including that by Pietrzak et al,3 this would mean that vaccination was associated with approximately 50% lower risk of all‑cause death, even in the periods with almost no COVID‑19–related deaths. As it is impossible that COVID‑19 vaccines would have prevented all‑cause deaths in a period when there had been virtually no COVID‑19–related deaths, we must consider the healthy vaccinee effect as an alternative explanation. We can speculate about the reasons for this phenomenon. The most plausible ones are behavioral—it is likely that people who get vaccinated generally take better care of their health. On the other hand, the most fragile people, in terminal stages of their diseases, most probably chose not to be vaccinated. Alternative / additional explanations may include more difficult access to health care services for the unvaccinated individuals in that period, or health deterioration following previous SARS‑CoV‑2 infection, which was more likely in the unvaccinated group. Regardless of the reason, these data disprove the principal assumption of practically all observational studies that both groups are at the same risk of dying from COVID‑19 before vaccination. As individuals in the unvaccinated group are generally more fragile (ie, have a much higher likelihood of dying from any cause) than those in the vaccinated group, they will also be more susceptible to dying from COVID‑19.
To further strengthen our case, we would like to point to another Central European (Hungarian) study by Pálinkás and Sándor.8 In that study, the reported effectiveness of COVID‑19 vaccines against all‑cause mortality was approximately 50%, and the authors attempted to quantify the healthy vaccinee effect. We are not sure whether such a direct recalculation is possible; however, we feel the need to point this out as a caveat to the simplistic interpretation of observational studies. So far, it appears that this effect might be consistent, at least among the postcommunist countries of the Central Europe, and it might be interesting to conduct a similar analysis also for Poland. It is likely that Pietrzak et al3 are already in possession of relevant data.
- Zagożdżon P. Bias in data analysis of the study “Effectiveness of the BNT162b2 vaccine in preventing COVID‑19–associated deaths in Poland.” Pol Arch Intern Med. 2023; 133: 16573. | Crossref
- Jarynowski A. Effectiveness of the BNT162b2 (COMIRNATY) vaccination in protecting from death due to COVID‑19 in Poland: epidemiologic commentary and limitations. Pol Arch Intern Med. 2023; 133: 16574. | Crossref
- Pietrzak Ł, Polok K, Halik R, et al. Effectiveness of the BNT162b2 vaccine in preventing COVID‑19–associated deaths in Poland. Pol Arch Intern Med. 2023; 133: 16453. | Crossref
- Høeg TB, Duriseti R, Prasad V. Potential “healthy vaccinee bias” in a study of BNT162b2 vaccine against Covid‑19. N Engl J Med. 2023; 389: 284‑286. | Crossref
- General Health Insurance Company of the Czech Republic. Information provided upon request pursuant to Act no. 106/1999 Coll [in Czech]. https://www.vzp.cz/o‑nas/informace/odpovedi‑na‑zadosti‑o‑informace/zadost‑ze‑dne‑14‑11‑2021. Accessed March 25, 2023.
ARTICLE INFORMATION