Treatment of the most difficult-to-cure hepatitis C virus–infected population with sofosbuvir / velpatasvir
1* ,
Key words: direct-acting antivirals, hepatitis C virus, negative predictor, pangenotypic treatment, sustained virologic response
,
Key words: direct-acting antivirals, hepatitis C virus, negative predictor, pangenotypic treatment, sustained virologic response



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Treatment of the most difficult-to-cure hepatitis C virus–infected population with sofosbuvir / velpatasvir
Introduction: Pangenotypic therapies for infections with hepatitis C virus (HCV), although universal and highly effective, entail a risk of treatment failure.
Objectives: Our study aimed to identify the population of HCV‑infected patients most difficult to cure with the sofosbuvir / velpatasvir (SOF/VEL) regimen.
Patients and methods: The effectiveness of the SOF/VEL regimen with a possible addition of ribavirin (RBV) was evaluated in populations known to be less responsive to treatment, and then in a population characterized by the combination of all factors impairing effectiveness, comprising patients treated with this regimen in the EpiTer‑2 multicenter retrospective study.
Results: A total of 2267 patients were treated with SOF/VEL±RBV. Of those, 2078 (96.4%) achieved sustained virologic response. The cure rate was 93.5% among 646 patients infected with genotype (GT) 3, 92.3% among 635 patients with cirrhosis, 95.5% in a population of 1233 men, and 94.1% among 421 patients with body mass index (BMI) above 30. An analysis in a group of 43 men with cirrhosis and obesity infected with GT3 showed the effectiveness of pangenotypic therapy at only 79.1%, falling to 66.7% in individuals with previous treatment failure.
Conclusions: In a large population of SOF/VEL‑treated HCV‑infected patients, we showed relatively low effectiveness of the regimen in treatment‑experienced men with cirrhosis and obesity, infected with GT3. Triple therapy should be considered when initiating the treatment of HCV infections in this group, which, however, needs to be confirmed in further studies. Previous studies were conducted in less demanding populations, because they did not take into account sex and BMI, which significantly affect the treatment effectiveness.
What's new?
Our study aimed to identify negative predictors that most significantly reduce the chances of successful therapy with a pangenotypic sofosbuvir / velpatasvir regimen in patients with chronic hepatitis C virus infection in real‑world clinical practice. Using retrospective data from the multicenter EpiTer‑2 study, we demonstrated that despite a very high overall response rate of 96.4%, the combination of male sex, genotype 3 infection, cirrhosis, obesity, and nonresponse to previous therapy lowers the chances of cure to 67%.
Introduction
A revolution in the treatment of chronic hepatitis C virus (HCV) infection that took place in the last decade thanks to the introduction of direct‑acting antivirals (DAAs) improved cure rates to over 95%.1 With such a dramatic increase in effectiveness, labeling some patient populations as difficult‑to‑treat no longer seems valid. This change was one of the factors that made it possible to achieve the goal set by the World Health Organization of eliminating HCV infections as a public health threat.2,3
In the era of interferon (IFN)-based regimens, the term difficult‑to‑treat was used to describe patients with cirrhosis, those who failed previous therapy, coinfected with HIV, and patients with renal failure, or other severe comorbidities.4 There were various reasons for lower effectiveness of the therapy. They consisted of its unfavorable safety profile with frequent side effects resulting in dose reduction or even treatment discontinuation, as well as problems with treatment access and a lack of patient adherence. The latter was of particular importance in the patients with HIV and those addicted to drugs or alcohol.5,6 The lower response rate of IFN therapy was also noted in patients infected with genotype (GT) 1 and GT4, as compared with GT2 and GT3.7 Male sex, older age, and high body mass index (BMI) were also negative predictors of therapeutic success.8,9 These difficulties have been overcome in the era of DAAs, especially with the introduction of highly potent pangenotypic regimens, but still, a success rate of more than 95% does not mean that every patient can be cured.10,11 Although the failure rate is incomparably smaller than in the case of IFN‑based therapies, knowledge on the factors that reduce the chances of recovery is extremely important, also for planning rescue therapy.12-14
The aim of the current real‑world experience (RWE) analysis was to identify the HCV‑infected patient population most difficult‑to‑cure with the pangenotypic option of sofosbuvir / velpatasvir and possible addition of ribavirin (SOF/VEL±RBV). This term seems more appropriate than difficult‑to‑treat due to a very good safety profile of SOF/VEL‑based therapy. We identified individual negative predictors and also a combination of factors that most strongly affect effectiveness of this therapy.
Patients and methods
Study population
The analysis included patients selected from the EpiTer‑2 database, a large, retrospective, multicenter, national, real‑world study evaluating DAA treatment in 17 166 consecutive patients with HCV infection treated in 22 Polish hepatology centers from 2015 through 2022. As shown in Figure 1, a total of 5549 patients were treated with pangenotypic regimens. After excluding those lost to follow‑up, the population was limited to 5355 patients, which included 2267 individuals treated with SOF/VEL±RBV, in whom treatment effectiveness was assessed per‑protocol (PP). Further analysis included an assessment of populations considered most difficult‑to‑cure in terms of achievable effectiveness, followed by an analysis of populations with a combination of factors that worsen the treatment efficacy, as illustrated in Figure 1.
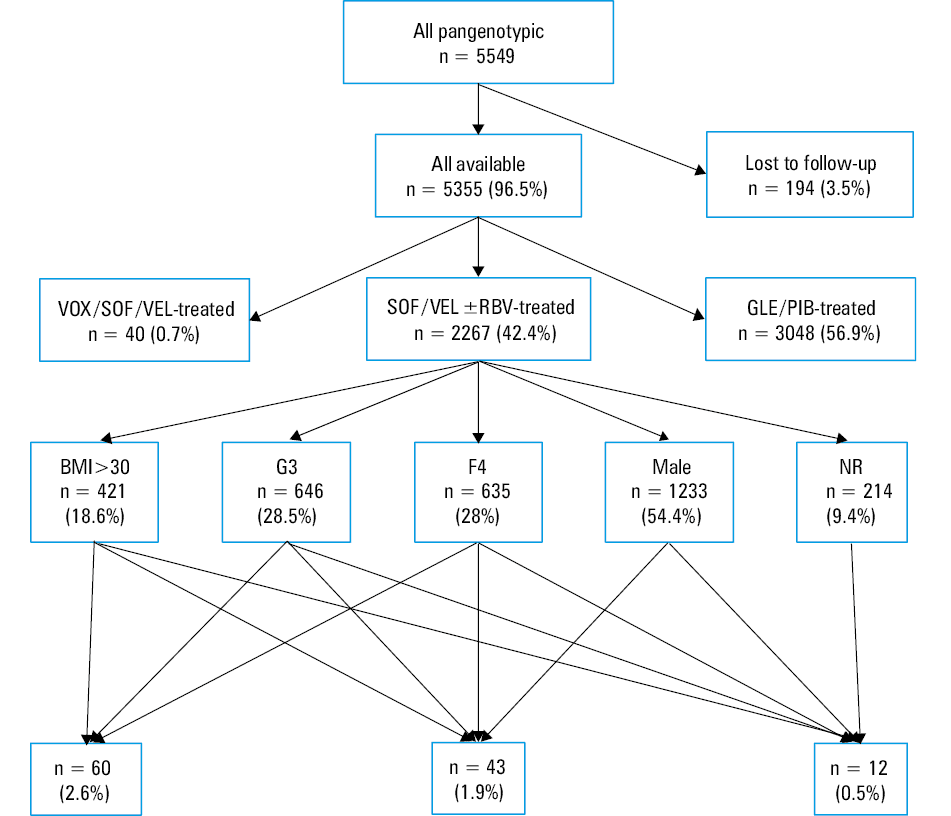
Abbreviations: BMI, body mass index; F, fibrosis; G, genotype; GLE, glecaprevir; NR, nonresponder; PIB, pibrentasvir; RBV, ribavirin; SOF, sofosbuvir; VEL, velpatasvir; VOX, voxilaprevir
A choice of the antiviral regimen, including retherapy, was made by the treating physicians based on current national recommendations15,16 and reimbursement policy of the National Health Fund (NHF). DAA doses and treatment duration were consistent with the Summary of Product Characteristics (SmPC).17 The patients provided their written informed consent before the start of the treatment, according to the ethical requirements of NHF. Since the EpiTer‑2 is a database that includes anonymized patient data collected retrospectively from the treatment records, the patient consent to participate in this study was waived due to its retrospective design.
Clinical and laboratory data
Clinical and laboratory data were collected retrospectively and entered into a platform operated by Tiba company (Wrocław, Poland), following the National General Data Protection Regulation in Poland.
The information captured at baseline included demographic and clinical data: age, sex, BMI, comorbidities and concomitant medications, severity of liver disease, hepatitis B virus (HBV) and HIV coinfections, and a history of previous antiviral treatment.
The degree of liver disease was evaluated noninvasively by transient elastography or shear‑wave elastography, or histologically by liver biopsy. The results were presented as per fibrosis (F) stage 0–4, according to the METAVIR score and the recommendations of the European Association for the Study of the Liver, with 13 kP as a threshold defining liver cirrhosis.18 The patients with cirrhosis were assessed with the Child–Pugh (CP) and Model of End‑Stage Liver Disease (MELD) scores. Laboratory parameters analyzed included the activity of serum alanine transaminase, the concentration of bilirubin, albumin, creatinine, and hemoglobin, white blood cell and platelet counts, and HCV viral load. HCV RNA was assessed by real‑time polymerase chain reaction assays at baseline, at the end of the treatment, and at least 12 weeks after therapy completion.
Statistical analysis
Therapy ffectiveness was assessed in the intent‑to‑treat analysis, which included patients who received at least 1 dose of DAA, but we focused mostly on the PP analysis that excluded the patients with nonvirologic failure. The analysis of possible drug interactions was based on the Interaction Checker tool provided online by the University of Liverpool.19
The results were expressed as median and interquartile range or number (percentage). A P value below 0.05 was considered significant. The significance of differences was calculated with the χ2 or the Fisher exact test (applied if the number of observations in any of the subgroups was <10). Furthermore, to better illustrate an association between the exposure (therapy) and outcome (sustained viral response [SVR]), odds ratios with 95% CIs were calculated. Statistical analyses were performed with GraphPad Prism 5.1 software (GraphPad Software, Inc., La Jolla, California, United States).
Results
Characteristics of the study population
A majority of patients in the analyzed group were men at a median age of over 50 years (Table 1). They were predominantly infected with GT1 (60.3%) and GT3 (30.1%). Advanced liver disease (F3 or F4) was diagnosed in 43% of the patients, more than two‑thirds were the cases of cirrhosis. However, only 5% of the patients scored B or C on the CP scale, only 2.6% had MELD score above 15, 4.5% had a history of decompensation, and 1.5% had a history of hepatocellular carcinoma (Table 1). HIV coinfection was found in 13% and HBV in 17% of the patients. Over 90% were treatment‑naive individuals, and most of those who failed the previous therapy were relapsers after undetectable HCV RNA at the end of treatment.
Parameter | Value | |
Data are presented as median (IQR) or number (percentage) of patients.
SI conversion factors: to convert ALT to μkat/l, multiply by 0.0167.
Abbreviations: ALT, alanine transaminase; HBV, hepatitis B virus; HCC, hepatocellular carcinoma; HCV, hepatitis C virus; IQR, interquartile range; MELD, Model of End‑Stage Liver Disease; others, see Figure 1 | ||
Age, y | 50 (40–62) | |
Sex, women / men | 961 (42.4)/ 1306 (57.6) | |
BMI, kg/m2 | 26.1 (23.2–29) | |
Genotype | 1 | 46 (2) |
1a | 128 (5.7) | |
1b | 1236 (54.6) | |
2 | 16 (0.7) | |
3 | 681 (30.1) | |
4 | 158 (7) | |
Fibrosis / stiffness | F0 | 39 (1.7) |
F1 | 760 (33.5) | |
F2 | 430 (19) | |
F3 | 314 (13.9) | |
F4 | 660 (29.1) | |
Unknown | 64 (2.8) | |
Nonresponders | Overall | 222 (9.8) |
Null‑response | 45 (20.3) | |
Relapse | 128 (57.7) | |
Unknown type of nonresponse | 28 (12.6) | |
Discontinuation due to safety reason | 21 (9.5) | |
Characteristics of previous therapy | Interferon‑based | 114 (51.4) |
Interferon‑free | 108 (48.6) | |
Child–Pugh B or C | 111 (4.9) | |
MELD score >15 | 58 (2.6) | |
Decompensation history | 101 (4.5) | |
HCC history | 34 (1.5) | |
Liver transplantation history | 7 (0.3) | |
HIV coinfection | 301 (13.3) | |
HBV coinfection | 380 (16.8) | |
HCV RNA, IU/l | 1.26 (0.36–3.16) | |
ALT, IU/l | 67.8 (41–115) | |
More than 92% of the patients received SOF/VEL treatment for 12 weeks, but in 7.1% of the cases RVB was added (Table 2).
Parameter | Value | |
Abbreviations: EOT, end of therapy; ITT, intent‑to‑treat; n, number of patients meeting the criterion; N, number of patients in whom the parameter was evaluated; PP, per‑protocol; SVR, sustained virologic response; others, see Figure 1 | ||
Current therapy, n (%) | SOF/VEL for 12 weeks | 2092 (92.3) |
SOF/VEL for 24 weeks | 15 (0.7) | |
SOF/VEL+RBV for 12 weeks | 113 (5) | |
SOF/VEL+RBV for 24 weeks | 47 (2.1) | |
EOT response PP, n/N (%) | 2040/2192 (93.1) | |
EOT response ITT, n/N (%) | 2040/2254 (90.5) | |
SVR PP, n/N (%) | 2078/2155 (96.4) | |
SVR ITT, n/N (%) | 2078/2267 (91.7) | |
Treatment effectiveness and negative predictors
HCV RNA was undetectable at the end of treatment in 93.1%, and SVR was achieved in 96.4% of the patients (Table 2). In the populations burdened with individually analyzed factors worsening the effectiveness of treatment, the lowest SVR, not exceeding 90%, was found in the patients who had failed previous therapy. In the remaining groups, the SVR ranged from 92.3% in the patients with cirrhosis to 95.5% in men (Table 3; Supplementary material, Figure S1). A comparison of the most difficult‑to‑cure patients and the corresponding groups of the easiest‑to‑cure, in which the SVR always exceeded 97%, showed significant differences (Table 3; Supplementary material, Figure S2).
Parameter | SVR, n/N (%) | P value | OR | 95% CI | |
Values were compared using the Fisher exact test.
| |||||
Sex | Men | 1178/1233 (95.5) | 0.01 | 0.52 | 0.32–0.86 |
Women | 97.6 (900/922) | ||||
BMI | >30 kg/m2 | 396/421 (94.1) | 0.006 | 0.49 | 0.3–0.8 |
≤30 kg/m2 | 1682/1734 (97) | ||||
Genotype | GT3 | 604/646 (93.5) | <0.001 | 0.34 | 0.22–0.54 |
Non‑GT3 | 1474/1509 (97.7) | ||||
Fibrosis | F4 | 586/635 (92.3) | <0.001 | 0.20 | 0.12–0.33 |
Non‑F4 | 1438/1462 (98.4) | ||||
NR | 192/214 (89.7) | <0.001 | 0.25 | 0.15–0.42 | |
NAI | 1837/1890 (97.2) | ||||
BMI >30/GT3/F4 | 51/60 (85) | <0.001 | 0.09 | 0.04–0.23 | |
BMI ≤30/non‑GT3/non‑F4 | 843/857 (98.4) | ||||
BMI >30/GT3/F4/Male | 34/43 (79.1) | <0.001 | 0.05 | 0.02–0.16 | |
BMI ≤30/non‑GT3/non‑F4/Female | 367/372 (98.7) | ||||
BMI >30/GT3/F4/Male/NR | 8/12 (66.7) | <0.001 | 0.02 | 0–0.11 | |
BMI ≤30/non‑GT3/non‑F4/Female/NAI | 338/342 (98.8) | ||||
The patients with a combination of worsening factors accounted for less than 2.6% of the whole study group. The analysis carried out in a group of 60 cirrhotic and obese patients infected with GT3 confirmed 85% effectiveness of SOF/VEL±RBV, but after limiting this group to men only, the effectiveness decreased to 79.1%, and after taking into account nonresponders to previous therapies, it further decreased to 66.7% (Table 3; Supplementary material, Figure S1). Differences in the effectiveness of treatment as compared with the populations of patients not burdened with factors worsening the prognosis were significant (Table 3). Adding RBV to the SOF/VEL regimen in the populations where it is considered beneficial (compensated cirrhosis and GT3) or recommended (decompensated cirrhosis) according to SmPC, did not improve the effectiveness of SOF/VEL therapy.
We also analyzed the characteristics of 4 theoretically treatable women who did not respond to treatment despite no failure of previous therapy, were not obese, had mild liver stiffness, and were infected with non‑GT3 (Table 4). We detected potential factors negatively affecting the effectiveness of therapy in only 2 women. In one of them (NS) it was discontinuation of therapy in the 4th week due to pregnancy, and in the other (EK) the use of omeprazole.
Parameter | Patient initials | |||
KW | NS | EK | EJ | |
SI conversion factors: to convert albumin to g/l, multiply by 10; ALT to µkat/l, by 0.0167; bilirubin to µmol/l, by 17.104; hemoglobin to g/l, by 10; creatinine to µmol/l, by 88.4.
| ||||
Age, y | 46 | 31 | 70 | 58 |
Genotype | 4 | 1B | 1B | 1B |
Regimen | SOF/VEL, 12 weeks | SOF/VEL, 12 weeks | SOF/VEL, 12 weeks | SOF/VEL, 12 weeks |
Previous treatment | No | No | No | No |
Liver stiffness, kPa | 6.2 | 7.1 | 6 | 5.5 |
History of decompensation | No | No | No | No |
History of HCC | No | No | No | No |
Extrahepatic manifestations | No | No | No | No |
HBV coinfection | No | No | No | No |
HIV coinfection | No | No | No | No |
Comedication | Tramadol, paracetamol | – | Bisoprolol, omeprazole, spironolactone | Valsartan, hydrochlorothiazide, amlodipine |
Possible interactions | No | – | Possible with omeprazole | No |
Comorbidities | Back pain syndrome | – | Hypertension | Hypertension |
HCV RNA, IU/ml | 542 000 | 500 000 | 801 603 | 713 000 |
ALT, IU/l | 72 | 46 | 10 | 30 |
Albumin, g/dl | 4.4 | 4.9 | 4.7 | 4 |
Bilirubin, mg/dl | 0.9 | 0.47 | 1.05 | 0.3 |
Hemoglobin, g/dl | 15.7 | 14.5 | 10 | 14.7 |
Platelets, × 103/µl | 225 | 211 | 169 | 200 |
Creatinine, mg/dl | 0.8 | 0.69 | 0.73 | 0.57 |
INR | 0.95 | 0.89 | 1.17 | 1 |
BMI | 23.3 | 17.7 | 21.2 | 28.4 |
Treatment discontinuation | No | In 4th week due to pregnancy | No | No |
HCV RNA at the end of treatment | Detectable | Not done | Detectable | Not detectable |
Discussion
Although the overall efficacy of pangenotypic DAA options is very high, there is still a small percentage of patients with chronic HCV infection who do not respond to this treatment. We decided to look more closely at this group of nonresponders, to determine not only individual factors, but also a combination of negative predictors of treatment effectiveness. We did not compare the 2 available first‑line pangenotypic regimens, because our study was a retrospective one and did not guarantee equal population matching due to preselection resulting from different and changing labels, drug program requirements, and option selection to avoid the risk of drug‑drug interactions. We focused on the SOF/VEL±RBV combination registered for use in patients with chronic hepatitis C at any stage of liver disease, including decompensated cirrhosis.20-23
In our study population, the patients with cirrhosis accounted for over 29%, and this historical negative predictor of therapy effectiveness from the IFN era also significantly reduced the SVR rate of patients treated with SOF/VEL±RBV. Those with cirrhosis responded to treatment in 92.3%, as compared to SVR of 98.4% in the noncirrhotic individuals. This effectiveness was lower than that of 96% reported by Asselah et al,24 who assessed the cure rate in a group of cirrhotic patients participating in 3 phase 3 registration clinical trials (ASTRAL‑1, 2, and 3). However, it should be noted that these studies included only individuals with compensated cirrhosis, while in our analysis 17% of the cirrhotic patients were diagnosed with decompensation at baseline. The ASTRAL‑4 clinical trial dedicated to this patient population documented an overall SVR rate of 88%; being 83% and 86% after 12- and 24‑week SOF/VEL therapy, respectively, while the addition of RBV increased this percentage to 94%.21 We cannot comment on this, because in our study we did not evaluate the role of RBV as a factor affecting the therapy effectiveness.
According to the SmPC, the addition of RBV should also be considered in patients with compensated cirrhosis infected with GT3, although data from both clinical trials and RWE cohorts are inconclusive in this area.17,25-29 This recommendation stems from a search for opportunities to increase the efficacy of therapy in cirrhotic patients infected with GT3, which in our study was found to be another negative predictor of SVR, lowering the cure rate to 93% vs 98% in non‑GT3 infections. The patients burdened with these 2 negative predictors, cirrhosis and GT3 infection, evaluated in the ASTRAL‑3 clinical study, responded in 91%, while the POLARIS‑3 study showed a much higher (96%) success rate in this population with the SOF/VEL regimen.22,30 The range of SVR obtained in such patients in RWE studies is also wide, from 87% to over 99%, depending on the characteristics of the population.27,29,31-35 In our analysis, we evaluated these 2 unfavorable parameters combined with another negative predictor identified using the test of statistical significance, which turned out to be obesity defined as BMI above 30. The effectiveness achieved in such a patient population was 85%. It is worth recalling that in the era of IFN‑based therapies, obesity was considered one of the factors that reduced SVR.36 It is difficult to compare our results with those of other researchers, as reports from the DAA era considering the effect of BMI on the SVR of this parameter are scarce. To the best of our knowledge, only 3 papers, including 2 conference reports, have evaluated the impact of obesity on SVR.37-39 Two of them documented no effects, but 1 analysis did not include GT3‑infected patients at all, and the other included only 3 such patients. Moreover, the group sizes were small (188 and 168 individuals, respectively), and both studies concerned different DAA regimens.37,38 In contrast, an analysis of a much larger population of 1492 patients treated with the sofosbuvir / ledipasvir regimen, presented in the form of a conference report, showed that patients with a high BMI had a higher risk of treatment failure.39 That study also confirmed an increased risk of nonresponse in cirrhotic and male patients. This is in line with the results of our analysis, as it was the male sex that was another identified negative predictor of SVR. Obese men with cirrhosis in the course of GT3 infection responded to SOF/VEL‑based therapy in 79%. The impact of male sex on the odds of response to DAA therapies, including the SOF/VEL option, has been evaluated in numerous RWE analyses supporting our findings.11,40-42
Finally, the list of factors that reduce the chances of successful SOF/VEL therapy established in the current study is closed by a failure of previous treatment. Adding it to the combination of previously‑described negative predictors lowered the cure rate to 67%. This is a well‑known parameter associated with a significantly worse virologic response in the IFN era, while data from the DAA era, coming from both clinical trials and RWE studies, are inconsistent.24,32,41,43,44 Reports on SOF/VEL therapy in previously treated patients with cirrhosis caused by GT3 infection also indicate a wide range of virologic response rates. In the ASTRAL‑3 trial, the SVR of 89% was achieved in this patient population, while in a nationwide RWE Italian study evaluating the SOF/VEL regimen, such patients responded in as much as 96%.22,34 Only 75% SVR was reported in GT3‑infected patients with failure of previous therapy in the RWE cohort from Canada, but the presence of cirrhosis was not included in this analysis, so it is reasonable to expect that this value could be even lower.33
However, not only individuals with identified negative predictors did not respond to SOF/VEL‑based treatment in our study. We took a closer look at the characteristics of 4 theoretically treatable female patients who did not respond to treatment despite not having failed prior therapy, not being obese, with liver stiffness corresponding to mild fibrosis, and infected with non‑GT3. Among the factors that may have contributed to the lack of response was discontinuation of therapy due to pregnancy at week 4 in 1 of the patients, and concomitant use of omeprazole in another woman. It should be mentioned that although data from the literature recommend caution in patients taking proton pump inhibitors while receiving SOF/VEL due to possible drug‑drug interactions, there is no clear evidence of a significant effect of these drugs on treatment success.45 In the remaining 2 patients, we did not find any factors that could reduce their chances of response to treatment. This suggests that other variables may be involved, which we were unable to determine in our analysis, and which is one of its limitations. Other limitations that we are aware of are due to the observational nature and retrospective design of the study, and include possible bias, missing some data, and value entry errors. We did not collect objective data confirming adherence to the therapy, and we relied only on patients’ declarations in this regard. We also did not evaluate the presence of resistance‑associated substitutions before treatment, but according to published data documenting the high barrier to resistance of the SOF/VEL‑based regimen, this does not affect the effectiveness of the therapy.32,46 The strongest point of our study is the collection of data from a heterogeneous cohort representative of routine clinical practice.
Conclusions
In a large real‑world population of HCV‑infected patients treated with SOF/VEL±RBV, despite a high overall cure rate exceeding 96%, we demonstrated a relatively low effectiveness of the therapy in treatment‑experienced men with obesity and cirrhosis, and infected with GT3. In this small, difficult‑to‑cure population constituting less than 2.6% of the whole study group, triple pangenotypic therapy should be considered as the first‑line management. However, this needs to be confirmed in further studies. This strategy was evaluated in a population of cirrhotic patients infected with GT3 in the POLARIS‑3 trial, but without taking into account sex and BMI, which significantly affect efficacy.
- Brzdęk M, Zarębska‑Michaluk D, Invernizzi F, et al. Decade of optimizing therapy with direct‑acting antiviral drugs and the changing profile of patients with chronic hepatitis C. World J Gastroenterol. 2023; 29: 949‑966. | Crossref
- World Health Organization. Fact‑sheets on Hepatitis C. Published June 24 2022. https://www.who.int/news‑room/fact‑sheets/detail/hepatitis‑c. Accessed, July 4, 2023.
- Flisiak R, Frankova S, Grgurevic I, et al. How close are we to hepatitis C virus elimination in Central Europe? Clin Exp Hepatol. 2020; 6: 1‑8. | Crossref
- Hilgenfeldt EG, Schlachterman A, Firpi RJ. Hepatitis C: treatment of difficult to treat patients. World J Hepatol. 2015; 7: 1953‑1963. | Crossref
- Afdhal NH. Hepatitis C viral infection in difficult‑to‑treat populations: an overview. Clin Liver Dis (Hoboken). 2012; 1: 63‑64. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION