Possible association between β-blocker use and a risk of intracranial aneurysm rupture
Key words: β-blockers, intracranial aneurysm, subarachnoid hemorrhage

 CC BY 4.0
CC BY 4.0
Possible association between β-blocker use and a risk of intracranial aneurysm rupture
Introduction: Aneurysmal subarachnoid hemorrhage is a devastating type of stroke, associated with high mortality and morbidity. One of modifiable risk factors of aneurysm rupture is hypertension, however, it is still not clear whether any particular antihypertensive drugs play a significant role in the prevention of aneurysm rupture.
Objectives: We decided to investigate whether there is any association between acetylsalicylic acid, α-blockers, β-blockers, angiotensin‑converting enzyme inhibitors, angiotensin II receptor blockers, calcium channel blockers, diuretics, statins, and anticoagulants and a risk of intracranial aneurysm rupture.
Patients and methods: We retrospectively analyzed 334 patients with ruptured and unruptured intracranial aneurysm. Based on logistic regression models, we obtained unadjusted and adjusted odds ratios (ORs) of subarachnoid hemorrhage associated with the use of vasoactive medications and with indices of tortuosity.
Results: We found that β-blocker intake was significantly related to higher tortuosity of the cerebral arteries. Also, the intake of β-blockers (OR, 0.41; 95% CI, 0.21–0.77; P = 0.01) and statins (OR, 0.23; 95% CI, 0.05–0.68; P = 0.01) significantly decreased the risk of aneurysm rupture, a result driven by a decreased rupture risk of anterior circulation aneurysms. No such association was found for the posterior part of the cerebral circulation.
Conclusions: Aneurysm located in the anterior cerebral circulation might be less likely to rupture if patients receive β-blockers or statins.
What's new?
β-Blockers are no longer the first‑line drugs in antihypertensive therapy. However, they are still indicated in patients with myocardial infarction, heart failure, or aortic aneurysms. Our data may support the notion that β-blockers and statins should be used in patients with unruptured intracranial aneurysms, and possibly in hypertensive patients at a high risk of having an asymptomatic aneurysm, such as patients with strong family history of aneurysms and subarachnoid hemorrhage. However, independent confirmation of our results is needed before any such recommendations are made.
Introduction
Subarachnoid hemorrhage (SAH) is a devastating type of stroke, with incidence in the general population of about 11 per 100 000.1 It is associated with a 30%–40% mortality rate and poor treatment outcome in about 50% of survivors.2,3 In approximately 85% of the cases, SAH is caused by intracranial aneurysm rupture.4 It is recommended that the unruptured intracranial aneurysms are treated by surgical or endovascular intervention.5 However, such treatment may in some patients be impossible due to various reasons. There are also groups of individuals, potentially burdened with a higher risk of hosting an aneurysm due to family history, hypertension, or both, in whom screening computed tomography (CT) is not always possible, and who might benefit from pharmacological therapy. Currently, the only recommendations for patients with conservatively managed intracranial aneurysms are routine imaging controls, such as computed tomography, angriography, and magnetic resonance angiography and minimization of rupture risk factors.6 Few groups of medications, such as statins,7 acetylsalicylic acid,8 or anticoagulants were analyzed in SAH prevention, however, their impact on the risk of aneurysm rupture remains inconclusive.6,9
As hypertension is one of the most important modifiable risk factors of SAH, it was suggested that antihypertensive drug intake might prevent intracranial aneurysm rupture.10 However, to the best of our knowledge, there are no studies showing any positive influence of these drugs on the risk of SAH. Therefore, we decided to investigate whether there is an association between the use of antihypertensive drugs, statins, and acetylosalicic acid and a risk of intracranial aneurysm rupture.
Patients and methods
Patients
We retrospectively analyzed 334 patients with intracranial aneurysm confirmed by digital subtraction angiography. The patients included in the study group were individuals with either ruptured intracranial aneurysm or aneurysm diagnosed as an incidental finding, and qualified for planned treatment. The patients were hospitalized between January 2013 and June 2018 at the Department of Neurosurgery and Neurotraumatology, Jagiellonian University Medical College, and University Hospital, Kraków, Poland. We included the patients with aneurysms located in the anterior cerebral artery (ACA), anterior communicating artery (ACoA), middle cerebral artery (MCA), internal carotid artery (ICA), and basilar artery (BA). We excluded the patients with a history of SAH, previous neurosurgical or intracranial endovascular interventions, or diagnosed with a connective tissue disorder. The presence of SAH was assessed based on CT. Data on medication use and the presence of hypertension, diabetes mellitus, smoking, and dyslipidemia were obtained from the patients’ medical records. As acute headache, especially when associated with SAH, affects blood pressure, we did not use blood pressure values in the subsequent analyses. The methodology of tortuosity measurements is described in Supplementary material. The study protocol was approved by the Jagiellonian University Bioethics Committee (1072.6120.312.2018). All patients gave their informed consent at the time of hospitalization. All procedures involving human participants were in accordance with ethical standards of the institutional research committee.
Statistical analysis
Database management and statistical analysis were conducted with RStudio package, version 8.5 for Windows (RStudio Inc., Auckland, New Zealand).
We used the Shapiro–Wilk test to assess normality of data distribution. We compared normally distributed continuous variables with the t test, and used the Mann–Whitney test for non‑normally distributed variables. We used the χ2 test for comparisons of dichotomized variables. To assess possible influence of risk factors and medications on the presence of ruptured aneurysm, we fitted univariable and multivariable logistic regression models. In all adjusted models, hypertension, diabetes mellitus, smoking, hypercholesterolemia, sex, and age were used as confounders. We additionally adjusted the analysis for other medications. The analyses accounted for the use of acetylsalicylic acid, α-blockers, β-blockers, angiotensin‑converting enzyme inhibitors (ACEIs), angiotensin II receptor blockers (ARBs), calcium channel blockers, diuretics, statins, and anticoagulants. All tests were 2‑tailed, and the P value below 0.05 was considered significant.
Results
Study group characteristics
Mean (SD) age of 334 patients (68.56% women) was 57.9 (12.6) years. A total of 105 patients (31.4%) had ruptured aneurysm. The most common location of the aneurysm was ICA (40.1%), then ACA (31.1%), BA (18%), and MCA (10.8%). As many as 190 patients (56.9%) had cardiovascular diseases and 181 (54.2%) took antihypertensive medications. The characteristics of the study group are presented in Table 1.
Variable | All patients (n = 334) | Ruptured aneurysm (n = 105) | Unruptured aneurysm (n = 229) | P value |
Data are presented as number (percentage) or median (interquartile range) unless indicated otherwise.
Abbreviations: ACEIs, angiotensin‑converting enzyme inhibitors; ARBs, angiotensin II receptor blockers | ||||
Risk factors | ||||
Female sex | 229 (68.56) | 64 (60.95) | 165 (72.05) | 0.04 |
Age, y, mean (SD) | 57.91 (12.6) | 58.30 (12.53) | 56.82 (13.92) | 0.35 |
Hypertension | 142 (42.51) | 43 (40.95) | 99 (43.23) | 0.7 |
Diabetes mellitus | 39 (11.68) | 5 (4.76) | 34 (14.85) | 0.01 |
Smoking | 74 (22.16) | 22 (20.95) | 52 (22.71) | 0.72 |
Dyslipidemia | 55 (16.47) | 8 (7.62) | 47 (20.52) | <0.001 |
Aneurysm size, mm | 5.12 (3.82–7.15) | 6.84 (4.39–8.43) | 5.35 (4.02–7.55) | 0.02 |
Aneurysm location | ||||
Anterior communicating artery | 104 (31.14) | 49 (46.67) | 55 (24.02) | <0.001 |
Middle cerebral artery | 134 (40.12) | 3 (2.86) | 33 (14.41) | <0.001 |
Internal carotid artery | 36 (10.78) | 22 (20.95) | 112 (48.91) | <0.001 |
Basilar artery | 60 (17.96) | 31 (29.52) | 29 (12.66) | <0.001 |
Drug intake | ||||
Acetylsalicylic acid | 102 (30.54) | 22 (20.95) | 80 (34.93) | 0.01 |
α-Blockers | 22 (6.59) | 5 (4.76) | 17 (7.42) | 0.36 |
β-Blockers | 111 (33.23) | 22 (20.95) | 89 (38.86) | 0.001 |
ACEIs | 93 (27.84) | 23 (21.9) | 70 (30.57) | 0.1 |
ARBs | 25 (7.49) | 6 (5.71) | 19 (8.3) | 0.41 |
Calcium channel blockers | 52 (15.57) | 15 (14.29) | 37 (16.16) | 0.66 |
Diuretics | 70 (20.96) | 16 (15.24) | 54 (23.58) | 0.08 |
Statins | 58 (17.37) | 6 (5.71) | 52 (22.71) | <0.001 |
Anticoagulants | 20 (5.99) | 4 (3.81) | 16 (6.99) | 0.26 |
Risk factors for aneurysm rupture
Women more often than men had ruptured aneurysm. Patients with diabetes mellitus (4.8% vs 14.9%; P = 0.01) and dyslipidemia (7.6% vs 20.5%; P <0.001) significantly less often had ruptured aneurysm. In terms of the aneurysm location, ACoA (46.7% vs 24%; P <0.001) and BA (P <0.001) aneurysms were significantly more likely to rupture, and MCA (2.9% vs 14.4%; P <0.001) and ICA (21% vs 48.9%; P <0.001) aneurysms were significantly less likely to rupture. The patients with ruptured aneurysms also had lower tortuosity in terms of all analyzed descriptors: relative (SD) length was 5.3 (2.1) mm and 5.9 (2.1) mm for unruptured and ruptured aneurysms, respectively, P = 0.01; sum of angle metrics was 3.5 (1.9) and 2.6 (1.6); P <0.001; product of angle distance was 3.2 (1.9) and 2.6 (1.7); P = 0.006; triangular index was 3.8 (1.9) and 3.1 (1.9); P = 0.002; and inflection count metric reached 2.7 (1.9) vs 1.7 (1.6); P <0.001. In a multivariable analysis, male sex (odds ratio [OR], 0.56; 95% CI, 0.33–0.95; P = 0.01), diabetes mellitus (OR, 0.29; 95% CI, 0.09–0.77; P = 0.02), and dyslipidemia (OR, 0.28; 95% CI, 0.11–0.64; P = 0.02) remained independently associated with a lower risk of aneurysm rupture, similarly as with lower tortuosity. Similar risk factors were observed in the patients with anterior circulation aneurysms, however, in terms of BA, no significant risk factors for aneurysm rupture were found (Figure 1).
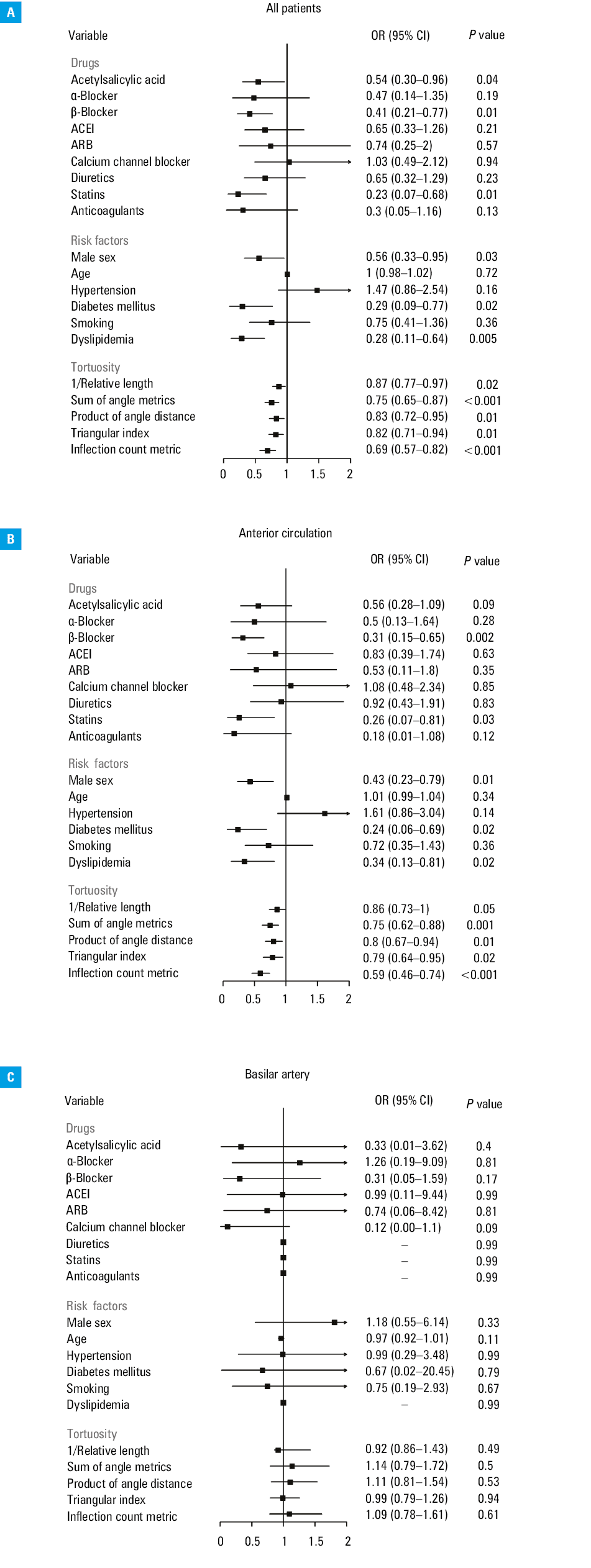
The effect of medications
We found that the patients who took acetylsalicylic acid (OR, 0.49; 95% CI, 0.28–0.83; P = 0.01), β-blockers (OR, 0.42; 95% CI, 0.24–0.71; P = 0.001), and statins (OR, 0.21; 95% CI, 0.08–0.46; P < 0.001) were significantly less likely to have ruptured aneurysm. In a multivariable analysis of all patients, after adjustment for risk factors, the use of each of the forementioned drugs was independently associated with a lack of aneurysm rupture. However, in the patients with anterior circulation aneurysms, only previous intake of β-blockers (OR, 0.37; 95% CI, 0.19–0.67; P = 0.002) and statins (OR, 0.2; 95% CI, 0.11–0.68; P = 0.03) was significantly associated with the absence of rupture. Also, we found no significant association between any medications and the BA aneurysm rupture. After additional adjustments for other medications, β-blockers (OR, 0.49; 95% CI, 0.24–0.95; P = 0.04) and statins (OR, 0.3; 95% CI, 0.08–0.94; P = 0.047) remained significantly associated with higher prevalence of unruptured aneurysm among all patients, however, in the patients with anterior circulation aneurysm we found such a relation only for β-blocker intake (OR, 0.39; 95% CI, 0.17–0.84; P = 0.02) (Table 2).
All patients (n = 334) | Anterior circulation (n = 274) | Basilar artery (n = 60) | ||||
OR (95% CI) | P value | OR (95% CI) | P value | OR (95% CI) | P value | |
Abbreviations: OR, odds ratio; others, see Table 1 | ||||||
Unadjusted | ||||||
Acetylsalicylic acid | 0.49 (0.28–0.83) | 0.01 | 0.53 (0.28–0.96) | 0.04 | 0.5 (0.13–1.74) | 0.29 |
α-Blockers | 0.62 (0.2–1.63) | 0.37 | 0.76 (0.21–2.2) | 0.64 | 0.29 (0–2.41) | 0.3 |
β-Blockers | 0.42 (0.24–0.71) | 0.001 | 0.37 (0.19–0.67) | 0.002 | 0.92 (0.27–3.08) | 0.89 |
ACEIs | 0.64 (0.37–1.08) | 0.1 | 0.83 (0.44–1.49) | 0.53 | 0.24 (0.06–0.83) | 0.03 |
ARBs | 0.67 (0.24–1.64) | 0.41 | 0.49 (0.11–1.51) | 0.26 | 0.93 (0.16–5.41) | 0.93 |
Calcium channel blockers | 0.87 (0.44–1.63) | 0.66 | 1.04 (0.5–2.06) | 0.91 | 0.6 (0.07–3.88) | 0.59 |
Diuretics | 0.58 (0.31–1.06) | 0.08 | 0.85 (0.43–1.61) | 0.63 | 0.09 (0.01–0.53) | 0.03 |
Statins | 0.21 (0.08–0.46) | <0.001 | 0.3 (0.11–0.68) | 0.01 | – | – |
Anticoagulants | 0.3 (0.05–1.09) | 0.11 | 0.2 (0.01–1.02) | 0.12 | 0.93 (0.04–24.36) | 0.96 |
Mutually adjusted | ||||||
Acetylsalicylic acid | 0.7 (0.36–1.33) | 0.29 | 0.72 (0.33–1.49) | 0.38 | 0.3 (0.02–3.33) | 0.33 |
α-Blockers | 0.49 (0.14–1.48) | 0.23 | 0.51 (0.12–1.79) | 0.32 | 0.15 (0–2.9) | 0.26 |
β-Blockers | 0.49 (0.24–0.95) | 0.04 | 0.39 (0.17–0.84) | 0.02 | 1.17 (0.09–19.25) | 0.9 |
ACEIs | 0.7 (0.32–1.51) | 0.37 | 0.88 (0.37–2.06) | 0.78 | – | – |
ARBs | 0.78 (0.23–2.42) | 0.67 | 0.67 (0.13–2.68) | 0.59 | – | – |
Calcium channel blockers | 1.12 (0.51–2.44) | 0.77 | 1.06 (0.45–2.46) | 0.89 | – | – |
Diuretics | 0.69 (0.32–1.4) | 0.31 | 0.97 (0.44–2.12) | 0.95 | – | – |
Statins | 0.3 (0.08–0.94) | 0.05 | 0.36 (0.09–1.26) | 0.12 | – | – |
Anticoagulants | 0.6 (0.09–2.53) | 0.53 | 0.34 (0.02–2.14) | 0.34 | – | – |
Discussion
We found that the patients whose intracranial aneurysms did not rupture were more likely to have been treated with β-blockers and statins than those who experienced subarachnoid bleed. This was true before and after adjustment for possible confounders, including the use of other antihypertensive medications. The overall outcome was driven by a protective effect in the anterior part of the cerebral circulation, that is, where most aneurysms occur. No other antihypertensive medications, including ACEIs, ARBs, diuretics, or calcium channel blockers, showed a similar association with the fate of intracranial aneurysms. Similarly, we found that the use of acetylsalicylic acid is related to a lower risk of ruptured aneurysm, however, this may be due to confounding by indication, as antiplatelet medications are routinely used prior to stent implantation into freshly‑diagnosed and unruptured aneurysms.
Despite possible adverse effects,13 β-blocker use is currently recommended in patients with aortic aneurysms, both in initial management and after surgery.14 Positive influence of these medications was shown especially in patients with Marfan syndrome, in whom β-blockers reduced aortic root growth and cardiovascular end points (aortic regurgitation, dissection, surgery, heart failure, or death) as well as improved overall survival.15 The performance of β-blockers was also analyzed in patients without Marfan syndrome, where they were shown to reduce aneurysm growth.16 However, some clinical trial reports failed to demonstrate significant protective effect of β-blockers on growth and risk of rupture in aortic aneurysms.16 Statins were also shown to reduce the growth of aortic aneurysms, a risk of their rupture, and perioperative mortality.17 Valença10 put forth an idea that β-blockers and statins could be beneficial in patients with intracranial aneurysms. While some authors demonstrated such an effect for statins, others reported conflicting results,7 and data concerning the impact of β-blockers on the risk of SAH have been inconclusive.9 To the best of our knowledge, no study so far has demonstrated a protective effect of β-blockers, the favorable action of which has only been proved in post‑SAH patients.18
β-Blockers act by lowering blood pressure, slowing heart rate and, in the case of such compounds as nebivolol, increasing NO synthesis in blood vessel walls.19 It has been demonstrated that the effect of β-blockers on blood pressure differs between the peripheral (brachial artery) and central (ascending aorta, common carotid artery) systemic circulatory regions. This stiffness‑related difference was further shown to possibly impact mean cerebral blood flow velocity, as assessed with transcranial Doppler ultrasound.20 Paradoxically, the antihypertensive drug classes providing a more uniform blood pressure reduction, both in the central and peripheral segments of the systemic circulation, might not decrease cerebral blood flow velocity enough to mechanically protect from the aneurysm rupture.
Our study replicated earlier findings that statin intake might offer benefits for patients with intracranial aneurysm.21 This is most likely related to pleiotropic effects of statins, such as anti‑inflammatory protection and decreased expression of macrophage chemoattractants and antivascular remodeling factors including metalloproteinases (MMPs).21 Indeed, MMP‑2 and MMP‑9 are overexpressed in intracranial aneurysm wall.22 β-Blockers may also modulate inflammatory responses. In patients with dilated cardiomyopathy, treatment with β-blockers decreases expression of interleukin (IL)-10, tumor necrosis factor α (TNF-α), and soluble receptors for TNF (sTNF‑R1 and R2).23 In patients with heart failure, β-blockers were shown to decrease circulating chemotaxis factors, inflammatory cytokines such as IL‑6, and to alter leukocyte distribution.24 Additionally, β-blockers induce the release of endothelin, a potent vasoconstrictor in all arterial circulatory regions, including the cerebral region.25
We found that the relationships between a history of β-blocker use and fate of aneurysm is restricted to the anterior part of the cerebral circulation. The posterior cerebral circulation is characterized by lower blood flow26 than the anterior circulation and less sympathetic innervation,27 which may weaken the influence of β-blockers. Also, due to different hemodynamic characteristics of the basilar artery and the arteries of the anterior circulation, they might differ in susceptibility to wall shear stress changes and arterial wall damage.28
In conclusion, in the case of an aneurysm located in the anterior cerebral circulation, but not in the BA, the use of β-blockers and statins was significantly more common among patients with unruptured aneurysms.
Our results need to be considered in the context of possible limitations. First, our study is a post hoc analysis of a retrospective group of acutely admitted patients, in whom the doses of medications, duration, and adherence to therapy were unknown. Moreover, we could not access the preadmission blood pressure values. On the other hand, blood pressure may change abruptly during severe acute headache, which was the reason for evaluation for possible SAH. This fact precludes usefulness of blood pressure values in the analyses such as ours. In consequence, we decided that the information on the history of hypertension would be used as a proxy for blood pressure. Second, our group of 334 patients is moderate in size, and we had too few cases of ruptured aneurysms for MCA alone to apply logistic models. On the other hand, our study is the first one that demonstrates an association of the history of β-blocker and statin intake with the absence of aneurysm rupture.
- Ingall T, Asplund K, Mähönen M, Bonita R. A multinational comparison of subarachnoid hemorrhage epidemiology in the WHO MONICA stroke study. Stroke. 2000; 31: 1054‑1061. | Crossref
- Stegmayr B, Eriksson M, Asplund K. Declining mortality from subarachnoid hemorrhage: changes in incidence and case fatality from 1985 through 2000. Stroke. 2004; 35: 2059‑2063. | Crossref
- Nieuwkamp DJ, Setz LE, Algra A, et al. Changes in case fatality of aneurysmal subarachnoid haemorrhage over time, according to age, sex, and region: a meta‑analysis. Lancet Neurol. 2009; 8: 635‑642. | Crossref
- van Gijn J, Kerr RS, Rinkel GJ. Subarachnoid haemorrhage. Lancet. 2007; 369: 306‑318. | Crossref
- Thompson BG, Brown RD Jr, Amin‑Hanjani S, et al. Guidelines for the management of patients with unruptured intracranial aneurysms: a guideline for healthcare professionals from the American Heart Association / American Stroke Association. Stroke. 2015; 46: 2368‑2400. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION